
記住我








Heart failure with reduced ejection fraction (HFrEF) is a complex syndrome where cardiac output is unable to meet metabolic demands and accommodate venous return; the only curative treatment is cardiac transplantation (1). The relative paucity of organs for transplantation has led to the adoption of left ventricular assist devices (LVADs) to durably support circulation in select individuals. LVADs have proven superior to optimal medical therapy in trials and registry data (2–4). Current best data suggest a 1-year survival rate of more than 80% with LVAD therapy (5).
Functional tricuspid regurgitation (TR) is present to some degree in 88% of patients with HFrEF (6). In patients with significant left ventricular (LV) dysfunction warranting isolated LVAD support, the prevalence rate of severe TR is 11.7% (5). TR is associated with worse outcomes in patients undergoing LVAD implantation—the duration of postoperative inotropic support, hospital stay, and temporary right ventricular assist device (RVAD) requirement are all increased in patients with significant preimplant TR (7). Furthermore, there is a concern over decreased survival rates (7).
An understanding of the pathophysiology, clinical significance, and best management of TR in the setting of LVAD support is necessary, given the prevalence and impact of TR in this population, and this is the focus of this review.
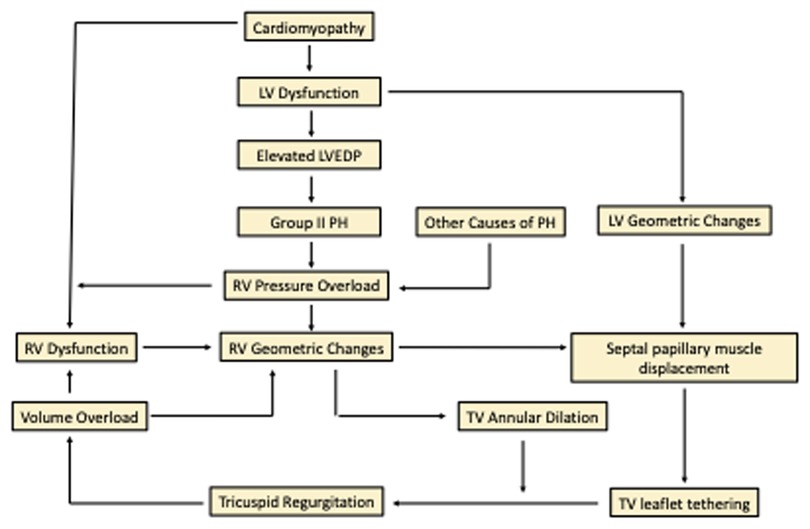
2. Pathophysiology of functional tricuspid regurgitationThere is a close relationship between TR and left and right ventricular (RV) dysfunction. In patients under consideration for LVAD therapy, the underlying cardiomyopathy results in severe LV dysfunction. Chronic volume and pressure overload of the left heart leads to cardiac remodeling with ventricular dilation and hypertrophy.
The increased left-sided pressure results in WHO group 2 pulmonary hypertension (PH) and transmission of the hydrostatic pressure to the RV via the pulmonary vasculature. Functional TR is thus strongly linked to the severity of PH (8). The increased afterload causes RV geometric changes (9). In addition, the underlying cardiomyopathy may affect the RV muscle directly, causing RV dysfunction and RV pressure/volume overload.
Geometric changes include enlargement of the RV apically, lengthening of the ventricle, annular dilation of the tricuspid valve (TV), and papillary muscle displacement, leading directly to tricuspid regurgitation (10, 11). Annular dilation and annular area have been linked to the severity of TR (8, 12). Frequently, these patients also suffer from chronic atrial fibrillation, which contributes to dilation of the right atrium (RA) and tricuspid annulus (13). The geometric changes in the RV pull the papillary muscles outward, restricting or tethering/tenting the leaflets of the TV (11, 13, 14). Although TV leaflet tethering is most strongly associated with RV size and geometry, LV function is an independent and weaker contributor (15). This contribution of LV dysfunction may be explained by a displacement of the septal RV papillary muscle and apical displacement of the anterior papillary muscle seen with LV dilation (8, 12, 16). Tethering of the TV leaflets is sufficient to induce regurgitation in patients even in the absence of significant annular dilation (15). Both annular dilation alone and isolated papillary muscle displacement have been confirmed to cause TR in a porcine in vitro model (17).
A positive feedback loop compounds the issue with an increase in volume, worsening geometric changes, and progression of the TR unless the loop is successfully interrupted (Figure 1) (18). Chronic TR results in irreversible cardiac remodeling (19).
Figure 1. Pathophysiology of tricuspid regurgitation. LV, left ventricle; RV, right ventricle; PH, pulmonary hypertension; TV, tricuspid valve; LVEDP, left ventricular end diastolic pressure.
3. Natural history and impact of uncorrected TR in LVAD placementRV function is known to be critical to successful LVAD placement (20). As the pathophysiology of TR affects RV function, there are concerns around the clinical impact of significant TR in patients requiring LVAD placement. A review of 2,527 patients in the INTERMACS registry associated the presence of moderate and severe TR pre-LVAD implantation with worse long-term survival (21). Indeed, long-term survival is worse in patients with both preimplant RV dysfunction and preimplant significant TR, suggesting a synergistic detrimental effect (22).
It has been hypothesized that an acute increase in venous return and RV stroke volume from the LVAD can lead to worsening RVF and TR. Conversely, LVAD placement has the potential to interrupt the cycle of volume and pressure overload and improve TR through direct LV unloading.
In examining the effect of LVAD placement in offloading the LV, significant reverse cardiac remodeling was noted within 40 days of implant in hearts explanted at the time of transplant (23). Multiple studies have demonstrated improvements after LVAD placement in pulmonary artery pressures, pulmonary vascular resistance (PVR), pulmonary capillary wedge pressures, and in RV and TV function (22, 24–30). TR improvement after LVAD placement was seen more in patients with a higher PVR, which is likely, as such patients gain from LVAD placement through a substantial decline in PVR (29). Significant echocardiographic improvement in moderate to severe TR occurs in 55%–81% of patients (22, 25, 28, 29). These findings are noted early in the postoperative period, and TR continues to improve over a longer-term follow-up (22, 30). However, not all patients with significant TR show improvement in TV function, and a proportion of patients experience a worsening of TR after LVAD implantation (27, 31).
3.1. Effect of preoperative TR on early and late RV functionA study of first-generation LVADs showed that 75% of patients with Grade III or IV TR developed early RVF post-LVAD placement compared with only 12% of patients with grade I or II TR (32). With the continuous flow HeartMate II LVAD, severe preoperative TR was identified as one of several independent predictors for early biventricular support (30). In a randomized trial of LVAD placement with a similar incidence of moderate to severe preoperative TR in both arms (approximately one-quarter), RVF requiring RVAD placement was low and did not vary between the axial flow HeartMate II and the centrifugal flow HeartMate 3 devices (33). In comparison, when looking exclusively at patients with moderate to severe TR undergoing mostly HeartMate 3 placement without TV surgery, the incidence of severe RVF was higher—inotropic support for more than 14 days was needed in 37.5% of patients, and 14.3% of patients required RVAD support (34). Preimplant TR, in combination with elevated RA pressure and end-organ dysfunction, was associated with an increase in early mortality after continuous flow LVAD placement in a large study of the EUROMACS registry (22). These data underline the early hazards related to significant TR.
Late RVF, occurring in 12% of LVAD recipients, is noted to be a frequent cause of death beyond the first year of implant and linked to worse long-term survival (35–37). Preimplantation significant TR was identified as the strongest independent predictor for late RVF; up to 81.2% of patients with late RVF had preimplant moderate or severe TR (38).
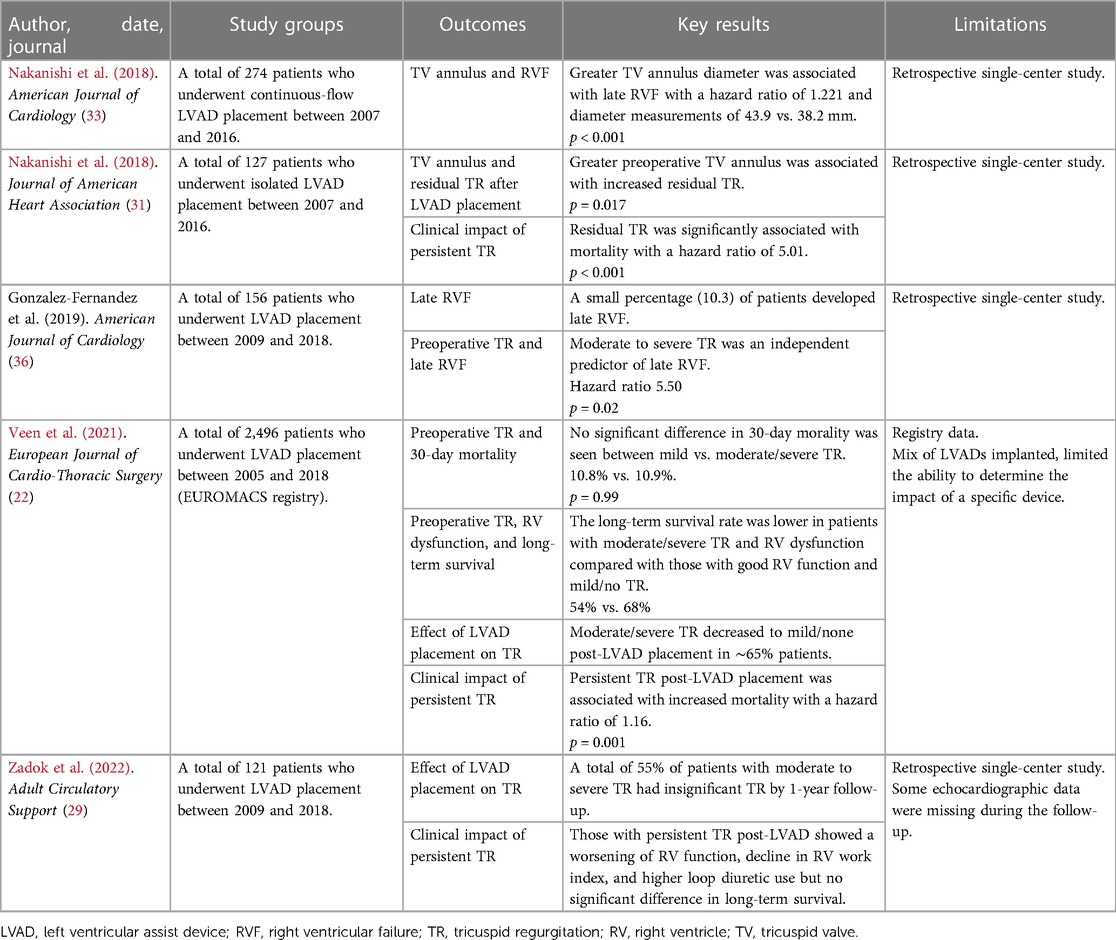
3.2. Persistent/residual TR after LVAD placementCritically, patients with residual TR have been identified to have increased long-term mortality, and the persistence of significant TR after LVAD placement is associated with a decline in RV function (22, 29, 31). Table 1 summarizes studies examining the late effects of TR after LVAD placement.
Table 1. Summary of studies examining long-term results with significant preoperative TR that is not corrected at LVAD placement.
Several authors have attempted to identify factors that might predict persistent TR after LVAD placement. In one study, residual TR was associated with preoperative TV annulus diameter but not with leaflet tethering (31). Patients with atrial fibrillation are less likely to see an improvement in TR post-LVAD placement, probably because the etiology of their TR includes RA dilation from atrial fibrillation and is less positively impacted by LVAD implantation (29). Atrial fibrillation has also been weakly associated with a progression of TR after LVAD placement (39).
4. Impact of concomitant TV surgery at LVAD implantWhile significant TR is frequently identified in patients undergoing LVAD placement, the decision to opt for concomitant tricuspid valve intervention (TVI) is controversial. Intervention at the time of LVAD placement could consist of tricuspid valve repair (TVr) or replacement. In practice, repair with an annuloplasty ring has been the dominant mode of TVI (40). Performance of a TVI increases cardiopulmonary bypass (CPB) time and may require cardiac arrest; both of which have the potential to increase operative risk and RVF (26, 41).
Initial experience in a cohort with older-generation LVADs showed a reduction in inotrope use, renal dysfunction, and length of hospital stay in patients of the TVI group as well as a non-significant reduction in the use of RVADs (42). A more recent study of continuous flow LVADs comparing concomitant TVI with isolated LVAD placement in patients with severe TR found a decrease in 30-day readmissions with TVI (43). However, there was no difference in RVF, survival, or TR recurrence.
Two small series identified no substantial difference in outcomes for patients undergoing TVI with LVAD placement and those receiving LVAD implants without TVI, but the groups without TVI did not have significant TR, rendering the comparison difficult (44, 45). Others, including a meta-analysis, found no outcome benefit to TVI, including in clinical measures of RVF or survival (21, 41, 46). A recent propensity-matched cohort of the EUROMACS registry identified patients undergoing TVI to have an intensive care unit (ICU) stay lengthened by 4 days with no benefit in clinical outcomes (26). In this cohort, moderate to severe TR was less prevalent in patients with TVI immediately after surgery but became comparable with time.
A large single-center series with a mix of continuous flow LVADs revealed an improvement in TR with TVI at the expense of increased bleeding and transfusion and no improvement in clinical outcomes (47).
Of concern, TVI was associated with increases in operative time, length of inotropic support, ventilatory support, and ICU stay as well as morbidities such as bleeding, transfusion, RVF, and renal failure in three small single-center series (48–50). In a larger study of patients with moderate to severe TR from the STS database, LVAD placement with concomitant TVI, in comparison with LVAD alone, did not affect RVAD use or death but did increase the risk for renal failure, transfusion, reoperation, ventilator, ICU, and hospital length of stay. Similarly, an analysis of the INTERMACS database associated TVI with increased bleeding, arrhythmia, stroke, and mortality (51).
Methodological concerns in these studies include their retrospective nature, unequal comparator groups particularly with respect to TR severity, and the possibility of selection bias. The TVVAD study randomized patients at a single center with moderate or severe TR to LVAD alone or with concomitant TVI and utilized a primary endpoint of RVF. This study predominantly utilized the current generation of continuous flow LVAD (HeartMate 3, Abbott). Early published results demonstrate an improvement in TR with no substantive clinical benefit, including in the primary endpoint, survival, or adverse events (34). The parameter of quality of life measured by using the Kansas City Cardiomyopathy Questionnaire was also similar between the two groups.
Long-term failure of TVr is an additional concern. In 156 patients with continuous flow LVADs, 37.8% were identified as having a failed TVr defined as moderate or severe TR on any postoperative echocardiographic follow-up (52). Postintervention significant TR (recurrent TR) has been associated with RVF and worse heart failure-free outcomes (46, 52).
Taken together, the data do not currently support TVI at the time of LVAD placement for patients with significant TR. Clinical benefit has not been conclusively demonstrated, and risks such as bleeding, organ dysfunction, and prolongation of various indices of hospital care have been identified and are likely a sequela of prolonging CPB.
Why is TV surgery not helpful for this patient population despite the association of preoperative TR with worse post-LVAD clinical outcomes? There are several hypotheses, and the following are some of them: (1) TR improves in the majority of patients with LVAD therapy such that TVI for all would “overtreat”; (2) TR persists in some patients despite TVI raising the possibility that a different surgical strategy might be more effective in the long-term treatment of TR; (3) TR develops de novo in some patients who do not have significant TR at LVAD implant, thus making it hard to draw meaningful comparisons with a control “no pre-operative TR” group; (4) TR is a marker of ventricular dysfunction, does not directly affect clinical outcomes, and thus, interventions aimed at TR do not improve outcomes; and (5) TV surgery involves operative time and risk that negate the benefit.
5. De novo significant tricuspid regurgitation after LVAD placementDuring the follow-up of LVAD recipients, incidence rates range from 6% to 20% of the development of significant TR in patients with none or mild preoperative TR (22, 28, 29, 31). The function of the RV in this subpopulation has not been defined in the available literature and no preoperative clinical/echocardiographic or operative parameters that predict the development of TR after LVAD placement have been identified (28, 29). It is unclear whether this subset of patients with de novo TR carries a risk of RVF or worse long-term prognosis compared with patients with insignificant TR or resolved TR after LVAD placement; this is an area for future investigations.
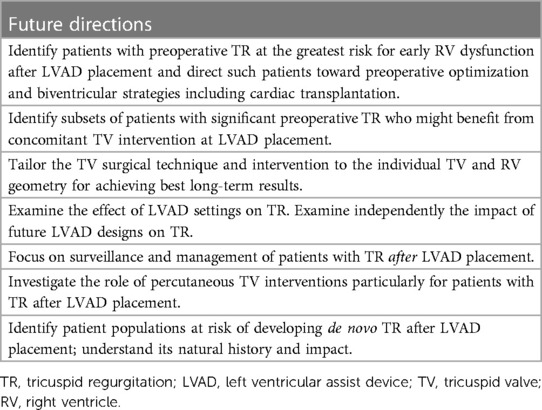
6. Future directionsSeveral outstanding questions related to the natural history and best management of TR in the setting of LVAD therapy remain, which should guide future directions of study (Table 2).
Table 2. Future directions for understanding and managing tricuspid regurgitation in the setting of LVAD support.
It remains unclear whether TR is a marker for RV dysfunction and a predictor of worse clinical outcomes in LVAD recipients or whether it is a causative agent. Longer-term follow-up of the randomized TVVAD trial will be important to clarify the predictors of worse clinical outcomes, the role of TVI, the durability of TVr, and the clinical impact of persistent or recurrent TR.
It is possible that the particular unloading pattern (axial vs. centrifugal flow) of the LVAD implanted affects TR in a way that has not been well defined. In addition, the setting of the LVAD might be impactful with a higher speed unloading the LV more but also, perhaps, increasing venous return. Most published studies include a heterogenous group of LVADs. Future studies of advancing LVAD technology, or studies that include historical devices, separate based upon the type of LVAD based on the LVAD implanted and also to examine the effect of LVAD setting on TR.
Subgroups of patients with significant TR that might benefit from concomitant TVI should be studied. These could include those with TR pathophysiology least likely to respond to isolated LVAD placement. Potential candidates would be patients (1) with severe TR, as most studies to date combine moderate and severe TR, (2) with a dilated TV annulus, (3) with tethered leaflets, and (4) with preoperative atrial fibrillation, as it contributes to the pathophysiology of TR and is associated with persistent TR after LVAD placement. Similarly, if subgroups with the highest early RVF risk are identified, they might be preferred for heart transplantation over LVAD placement.
The current preferred strategy for TVr with an annuloplasty needs re-evaluation. In a non-LVAD setting of TV repair with annuloplasty, TV tethering was the strongest predictor of residual TR (53). Based on TV pathology, certain patients, such as those with significant TV tethering, may warrant a consideration of complex repairs or valve replacement (53, 54). What is the role of percutaneous TVI with edge-to-edge repair in this population? Benefits might lie in avoiding prolongation of the index operation and shifting the focus on patients with TR after LVAD placement.
Patients with TR after LVAD placement could be classified as persistent, recurrent after TVI, or de novo. They warrant more attention through heightened surveillance and an understanding of the etiology of their TR, natural history, and best management.
7. ConclusionSignificant TR is commonly found in patients with severe LV dysfunction under consideration for LVAD placement. Although its pathophysiology is delineated, and it has been linked to worse clinical outcomes, the best management of significant TR at the time of LVAD placement and afterward remains unclear. TR after LVAD placement is of particular concern as it is linked to progressive RV dysfunction and associated morbidity. These patients warrant further study to understand their best management.
Author contributionsAM and AS outlined the manuscript together. AM wrote the preliminary draft. AS edited and provided additions to the manuscript significantly. Both AM and AS worked on the manuscript revisions, figures, and tables. All authors contributed to the article and approved the submitted version.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Peura JL, Colvin-Adams M, Francis GS, Grady KL, Hoffman TM, Jessup M, et al. Recommendations for the use of mechanical circulatory support: device strategies and patient selection. Circulation. (2012) 126(22):2648–67. doi: 10.1161/CIR.0b013e3182769a54
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Rose EA, Gelijns AC, Moskowitz AJ, Heitjan DF, Stevenson LW, Dembitsky W, et al. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. (2001) 345(20):1435–43. doi: 10.1056/NEJMoa012175
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Slaughter MS, Rogers JG, Milano CA, Russell SD, Conte JV, Feldman D, et al. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med. (2009) 361(23):2241–51. doi: 10.1056/NEJMoa0909938
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Mehra MR, Cleveland JC, Uriel N, Cowger JA, Hall S, Horstmanshof D, et al. Primary results of long-term outcomes in the MOMENTUM 3 pivotal trial and continued access protocol study phase: a study of 2200 HeartMate 3 left ventricular assist device implants. Eur J Heart Fail. (2021) 23(8):1392–400. doi: 10.1002/ejhf.2211
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Molina EJ, Shah P, Kiernan MS, Cornwell WK, Copeland H, Takeda K, et al. The Society of Thoracic Surgeons INTERMACS 2020 annual report. Ann Thorac Surg. (2021) 111(3):778–92. doi: 10.1016/j.athoracsur.2020.12.038
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Benfari G, Antoine C, Miller WL, Thapa P, Topilsky Y, Rossi A, et al. Excess mortality associated with functional tricuspid regurgitation complicating heart failure with reduced ejection fraction. Circulation. (2019) 140(3):196–206. doi: 10.1161/CIRCULATIONAHA.118.038946
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Piacentino V 3rd, Williams ML, Depp T, Garcia-Huerta K, Blue L, Lodge AJ, et al. Impact of tricuspid valve regurgitation in patients treated with implantable left ventricular assist devices. Ann Thoracic Surg. (2011) 91(5):1342–6. doi: 10.1016/j.athoracsur.2011.01.053
CrossRef Full Text | Google Scholar
8. Spinner EM, Lerakis S, Higginson J, Pernetz M, Howell S, Veledar E, et al. Correlates of tricuspid regurgitation as determined by 3D echocardiography: pulmonary arterial pressure, ventricle geometry, annular dilatation, and papillary muscle displacement. Circ Cardiovasc Imaging. (2012) 5(1):43–50. doi: 10.1161/CIRCIMAGING.111.965707
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Koelling T, Aaronson K, Cody R, Bach D, Armstrong W. Prognostic significance of mitral regurgitation and tricuspid regurgitation in patients with left ventricular systolic dysfunction. American Heart Journal. (2002) 144(3):524–9. doi: 10.1067/mhj.2002.123575
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Sukmawan R, Watanabe N, Ogasawara Y, Yamaura Y, Yamamoto K, Wada N, et al. Geometric changes to tricuspid valve tenting in tricuspid regurgitation secondary to pulmonary hypertension quantified by novel system with transthoracic real-time 3-dimensional echocardiography. J Am Soc Echocardiogr. (2007) 20(5):470–7. doi: 10.1016/j.echo.2006.10.001
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Park YH, Song JM, Lee EY, Kim YJ, Kang DH, Song JK. Geometric and hemodynamic determinants of functional tricuspid regurgitation: a real-time three-dimensional echocardiography study. Int J Cardiol. (2008) 124(2):160–5. doi: 10.1016/j.ijcard.2006.12.036
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Topilsky Y, Khanna A, Tourneau TL, Park S, Michelena H, Suri R, et al. Clinical context and mechanism of functional tricuspid regurgitation in patient with and without pulmonary hypertension. Cardiovascular Imaging. (2012) 5(3):314–23. doi: 10.1161/CIRCIMAGING.111.967919
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Fukuda S, Gillinov AM, Song JM, Daimon M, Kongsaerepong V, Thomas JD, et al. Echocardiographic insights into atrial and ventricular mechanisms of functional tricuspid regurgitation. Am Heart J. (2006) 152(6):1208–14. doi: 10.1016/j.ahj.2006.07.027
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Spinner E, Sundareswaran K, Das LP, Thourani V, Oshinski J, Yoganathan A. Altered right ventricular papillary muscle position and orientation in patients with a dilated left ventricle. J Thorac Cardiovasc Surg. (2011) 141(3):744–9. doi: 10.1016/j.jtcvs.2010.05.034
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Spinner E, Shannon P, Buice D, Jimenez JH, Veledar E, del Nido P, et al. In vitro characterization of the mechanisms responsible for functional tricuspid regurgitation. Circulation. (2011) 124:920–9. doi: 10.1161/CIRCULATIONAHA.110.003897
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Ramsdell G, Nelson J, Pislaru S, Ramakrishna H. Tricuspid regurgitation in congestive heart failure: management strategies and analysis of outcomes. J Cardiothorac Vasc Anesth. (2021) 35(4):1205–14. doi: 10.1053/j.jvca.2020.06.022
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Zoghbi W, Adams D, Bonow R, Enriquez-Sarano M, Foster E, Grayburn P, et al. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American Society of Echocardiography developed in collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr. (2017) 30(4):303–71. doi: 10.1016/j.echo.2017.01.007
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Marciniak A, Glover K, Sharma R. Cohort profile: prevalence of valvular heart disease in community patients with suspected heart failure in UK. BMJ Open. (2017) 7(1):e012240. doi: 10.1136/bmjopen-2016-012240
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Song H, Gelow J, Mudd J, Hollifield K, Naftel D, Kirklini J. Limited utility of tricuspid valve repair at the time of left ventricular assist device implantation. Ann Thorac Surg. (2016) 101(6):2168–74. doi: 10.1016/j.athoracsur.2016.03.040
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Veen K, Mokhles M, Soliman O, de By TMMH, Mohacsi P, Schoenrath F, et al. Clinical impact and “natural” course of uncorrected tricuspid regurgitation after implantation of a left ventricular assist device: an analysis of the European Registry for Patients with Mechanical Circulatory Support (EUROMACS). Eur J Cardiothorac Surg. (2021) 59(1):207–16. doi: 10.1093/ejcts/ezaa294
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Madigan J, Barbone A, Choudhri A, Morales D, Cai B, Oz M, et al. Time course of reverse remodeling of left ventricle during support with a left ventricular assist device. J Thorac Cardiovasc Surg. (2001) 121(5):902–8. doi: 10.1067/mtc.2001.112632
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Frazier O, Benedict C, Radovancevic B, Bick R, Springer W, Macris M, et al. Improved left ventricular function after chronic left ventricular unloading. The Annals of thoracic surgery. (1996) 62(3):681–2. doi: 10.1016/s0003-4975(96)00437-7
CrossRef Full Text | Google Scholar
25. Morgan J, Paone G, Nemeh H, Murthy R, Williams C, Tita C, et al. Impact of continuous-flow left ventricular assist device support on right ventricular function. J Heart Lung Transplant. (2013) 32(4):398–403. doi: 10.1016/j.healun.2012.12.018
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Veen KM, Caliskan K, de By TMMH, Mokhles MM, Soliman OI, Mohacsi P, et al. Outcomes after tricuspid valve surgery concomitant with left ventricular assist device implantation in the EUROMACS registry: a propensity score matched analysis. Eur J Cardiothorac Surg. (2019) 56(6):1081–89. doi: 10.1093/ejcts/ezz208
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Lee S, Kamdar F, Madlon-Kay R, Boyle A, Colvin-Adams M, Pritzker M, et al. Effects of the HeartMate II continuous-flow left ventricular assist device on right ventricular function. J Heart Lung Transplant. (2010) 29(2):209–15. doi: 10.1016/j.healun.2009.11.599
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Mulzer J, Mueller M, Knierim J, Lanmueller P, Potapov E. Myocardial function recovery interventional assessment and surgical pump removal. Ann Cardiothorac Surg. (2021) 10(3):402–4. doi: 10.21037/acs-2020-cfmcs-12
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Zadok O, Ben-Avraham B, Barac Y, Hammer Y, Rubachevski V, Shaul A, et al. Natural history and prognosis of patients with unrepaired tricuspid regurgitation undergoing implantation of left ventricular assist device. ASAIO J. (2022) 68(4):508–15. doi: 10.1097/MAT.0000000000001521
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Alturi P, Fairman A, MacArthur JW, Goldstone AB, Cohen JE, Howard JL, et al. Continuous flow left ventricular assist device implant significantly improves pulmonary hypertension, right ventricular contractility, and tricuspid valve competence. J Card Surg. (2013) 28(6):770–5. doi: 10.1111/jocs.12214
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Nakanishi K, Homma S, Han J, Takayama H, Colombo P, Yuzefpolskaya M, et al. Prevalence, predictors, and prognostic value of residual tricuspid regurgitation in patients with left ventricular assist device. J Am Heart Assoc. (2018) 7(13):e008813. doi: 10.1161/JAHA.118.008813
PubMed Abstract | CrossRef Full Text | Google Scholar
32. Potapov EV, Stepanenko A, Dandel M, Kukucka M, Lehmkuhl HB, Weng Y, et al. Tricuspid incompetence and geometry of the right ventricle as predictors of right ventricular function after implantation of a left ventricular assist device. J Heart Lung Transplant. (2008) 27(12):1275–81. doi: 10.1016/j.healun.2008.08.012
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Mehra M, Uriel N, Naka Y, Cleveland J, Yuzefpolskaya M, Salerno C, et al. A fully magnetically levitated left ventricular assist device—final report. N Engl J Med. (2019) 380:1618–27. doi: 10.1056/NEJMoa1900486
PubMed Abstract | CrossRef Full Text | Google Scholar
34. Pla MM, Chiang Y, Nicoara A, Poehlein E, Green CL, Gross R, et al. Surgical treatment of tricuspid valve regurgitation in patients undergoing left ventricular assist device implantation: interim analysis of the TVVAD trial. J Thorac Cardiovasc Surg. (2022):S0022-5223(22)01243-0.doi: 10.1016/j.jtcvs.2022.10.054. [Epub ahead of print]36639288
PubMed Abstract | CrossRef Full Text | Google Scholar
35. Nakanishi K, Homma S, Han J, Takayama H, Colombo P, Yuzefpolskaya M, et al. Useless of tricuspid annular diameter to predict late right sided heart failure in patients with left ventricular assist device. Am J Cardiol. (2018) 122(1):115–20. doi: 10.1016/j.amjcard.2018.03.010
PubMed Abstract | CrossRef Full Text | Google Scholar
36. Takeda K, Takayama H, Colombo P, Yuzefpolskaya M, Fukuhara S, Han J, et al. Incidence and clinical significance of late right heart failure during continuous-flow left ventricular assist device support. J Heart Lung Transplant. (2015) 34(8):1024–32. doi: 10.1016/j.healun.2015.03.011
PubMed Abstract | CrossRef Full Text | Google Scholar
37. Stulak J, Mehta V, Schirger J, Aaronson K, Joyce L, Daly R, et al. Temporal differences in causes of mortality after left ventricular assist device implantation. Ann Thorac Surg. (2015) 99(6):1969–74. doi: 10.1016/j.athoracsur.2015.01.036
PubMed Abstract | CrossRef Full Text | Google Scholar
38. Gonzalez-Fernandez O, Bouzas-Crus N, Ferrera C, Woods A, Robinson-Smith N, Tovey S, et al. Effect of preoperative tricuspid and/or mitral regurgitation on development of late right-sided heart failure after insertion of HeartWare left ventricular assist device. Am J Cardiol. (2020) 125(2):236–43. doi: 10.1016/j.amjcard.2019.10.005
PubMed Abstract | CrossRef Full Text | Google Scholar
39. Anwer L, Tchantchaleishvili V, Poddi S, Daly R, Joyce L, Kushwaha S, et al. Atrial fibrillation should guide prophylactic tricuspid procedures during left ventricular assist device implantation. Am Soc Artif Intern Organs. (2018) 64(5):586–93. doi: 10.1097/MAT.0000000000000698
CrossRef Full Text | Google Scholar
40. Robertson J, Grau-Sepulveda M, Okada S, O’Brien S, Brennan M, Shah A, et al. Concomitant tricuspid valve surgery during implantation of continuous-flow left ventricular assist devices: a Society of Thoracic Surgeons database analysis. J Heart Lung Transplant. (2014) 33(6):609–17. doi: 10.1016/j.healun.2014.01.861
PubMed Abstract | CrossRef Full Text | Google Scholar
41. Dunlay S, Deo S, Park S. Impact of tricuspid valve surgery at the time of left ventricular assist device insertion on postoperative outcomes. Am Soc Artif Intern Organs. (2015) 61(1):15–20. doi: 10.1097/MAT.0000000000000145
CrossRef Full Text | Google Scholar
42. Piacentino V, Troupes CD, Ganapathi AM, Blue LJ, Mackensen GB, Swaminathan M, et al. Clinical impact of concomitant tricuspid valve procedures during left ventricular assist device implantation. Ann Thorac Surg. (2011) 92(4):1414–8. doi: 10.1016/j.athoracsur.2011.05.084
PubMed Abstract | CrossRef Full Text | Google Scholar
43. Critsinelis A, Kurihara C, Kawabori M, Sugiura T, Loor G, Frazier OH, et al. Outcomes in patients who underwent a concomitant tricuspid valve procedure during left ventricular assist device implantation. J Card Surg. (2019) 34(12):1458–64. doi: 10.1111/jocs.14304
PubMed Abstract | CrossRef Full Text | Google Scholar
44. Pal JD, Klodell CT, John R, Pagani FD, Rogers JG, Farrar DJ, et al. Low operative mortality with implantation of continuous-flow ventricular assist device and impact of concurrent cardiac procedures. Circulation. (2009) 120(11 Suppl):S215–9. doi: 10.1161/CIRCULATIONAHA.108.844274
留言 (0)