






記住我








CAD is a common cardiovascular disease, which is commonly caused by atherosclerotic plaques. Coronary artery plaque rupture triggers platelet adhesion to exposed sub-endothelial matrix proteins, platelet activation, and platelet aggregation, which might cause severe ischemic events (1). Antiplatelet therapy is a powerful strategy for preventing thrombosis and ischemic events. Dual antiplatelet therapy (DAPT), composed of oral P2Y12 receptor antagonist and aspirin, is an important component of secondary prevention for CAD patients. By virtue of lower bleeding risk (2, 3) and fewer adverse effects, clopidogrel is still indispensable in the era of emerging novel P2Y12 receptor antagonists. Clopidogrel is recommended for application in patients suffering from stable coronary artery disease (SCAD) (4, 5). Many factors affect the pharmacodynamics of clopidogrel, such as genetic factors, drug-drug interaction, and biological and clinical factors (6). A notable proportion of CAD patients using clopidogrel therapy present HRPR and are more likely to experience adverse events after percutaneous coronary intervention (PCI) (7).
Elevated FFAs is often observed among patients with metabolic abnormalities, such as diabetes mellitus, obesity, hypertension, and so on (8, 9). Metabolic abnormalities are proven risk factors for CAD (10), some of which were found to be associated with HRPR (11, 12). FFAs is also a biomarker for coronary artery thrombosis (13, 14), and is associated with the occurrence, severity, and poor prognosis of CAD (15–17). Whether FFAs affect clopidogrel's pharmacodynamics remained unclear. We conducted a cross-sectional study by collecting clinical information from CAD patients scheduled for elective PCI. The aim is to detect whether FFAs affect ADP-induced platelet reactivity in CAD patients receiving clopidogrel and evaluate the predictive value of FFAs for HRPR.
2. Method 2.1. Study design and populationBased on a prospectively collected database, we conducted a cross-sectional study to assess whether FFAs affects residual platelet reactivity while receiving clopidogrel therapy. This research consecutively enrolled 1,380 SCAD patients who underwent elective PCI from January 2019 to December 2019. All patients had available FFAs measurements and had received guideline-recommended preoperative clopidogrel therapy [maintenance dose (75 mg, once daily) for at least five days prior to PCI or loading dose (300 mg) of clopidogrel at least 12 h prior to PCI]. The exclusion criteria included: (1) incomplete baseline data, (2) receiving other P2Y12 inhibitors besides clopidogrel, (3) intolerance of DAPT consisting of aspirin and clopidogrel (such as drug allergy and BARC ≥ 3 bleeding events), (4) platelet count (PLT) > 400 or < 50 × 109/L, (5) severe renal or hepatic impairment [estimated glomerular filtration rate (eGFR) < 30 ml/min/1.73 m2 and/or alanine aminotransferase (ALT) > 2.5 times the normal upper limit], (6) other life-threatening diseases such as cancer.
2.2. Demographic, clinical, and laboratory informationPatients' information were documented by trained data collectors from electronic medical record system without knowledge of the current study's protocol. Demographic information included age and gender. Clinical data collected included heart rate, systolic and diastolic blood pressure, smoking status, body mass index (BMI), and medical history of hypertension, diabetes, dyslipidemia, and previous coronary revascularization (percutaneous or surgical). Current smoker was defined as self-reported regular tobacco use in the last 3 months. Hypertension was diagnosed based on a previous hypertension diagnosis, using an anti-hypertensive medication, or resting blood pressure ≥140/90 mmHg. Dyslipidemia was defined as having a previous diagnosis, currently undergoing lipid-lowering therapy, or having low-density lipoprotein cholesterol (LDL-C) > 4.1 mmol/L and/or high-density lipoprotein cholesterol (HDL-C) < 1.0 mmol/L and/or total cholesterol (TC) > 6.2 mmol/L and/or triglyceride (TG) > 2.3 mmol/L. Diabetes was defined as a self-reported previous diagnosis, receiving glucose-lowering therapy, or a new diagnosis based on current guidelines (18). Besides these, we collected laboratory measurements, including FFAs, routine blood indicators [white blood cell count (WBC), PLT, and hemoglobin (Hb)], liver function indicators [albumin (ALB), ALT, and aspartate aminotransferase (AST)], renal function indicators [creatinine and eGFR], fasting blood glucose (FBG), lipid indicators (TG, TC, HDL-C, and LDL-C), fibrinogen (FIB), uric acid (UA), high-sensitivity C-reactive protein (hs-CRP). eGFR was calculated using an online tool provided by Chronic Kidney Disease Epidemiology Collaboration (http://ckdepi.org/equations/gfr-calculator/). FFAs was measured using an automated biochemical analyzer with the enzymatic colorimetric method (Roche, COBAS 8000). To avoid the condition that FFAs is unable to efficiently reflect the abnormal metabolism due to interfering factors (such as physical activity, hunger state, and so on), blood samples were taken from the patient at a quiet state after 12 h of fasting. In addition, 768 patients among them had ever tested CYPC19*2, CYPC19*3, and CYPC19*17 alleles, and we collected these information by browsing the electronic medical record system.
2.3. Platelet function testingOn the first morning after PCI, nurses collected venous blood samples into vacutainer tubes containing lithium heparin and 3.2% trisodium citrate, and the thrombelastography (TEG) assay was carried out within 2 h using LEPU TEG System (CFMS, Beijing, China) to evaluate the efficacy of antiplatelet therapy. The ADP-induced thrombus formation process monitored by the TEG was reported as a series of coagulation parameters. Previous literature had described the detection principle in detail (19). The modified TEG system evaluated the effects of antiplatelet therapy action via the ADP and arachidonic acid pathways using four channels. The CFMS TEG system and automated analytical software measured the physical properties of clots. MAADP reflects the maximum intensity of ADP-induced clots consisting of fibrin and platelet in a heparinized whole blood sample. The maximum amplitude of thrombin-induced clot strength (MAthrombin) represented the aggregation capacity of platelet and fibrin induced by thrombin and the maximum amplitude of fibrin clot strength (MAfibrin) represented the aggregation capacity of only fibrin induced by reptilase and factor XIIIa. ADPi was used to assess clopidogrel's efficacy in blocking the ADP pathway to inhibit platelet aggregation, which was calculated as ADPi=MAADP−MAfibrinMAthrombin−MAFibrin. Based on current consensus (20) and previous studies conducted in China (21), we defined ADP-induced HRPR as ADPi < 50% plus MAADP > 47 mm in the current study.
2.4. Statistical methodsContinuous variables were expressed as the mean and standard deviation (SD) or the median and interquartile range (IQR) according to normal or non-normal distribution. Normality testing was performed using graphical methods and the Shapiro-Wilk test. Categorical variables were expressed as numbers and percentages (%). We presented baseline characteristics of patients with HRPR and non-HRPR. We used the Student's t-test, the Mann–Whitney test, or the chi-square test to compare differences between the two groups as appropriate. To compare residual platelet activity and other covariates among patients with high and low levels of FFAs, we additionally divided patients into two groups based on an FFAs level of 0.445 mmol/L. A receiver operating characteristic (ROC) curve was drawn to determine the optimum cut-off value (0.445 mmol/L) based on the Youden index. The exposure risk of FFA > 0.445 mmol/L was tested using a univariate logistic regression model and expressed as the odds ratio (OR) and 95% confidence interval (95% CI). To correct potential confounding factors, we constructed a series of multivariable logistic regression models in several stages. The choice of covariates was based on current statistical significance, previous literature, and clinical judgment. Model 1: adjusted for sex and age, Model 2: adjusted for the medical history of hypertension, diabetes, and previous PCI, current smoker, usage pattern of clopidogrel, and variables included in Model 1, and Model 3: adjusted for Hb, WBC, PLT, HDL-C, LDL-C, ALT, creatine, FIB, hs-CRP, and variables included in Model 2. Then, we performed subgroup analysis to test the stability of results and detect potential interaction. Interactions were tested by using an interaction test in logistic regression models. Furthermore, we additionally conducted sensitivity analyses using propensity score matching (PSM). Groups (HRPR and non-HRPR) were matched using 1:1 nearest neighbor-matching, within a caliper width of 0.2 of the standard deviation of the propensity score logit. The variables selected for the propensity score model included covariates in Model 3. In addition, we again conducted univariate and multivariable analyses among patients with the CYPC19 genotype and tested the stability of the results after adjusting for variables including clopidogrel's metabolizer status.
Statistical significance was determined with a 2-tailed P-value <0.05. SPSS Statistics 26.0 (SPSS, Inc., Chicago, IL, USA) was used for the statistical analysis.
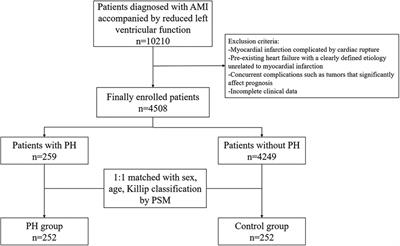
3. Results 3.1. Study populationAs shown by Figure 1, after careful screening, a total of 1,277 patients satisfied the inclusion and exclusion criteria and were enrolled in the current study, of which 486 patients (38.1%) showed HRPR. The mean age was 61.2 ± 9.5 years and 337 patients (26.4%) were female. Baseline information were complete. In Table 1, baseline characteristics were shown using stratification based on HRPR and non-HRPR. According to univariate comparison, patients with HRPR were older, and more frequently female. Patients with HRPR had a significantly higher proportion of diabetes and a significantly lower proportion of previous PCI. The proportion of using 300 mg loading clopidogrel or using daily 75 mg clopidogrel more than 5 days before PCI is balanced between groups. In terms of laboratory information, patients with HRPR had higher levels of FFAs (0.46 ± 0.22 vs. 0.41 ± 0.21, P < 0.001), PLT, HDL-C, LDL-C, FIB, FBG, and hs-CRP, and had lower levels of Hb, WBC, creatine, and eGFR. Additionally, we found CYPC19 genotype distributions between the two groups were different among 768 patients who had tested CYPC19*2, CYPC19*3, and CYPC19*17 alleles (Supplementary material S1, Table S1). The proportions of intermediate metabolizers and poor metabolizers are higher among patients with HRPR.
Figure 1. Inclusion and exclusion in the study population. SCAD, stable coronary artery disease; PCI, percutaneous coronary intervention; DAPT, Dual antiplatelet therapy; TEG, thromboelastography; PLT, platelet count; HRPR, high residual platelet reactivity.
Table 1. Baseline characteristics in patients with and without HRPR.
3.2. Platelet aggregation and other covariates among different levels of FFAsWe divided all patients included in the current study into two groups based on an FFAs level of 0.445 mmol/L. The cut-off point was determined by detecting the point with the optimum Youden index from the ROC curve (Supplementary Material S3). As shown in Table 2, patients with higher FFAs were more often female and had a significantly higher proportion of diabetes and hypertension. Besides these, patients with higher FFAs had higher levels of Hb, aminotransferase, lipid indicators, FBG, FIB, and hs-CRP, and lower creatine. Notably, there were significant differences in TEG parameters between groups with higher and lower FFAs. As shown in Figure 2, there existed higher MAADP and lower ADPi among patients with higher FFAs (the median value of MAADP: 46.3 [36.6, 53.6] vs. 41.4 [33.7, 49.95], P < 0.001; the mean value of ADPi: 34.21 ± 24.12 vs. 39.06 ± 23.06, P < 0.001), and the proportion of HRPR among patients with higher FFAs was larger (46.4% vs. 32.6%, P < 0.001).
Figure 2. ADP-induced platelet aggregation in different levels of FFAs. (A) ADP-induced platelet inhibition rate (ADPi), (B) the maximum amplitude of ADP-induced clot strength (MAADP) and (C) the frequency of HRPR in patients with different FFAs level.
Table 2. Platelet aggregation and other covariates among different levels of FFAs.
3.3. Effect of FFAs on residual platelet reactivityFFAs was recategorized as a dichotomous variable (FFAs > 0.445 and FFAs ≤ 0.445). To evaluate the effect of FFAs on ADP-induced residual platelet reactivity while using clopidogrel, we constructed univariable and multivariable logistic regression models including FFAs. As shown in Table 3, crude OR is 1.786 (1.419–2.250), which might suggest an association between higher FFAs and HRPR. As mentioned in the previous section, we constructed a series of multivariable logistic regression models to adjust for potential confounders and demonstrated higher FFAs as an independent factor associated with HRPR (model3: OR 1.745, 95%CI, 1.352–2.254). Besides this, we also found that age, female, higher PLT, lower Hb, lower WBC, higher ALT, and higher FBG were independently associated with HRPR.
Table 3. Univariable and multivariable logistic regression models.
3.4. Subgroup and sensitivity analysesAiming to test the stability of results, we additionally performed subgroup analyses based on age (≤65 years or >65 years), sex, diabetes, and PLT count (≤200 × 109 or >200 × 109). As shown in Figure 3, the association of FFAs with HRPR showed no significant interaction with sex, age, diabetes, and PLT count (all P-values for interaction >0.05). However, it was worth noting that higher FFAs lost its significant association with HRPR in the female (P = 0.402) and >65 years (P = 0.080) subgroup and the interaction between FFAs level and sex required attention (P = 0.114). After PSM, there were 415 matched patients in both groups. Based on the new population, we further test the stability of the results using univariable and multivariable logistic regression models (Supplementary Material S2), and higher FFAs remained a significant independent factor associated with elevated HRPR risk (Model 3: OR = 1.765, 95% CI, 1.319–2.360). Based on 768 patients who had tested CYPC19*2, CYPC19*3, and CYPC19*17 alleles, we again conducted univariable and multivariable logistic regression models. We found higher FFAs was still associated with the occurrence of HRPR after adjusting for potential confounders including metabolizer status (crude OR, 95%CI, 1.534 (1.136–2.073); adjusted OR, 95%CI, 1.522 (1.074–2.158), showed in Supplementary Material S1, Table S2).
Figure 3. Subgroup analysis. OR, Odds ratio; CI, Confidence interval; HRPR, high residual platelet reactivity; PLT, platelet count.
4. DiscussionThe current study was a cross-sectional study based on a prospectively-collected database. We detected the effect of higher FFAs on ADP-induced residual platelet activity among patients using clopidogrel, and we demonstrated higher FFAs as an independent factor associated with elevated HRPR risk.
Clopidogrel is an essential component of secondary prevention medication prescription among patients with CAD (5). There are many proven risk factors associated with CAD, including insulin resistance, diabetes mellitus, dyslipidemia, chronic inflammation, and so on. Previous studies have suggested that some risk factors for CAD affect the antiplatelet efficacy of clopidogrel (22–24). FFAs is a vital energy source for most body tissues, which is predominantly produced from lipolysis from stored triglycerides. FFAs is metabolized through β-oxidation and converted to water and CO2 to produce large amounts of energy in the form of ATP via β-oxidation and the citric acid cycle in the mitochondria (25). So, the concentration of FFAs is influenced by rates of lipolysis and consumption, which can more sensitively reflect abnormal fat metabolism. The risk for metabolic disease development is worsened by high plasma FFAs content. Previous studies had found that elevated FFAs is a risk factor for many states of abnormal metabolism, including body obesity, insulin resistance, diabetes, hypertension, and non-alcoholic fatty liver disease(26). Our results also showed associations of higher FFAs with higher BMI, diabetes, hypertension, and abnormal lipid indicators. Previous studies have found that elevated FFAs may be closely associated with the occurrence, severity, and adverse prognosis of CAD (15–17). Morbid pathological states or diseases mentioned above were wildly acknowledged as CAD's risk factors and comorbidity, and the impact on these of FFAs might be part of the mechanism that abnormal metabolism cause CAD. To the best of our knowledge, whether higher FFAs affects the antiplatelet efficacy of clopidogrel remained unknown. Our findings suggested a novel potential clinical application of FFAs in predicting clopidogrel efficacy.
TEG dynamically measures physical parameters of clot formation, clot strength, and clot degradation to obtain a quantitative analysis of platelet function (19). MAADP reflects the strength of platelet-fibrin clots formed via the ADP pathway, which had a good diagnostic value for HRPR and a good prognostic utility for thrombosis and ischemic events among patients undergoing PCI (27). The current consensus defines MAADP > 47 mm as HRPR (20). ADPi is calculated according to the equation ADPi=MAADP−MAfibrinMAthrombin−MAFibrin, which reflects the extent of platelet inhibition. According to current consensus and previous Chinese study (11, 21), our study set HRPR as MAADP > 47 mm plus ADPi < 50%. After the univariate and multivariate logistic regression analyses, higher FFAs was demonstrated as a potent independent factor associated with HRPR. Subgroup and sensitivity analyses further demonstrated that result was largely robust except for the female subgroup (P = 0.402). After adjusting confounders including clopidogrel's metabolizer status, we found that higher FFAs was still associated with HRPR. As previously reported, intermediate metabolizers and poor metabolizers of clopidogrel were more likely to present HRPR.
With stronger antiplatelet efficacy, novel P2Y12 antagonists, prasugrel and ticagrelor, have been widely used among patients with acute coronary syndrome or high thrombotic risk (4, 5). But, in many clinical scenarios, clopidogrel is still indispensable by virtue of the advantages of lower economic burden, lower bleeding risk, and fewer side effects, especially among patients with SCAD (4, 5). As a prodrug, clopidogrel can't exert the antiplatelet efficacy until being metabolized by cytochrome P450 (CYP450). Many factors have been reported to affect clopidogrel's antiplatelet efficacy, including genetic factors, drug-drug interaction, and biological and clinical factors. Of concern is the higher prevalence of the CYP2C19 loss-of-function alleles in east Asian populations (28), which leads to a higher incidence of HRPR. Evaluating antiplatelet efficacy using genetic testing or platelet function test is a common practice, although they are not recommended according to the guidelines. Accompanied by a higher proportion of HRPR, East Asians have been suggested to have a higher bleeding risk during receiving novel P2Y12 antagonists (29). TALOS-AMI trial (30) provided evidence that immediate switching from potent P2Y12 inhibitor to clopidogrel after the acute phase is non-inferior for patients suffering from acute myocardial infarction and significantly reduces bleeding risk compared to continued novel P2Y12 antagonists. The de-escalation strategy of DAPT is recommended to be guided based on the genotyping or platelet function test (20). Measuring blood biomarkers such as FFAs is more time-saving, easy to perform, and cheap than sequencing variants of cytochrome P450 genes. From a more practical clinical viewpoint, we provided an economical and simple indicator to assist in predicting HRPR and guiding DAPT de-escalation.
The explanations for the above results are not clear but may be multifactorial. As reported by previous studies, the current study also detected some factors associated with HRPR, including sex, age, diabetes, elevated hs-CRP, and so on. Some of these are associated with higher FFAs, which might partly explain the correlation between FFAs and HRPR. After adjusting for potential confounders and mediator variables, higher FFAs remained independently associated with HRPR, which meant FFAs itself affects residual platelet activity ignited via the ADP pathway. In an earlier study, Hoak JC et al. (31) found a high concentration of FFAs might enhance in vitro platelets' responsiveness to ADP. Patients with metabolic syndrome might enter into a hypercoagulable state. FFAs, a biomarker associated with metabolic syndrome, had been considered to be related to the hypercoagulable prothrombotic tendency in some basic research. Plasminogen activator inhibitor 1 is a biomarker of thrombosis, which exerts anti-fibrinolytic properties by inhibiting tissue-type plasminogen activators and urokinase-like plasminogen activators (32). Mathew M et al. found (33) that elevated FFAs within the physiological range induces plasminogen activator inhibitor 1, which maybe implies elevated FFAs as a pathogenic mechanism for thrombogenesis. TM-endothelial protein C receptor (EPCR)—Protein C pathway is a physiological anticoagulation system (34), Xie W et al. (35) found FFAs inhibit TM-EPCR-Protein C system via activating JNK signaling to promote the hypercoagulable state. Previous studies got evidence that FFAs promotes ADP-induced platelet aggregation and enhances the hypercoagulable state, which provides possible explanations for current observations. Among the study population, higher FFAs significantly enhances ADP-induced platelet activity quantified by TEG parameters and was demonstrated as an independent factor associated with HRPR while using clopidogrel. Current results call for more attention to FFAs while formulating antiplatelet prescriptions and evaluating antiplatelet efficacy of clopidogrel for SCAD patients undergoing PCI. In this research, we firstly found the association of FFAs with ADP-induced residual platelet reactivity among CAD patients receiving clopidogrel therapy. Without adding additional assays and medical expenditures, such as testing genes associated with clopidogrel resistance and testing platelet function, exploring biomarkers associated HRPR from routine items is clinically important. As a cheap and convenient indicator, FFAs might help to identify HRPR patients and to guide the formulation of antiplatelet prescriptions via improving existing prediction models or developing new models companied with other biomarkers.
However, the present study had several limitations. The current research was an observational study based on a single-center and small sample population, which might limit the generalization of our results and impose potential bias. And the cause-and-effect association cannot be determined. Second, due to the limited condition, we had not examined genotypes associated with the metabolism and transport of clopidogrel, such as CYP2C19 and ABCB1 genotypes. Third, our cross-sectional study lacked long-term follow-up data about ischemic and thrombosis events. Fourth, TEG parameters were derived from in vitro simulated coagulation process and might not accurately evaluate in vivo platelet activity. Fifth, all laboratory indicators were tested at baseline only once. Additionally, FFAs contains a range of different components, and different components of FFAs have different metabolic pathways and might be affected to various degrees by abnormal metabolism and other factors. The enzymatic colorimetric method we took just measured the total concentration of FFAs but not the concentration and proportion of FFAs constituents, which might lead to the loss of some crucial information. Finally, the biological mechanism of current conclusion is still unclear, and further investigation is warranted to explore the detailed mechanism.
5. ConclusionOur research found that higher FFAs enhances ADP-induced residual platelet reactivity among CAD patients using clopidogrel and higher FFAs is independently associated with clopidogrel HRPR. The current finding suggested that FFAs is a new, reliable, and accessible clinical biomarker applied in assisting in predicting clopidogrel HRPR and helping to guide the choice of P2Y12 receptor antagonist.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributionsZZ designed the study, analyzed the data, and drafted the manuscript. SD, XH, and MM analyzed the data and drew the figures. KH and TS collected the data from the electronic medical system and constructed the database. SY and YZ designed the study and revised the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1115142/full#supplementary-material.
References2. Galli M, Benenati S, Franchi F, Rollini F, Capodanno D, Biondi-Zoccai G, et al. Comparative effects of guided vs. Potent P2y12 inhibitor therapy in acute coronary syndrome: a network meta-analysis of 61 898 patients from 15 randomized trials. Eur Heart J. (2022) 43(10):959–67. doi: 10.1093/eurheartj/ehab836
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Shoji S, Kuno T, Fujisaki T, Takagi H, Briasoulis A, Deharo P, et al. De-escalation of dual antiplatelet therapy in patients with acute coronary syndromes. J Am Coll Cardiol. (2021) 78(8):763–77. doi: 10.1016/j.jacc.2021.06.012
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 Esc/Eacts guidelines on myocardial revascularization. Eur Heart J. (2019) 40(2):87–165. doi: 10.1093/eurheartj/ehy394
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, et al. 2021 Acc/Aha/scai guideline for coronary artery revascularization: executive summary: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. (2022) 79(2):197–215. doi: 10.1016/j.jacc.2021.09.005
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Siller-Matula JM, Trenk D, Schrör K, Gawaz M, Kristensen SD, Storey RF, et al. Response variability to P2y12 receptor inhibitors: expectations and reality. JACC Cardiovasc Interv. (2013) 6(11):1111–28. doi: 10.1016/j.jcin.2013.06.011
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Tabara Y, Takahashi Y, Kawaguchi T, Setoh K, Terao C, Yamada R, et al. Association of serum-free fatty acid level with reduced reflection pressure wave magnitude and central blood pressure: the nagahama study. Hypertension (Dallas, Tex: 1979). (2014) 64(6):1212–8. doi: 10.1161/HYPERTENSIONAHA.114.04277
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Sobczak AIS, Blindauer CA, Stewart AJ. Changes in plasma free fatty acids associated with type-2 diabetes. Nutrients. (2019) 11(9):2022. doi: 10.3390/nu11092022
CrossRef Full Text | Google Scholar
10. Alshammary AF, Alharbi KK, Alshehri NJ, Vennu V, Ali Khan I. Metabolic syndrome and coronary artery disease risk: a meta-analysis of observational studies. Int J Environ Res Public Health. (2021) 18(4):1773. doi: 10.3390/ijerph18041773
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Zhao X, Li Q, Tu C, Zeng Y, Ye Y. High glycated albumin is an independent predictor of low response to clopidogrel in acs patients: a cross-sectional study. Cardiovasc Diabetol. (2020) 19(1):171. doi: 10.1186/s12933-020-01146-w
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Wang J, Abdus S, Tan C, Gu Q, Yang M, Wang G, et al. Serum uric acid level negatively correlated with the prevalence of clopidogrel low response in patients undergoing antiplatelet treatment with aspirin and clopidogrel. Nutr Metabol Cardiovasc Dis. (2020) 30(12):2215–20. doi: 10.1016/j.numecd.2020.07.025
CrossRef Full Text | Google Scholar
13. Kan Y, Wang H, Lu J, Lin Z, Lin J, Gong P. Significance of plasma free fatty acid level for assessing and diagnosing acute myocardial infarction. Biomark Med. (2020) 14(9):739–47. doi: 10.2217/bmm-2019-0291
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Roy VK, Kumar A, Joshi P, Arora J, Ahanger AM. Plasma free fatty acid concentrations as a marker for acute myocardial infarction. J Clin Diagn Res. (2013) 7(11):2432–4. doi: 10.7860/jcdr/2013/7682.3566
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Xin Y, Zhang J, Fan Y, Wang C. Serum free fatty acids are associated with severe coronary artery calcification, especially in diabetes: a retrospective study. BMC Cardiovasc Disord. (2021) 21(1):343. doi: 10.1186/s12872-021-02152-w
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Jin JL, Cao YX, Liu HH, Zhang HW, Guo YL, Wu NQ, et al. Impact of free fatty acids on prognosis in coronary artery disease patients under different glucose metabolism Status. Cardiovasc Diabetol. (2019) 18(1):134. doi: 10.1186/s12933-019-0936-8
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Zhang MH, Cao YX, Wu LG, Guo N, Hou BJ, Sun LJ, et al. Association of plasma free fatty acids levels with the presence and severity of coronary and carotid atherosclerotic plaque in patients with type 2 diabetes Mellitus. BMC Endocr Disord. (2020) 20(1):156. doi: 10.1186/s12902-020-00636-y
PubMed Abstract | CrossRef Full Text | Google Scholar
18. American Diabetes Association Professional Practice C. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes Care. (2022) 45(Suppl 1):S17–S38. doi: 10.2337/dc22-S002
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Le Quellec S, Bordet JC, Negrier C, Dargaud Y. Comparison of current platelet functional tests for the assessment of aspirin and clopidogrel response. A review of the literature. Thromb Haemostasis. (2016) 116(4):638–50. doi: 10.1160/th15-11-0870
CrossRef Full Text | Google Scholar
20. Sibbing D, Aradi D, Alexopoulos D, Ten Berg J, Bhatt DL, Bonello L, et al. Updated expert consensus statement on platelet function and genetic testing for guiding P2y(12) receptor inhibitor treatment in percutaneous coronary intervention. JACC Cardiovasc Interv. (2019) 12(16):1521–37. doi: 10.1016/j.jcin.2019.03.034
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Tang YD, Wang W, Yang M, Zhang K, Chen J, Qiao S, et al. Randomized comparisons of double-dose clopidogrel or adjunctive cilostazol versus standard dual antiplatelet in patients with high posttreatment platelet reactivity: results of the creative trial. Circulation. (2018) 137(21):2231–45. doi: 10.1161/CIRCULATIONAHA.117.030190
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Li J, Yuan D, Jiang L, Tang X, Xu J, Song Y, et al. Similar inflammatory biomarkers reflect different platelet reactivity in percutaneous coronary intervention patients treated with clopidogrel: a large-sample study from China. Front Cardiovasc Med. (2021) 8:736466. doi: 10.3389/fcvm.2021.736466
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Zhao X, Wang J, Li Q, Ye Y, Zeng Y. Impact of pancreatic β-cell function on clopidogrel responsiveness and outcomes in Chinese nondiabetic patients undergoing elective percutaneous coronary intervention. Cardiovasc Drugs Ther. (2023) 37(3):487–96. doi: 10.1007/s10557-021-07272-1
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Angiolillo DJ, Capodanno D, Danchin N, Simon T, Bergmeijer TO, Ten Berg JM, et al. Derivation, validation, and prognostic utility of a prediction rule for nonresponse to clopidogrel: the abcd-gene score. JACC Cardiovasc Interv. (2020) 13(5):606–17. doi: 10.1016/j.jcin.2020.01.226
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Hou X, Han W, Gan Q, Liu Y, Fang W. Relationship between thromboelastography and long-term ischemic events as gauged by the response to clopidogrel in patients undergoing elective percutaneous coronary intervention. Biosci Trends. (2017) 11(2):209–13. doi: 10.5582/bst.2016.01233
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Man M, Farmen M, Dumaual C, Teng CH, Moser B, Irie S, et al. Genetic variation in metabolizing enzyme and transporter genes: comprehensive assessment in 3 Major east Asian subpopulations with comparison to caucasians and Africans. J Clin Pharmacol. (2010) 50(8):929–40. doi: 10.1177/0091270009355161
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Kim HK, Tantry US, Smith SC Jr, Jeong MH, Park SJ, Kim MH, et al. The East Asian paradox: an updated position statement on the challenges to the current antithrombotic strategy in patients with cardiovascular disease. Thromb Haemostasis. (2021) 121(4):422–32. doi: 10.1055/s-0040-1718729
CrossRef Full Text | Google Scholar
30. Kim CJ, Park MW, Kim MC, Choo EH, Hwang BH, Lee KY, et al. Unguided de-escalation from ticagrelor to clopidogrel in stabilised patients with acute myocardial infarction undergoing percutaneous coronary intervention (talos-ami): an investigator-initiated, open-label, multicentre, non-inferiority, randomised trial. Lancet (London, England). (2021) 398(10308):1305–16. doi: 10.1016/S0140-6736(21)01445-8
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Mathew M, Tay E, Cusi K. Elevated plasma free fatty acids increase cardiovascular risk by inducing plasma biomarkers of endothelial activation, myeloperoxidase and pai-1 in healthy subjects. Cardiovasc Diabetol. (2010) 9:9. doi: 10.1186/1475-2840-9-9
PubMed Abstract | CrossRef Full Text | Google Scholar
34. Kario K, Matsuo T, Kobayashi H, Matsuo M, Sakata T, Miyata T. Activation of tissue factor-induced coagulation and endothelial cell dysfunction in non-insulin-dependent diabetic patients with microalbuminuria. Arterioscler, Thromb, Vasc Biol. (1995) 15(8):1114–20. doi: 10.1161/01.ATV.15.8.1114
PubMed Abstract | CrossRef Full Text | Google Scholar
35. Xie W, Zhai Z, Yang Y, Kuang T, Wang C. Free fatty acids inhibit tm-epcr expression through jnk pathway: an implication for the development of the prothrombotic state in metabolic syndrome. J Thromb Thrombolysis. (2012) 34(4):468–74. doi: 10.1007/s11239-012-0793-8
留言 (0)