Conservative Management with Functional Brace Versus Various Surgical Fixation Techniques for Humeral Shaft Fractures: A Network Meta-Analysis
Background:
Historically, humeral shaft fractures have been successfully treated with nonoperative management and functional bracing; however, various surgical options are also available. In the present study, we compared the outcomes of nonoperative versus operative interventions for the treatment of extra-articular humeral shaft fractures.
Methods:
This study was a network meta-analysis of prospective randomized controlled trials (RCTs) in which functional bracing was compared with surgical techniques (including open reduction and internal fixation [ORIF], minimally invasive plate osteosynthesis [MIPO], and intramedullary nailing in both antegrade [aIMN] and retrograde [rIMN] directions) for the treatment of humeral shaft fractures. The outcomes that were assessed included time to union and the rates of nonunion, malunion, delayed union, secondary surgical intervention, iatrogenic radial nerve palsy, and infection. Mean differences and log odds ratios (ORs) were used to analyze continuous and categorical data, respectively.
Results:
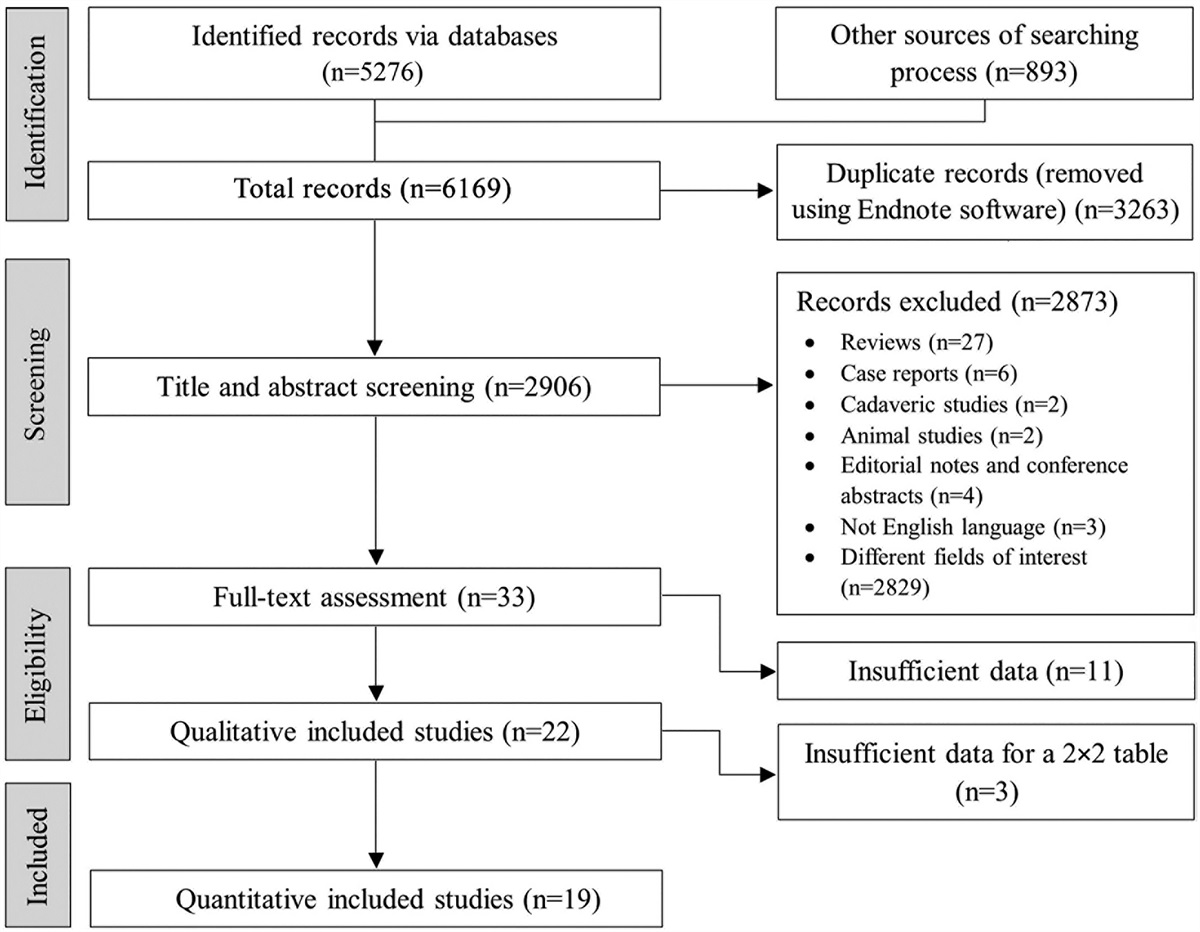
Twenty-one RCTs evaluating the outcomes for 1,203 patients who had been treated with functional bracing (n = 190), ORIF (n = 479), MIPO (n = 177), aIMN (n = 312), or rIMN (n = 45) were included. Functional bracing yielded significantly higher odds of nonunion and significantly longer time to union than ORIF, MIPO, and aIMN (p < 0.05). Comparison of surgical fixation techniques demonstrated significantly faster time to union with MIPO than with ORIF (p = 0.043). Significantly higher odds of malunion were observed with functional bracing than with ORIF (p = 0.047). Significantly higher odds of delayed union were observed with aIMN than with ORIF (p = 0.036). Significantly higher odds of secondary surgical intervention were observed with functional bracing than with ORIF (p = 0.001), MIPO (p = 0.007), and aIMN (p = 0.004). However, ORIF was associated with significantly higher odds of iatrogenic radial nerve injury and superficial infection than both functional bracing and MIPO (p < 0.05).
Conclusions:
Compared with functional bracing, most operative interventions demonstrated lower rates of reoperation. MIPO demonstrated significantly faster time to union while limiting periosteal stripping, whereas ORIF was associated with significantly higher rates of radial nerve palsy. Nonoperative management with functional bracing demonstrated higher nonunion rates than most surgical techniques, often requiring conversion to surgical fixation.
Level of Evidence:
Therapeutic Level I. See Instructions for Authors for a complete description of levels of evidence.






留言 (0)