
記住我








Management of acute cardiovascular diseases is constantly improving, which leads to a progressive increase of life expectancy and consequently, to a progressive increase of disease prevalence (1). Unavoidably, this will be associated with an increase of direct and indirect cost. Over a period of 20 years (2010–2030) a +25% increase of prevalence is expected to generate an increase of +215% of costs (2). Therefore, it is of paramount importance to explore innovative solutions that hold the promise of improving clinical outcomes in the domain of cardiovascular diseases and may reduce the financial burden on healthcare systems.
Heart failure (HF) is the largest cause of hospitalization in patients aged ≥65 years in Western countries (3–5). Recently data from the Italian ARNO observatory estimated that patients hospitalized for HF in Italy have 56% risk to experience a new hospital admission within one year since their discharge (6); interestingly, almost half of these new hospital admissions (49%) are due to non-cardiovascular reasons, meaning that patients with cardiovascular disease require a comprehensive, multidisciplinary monitoring. The same study showed that the Italian National Healthcare Service (NHS, or SSN -Servizio Sanitario Nazionale-) spends about €550 million every year for these patients, with each hospital admission costing €11,867, and with hospital readmissions being approximately twice more expensive than first admissions (6).
Management of HF is complex, quite often, patients who carry cardiac implantable electronic devices (CIEDs) also present other chronic conditions (such as diabetes, chronic obstructive pulmonary disease, cognitive impairment, osteo-articular diseases, etc.), have reduced life expectancy, poor quality of life, and the highest risk of hospital admission among any other disease in the western world (7).
An increasing number of patients with heart failure receive implantable cardioverter-defibrillators (ICDs) or cardiac resynchronization defibrillators (CRT-Ds) with remote monitoring (RM) function. Early detection of worsening heart failure, enabled by the regular collection and monitoring of predisposing factors or symptoms (such as weight, heart rate, and blood pressure) can help patients and physicians to adjust therapy or timely intervene in case of anomalies, thus improving clinical outcomes (8, 9). Also implanted therapeutic devices can provide, wirelessly and remotely, information on the device itself (generator and lead function), that are useful to verify the appropriate functioning (8, 9).
For all these reasons, the use of RM in patients with HF, and left ventricular systolic dysfunction, treated with implantable cardioverter-defibrillators (ICDs) or cardiac resynchronization therapy defibrillators (CRT-Ds) may improve efficiency of care, drives decision making, and has the potential of reducing the burden of hospital admissions for HF and other major cardiovascular events (10, 11).
For instance, a systematic review conducted in 2017 identified 39 relevant trials of RM, using non-implanted systems and largely based on assessments of symptoms, weight, blood pressure, heart rate and rhythm (12). The meta-analysis showed that RM was associated with a reduction in all-cause mortality of 20% and HF hospitalization of 37% (12). Finally, the adoption of RM has been proven to be an efficient way of monitoring HF patients in situations during which there is an important need of reducing or interrupting face-to-face consultations, like the recent COVID-19 pandemic (13–16).
Thanks to this compelling evidence, the Healthcare Service of Trento (Italy) has made the decision of funding RM for patients who carry CIEDs and has set up an ambulatory tariff for hospitals in charge of this service.
The aim of this observational, retrospective study, promoted by the Cardiology Unit of the Santa Chiara Hospital, was to conduct an assessment on the clinical and economic consequences of remotely monitoring patients treated with ICDs or CRT-Ds, comparing two alternatives: patients monitored through remote monitoring (hereafter, “RM”), vs. patients monitored through standard, in-office cardiology visits (hereafter, “SM”).
Material and methods DataClinical and resource consumption data for this retrospective analysis were extracted from the Electrophysiology Registry of the Trento Cardiology Unit, which has been systemically collecting patient information from January 2011 to February 2022.
The study protocol was approved by the local ethics committee. The investigation conformed to the principles outlined in the Declaration of Helsinki. All patients gave written informed consent, and data were treated confidentially.
The study population consisted of adult patients (aged ≥18 years), who: (i) received either ICD or CRT-D therapy; (ii) were discharged alive from the hospital, after implantation; (iii) were monitored with either RM or standard in-office cardiology visits; (iv) were followed up by the Electrophysiology Unit of the Santa Chiara Hospital (i.e., data were properly tracked in the registry) for at least 2 years (study period), or died before the end of the study period. Patient observation started at the date of CIED implantation, which served as index date.
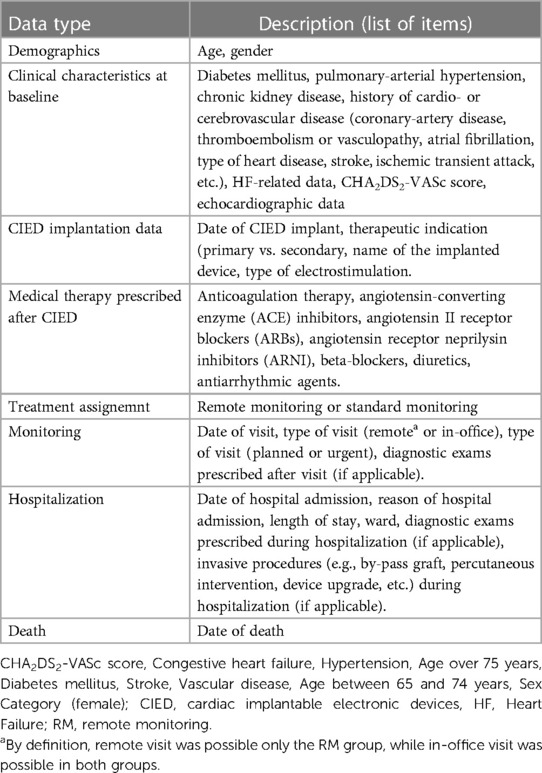
Demographic and clinical characteristics of CIED implanted patients were collected to identify potential differences between the two groups (remote vs. standard monitoring; (Table 1), then clinical and economic data of these patients were collected.
Table 1. Summary of data collected in the Trento registry.
The Remote Monitoring is carried out daily (weekdays) and provides for the analysis of alarms according to a color code. It is performed by two appropriately trained dedicated nurses who consult with the electrophysiologist cardiologist as needed. The basic parameters of the devices were always re-checked during the visit in presence (sensing, impedances, threshold, programming, battery life).
The physicians involved in remote monitoring activities are the same ones who also carry out outpatient visits and they are part of the electrophysiology team of the Trento Hospital Cardiology.
Patients with a defibrillator undergo a scheduled outpatient visit once a year. Extra visits (unscheduled visits) were based on the severity of the remote monitoring alarm.
From a clinical standpoint, survival analysis was conducted, and incidence of CV-related hospitalizations was measured. From an economic standpoint, direct costs (RM implementation, planned and unplanned in-office visits, laboratory and instrumental diagnostic examinations, hospital admissions) were summed up to estimate the cost per treated patient over a 2-year time horizon, and adopting two different perspectives: (i) the payer perspective (Trento Healthcare Service); (ii) the provider perspective (Santa Chiara hospital).
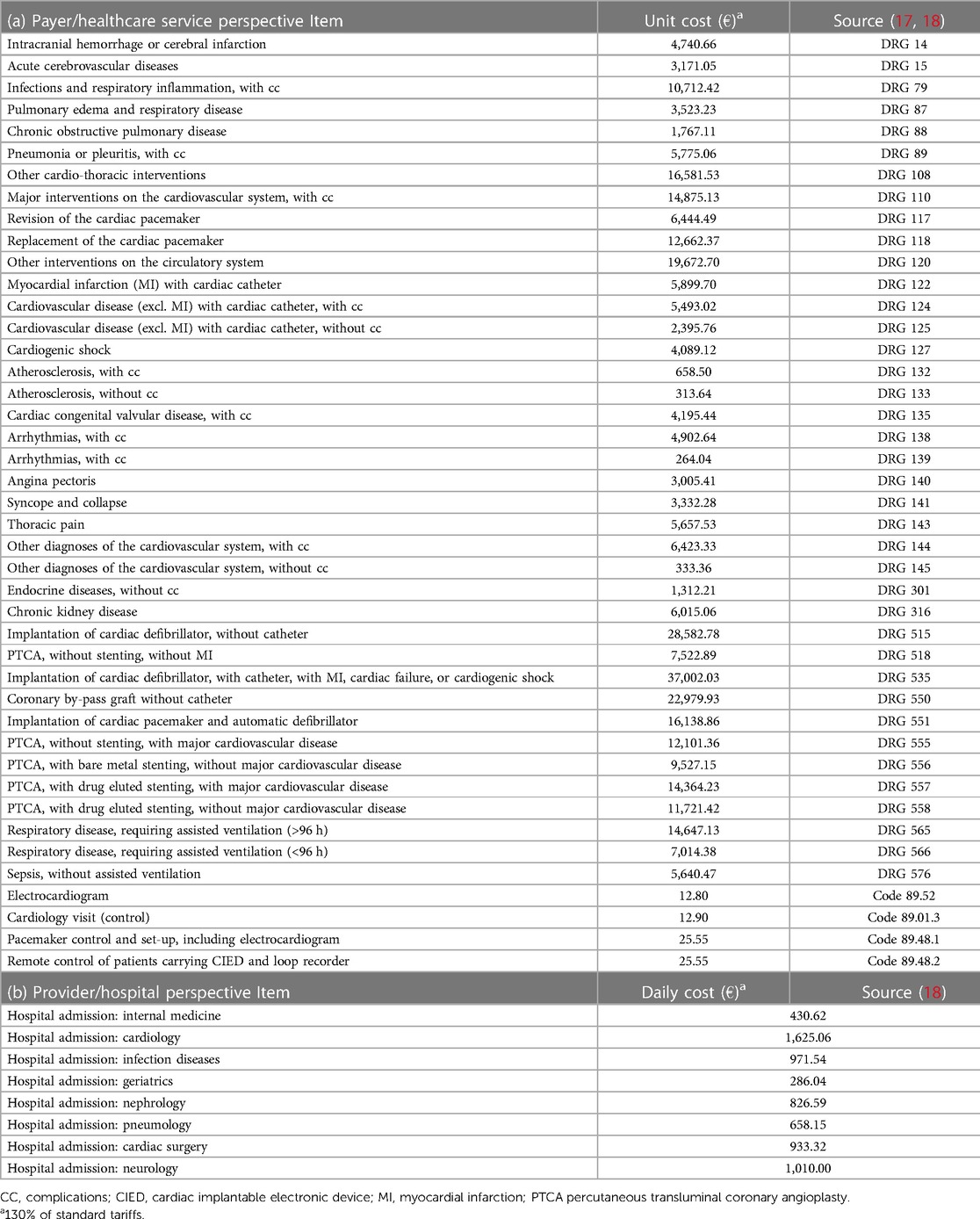
Cost analysis: payer (healthcare service) perspectiveTable 2a shows the unit costs that were used to estimate the economic impact adopting the payer perspective. The payer perspective captured the costs the Trento Healthcare Service covered to manage the study population during the 2-year observation period. These costs depend on the current tariffs (for both inpatient and outpatient services) the Healthcare Service remunerates hospitals and other healthcare providers with. For the inpatient care, the cost of hospital admissions corresponds to the DRG tariffs issued by the Healthcare Service [“Nomenclatore tariffario delle prestazioni di ricovero per acuti della Provincia Autonoma di Trento”(17)]; similarly, for outpatient care, the cost of visits, exams, etc. was retrieved from the formulary of outpatient services issued by the Healthcare Service [“Nomenclatore tariffario delle prestazioni di assistenza specialistica ambulatoriale della Provincia Autonoma di Trento”(18)].
Two different providers perform control visits in the Trento territory: (i) the heart failure (HF) ambulatory; (ii) the electrophysiology (EF) ambulatory. The associated cost of the two visits is slightly different, and such difference was captured in the analysis. The cost of the in-office visit in the HF ambulatory amounts to €25.70, consisting in a control visit (€12.90; Code 89.01.3), plus electrocardiogram (ECG; €12.80; Code 89.52). The cost of the in-office visit in the EF ambulatory amounts to €38.45, consisting in a control visit (€12.90; Code 89.01.3), plus pacemaker control (€25.55; Code 89.48.1) (18).
Cost analysis: provider (hospital) perspectiveThe provider perspective captured the production costs the hospitals sustain to deliver care to the CIED patients. The inpatient costs were calculated by multiplying the daily cost of hospital stay (depending on the ward; as calculated by the management & control department of the Santa Chiara Hospital, Trento), by the length of each hospitalization. Table 2b shows the hospital daily costs, recently calculated by the hospital [2019 (19)]). The cost of provision of outpatient and in-office visits was calculated considering staffing costs (€73/hour for physicians and €28/hour for assistant nurses). It was assumed that the duration of an in-office visit was half an hour, and that both a physician and a nurse would be needed during the visit. Since it was not possible to accurately determine the fixed costs of ambulatory care (i.e., room occupation), it was assumed that they would have minimal impact on the total cost of healthcare provision, and they were calculated as 10% mark-up of the staffing costs. The resulting cost was €55.55 per in-office visit (€73/hour × 0.5 h + €0.28/hours × 0.5 h), in the hospital perspective. The cost of RM, amounting to €68.20 per patient/year, was calculated taking into account that, a patient population of about N = 900 patients would require 1 full-time equivalent nurse (∼€45.3 thousands/year for a nurse paid €28/hour for 7.36 h/day and 220 working days/year) and 1 h-time equivalent physician (∼€16.1 thousands/year for a physician paid €73/hour for 1 h/day and 220 working days/year).
Table 2. Unit costs in the payer/healthcare service (a) and provider/hospital (b) perspective.
Statistical analysisDescriptive analyses and simple parametric and non-parametric testing (t-test and chi-square test) were used to identify potential differences at baseline between the RM and SM groups, as this study did not have randomized design. Because of the lack of balance for some of these characteristics (Supplementary Table S1), propensity score matching (PSM) was used to adjust the selection bias of assigning patients to the remote monitoring group. Covariates that were input in the probit regression model determining the PSM were as follows: age, gender, type of implanted device (CRT-D, cardiac resynchronization therapy defibrillator; ICD, implantable cardioverter-defibrillator), diagnosis of stroke or transient of ischemic attack, myocardial infarction, atrial fibrillation, deep vein thrombosis, aortic stenosis, category of left ventricular ejection fraction, New York Health Association (NYHA) class.
After PSM adjustment, standard statistical tests were conducted to assess potential differences among RM and SM groups. Survival curves and event rates in the matched population were estimated using the Kaplan-Meier method, and log-rank test. Binary outcomes (e.g., proportion of patients with at least one hospitalization) were compared by using non parametric test of proportions, while continuous variables (e.g., costs) were compared by using parametric t-test. Finally, for costs a mixed approach of testing difference with both parametric and non-parametric tests was preferred. All statistical data were analyzed using the Stata 13 software.
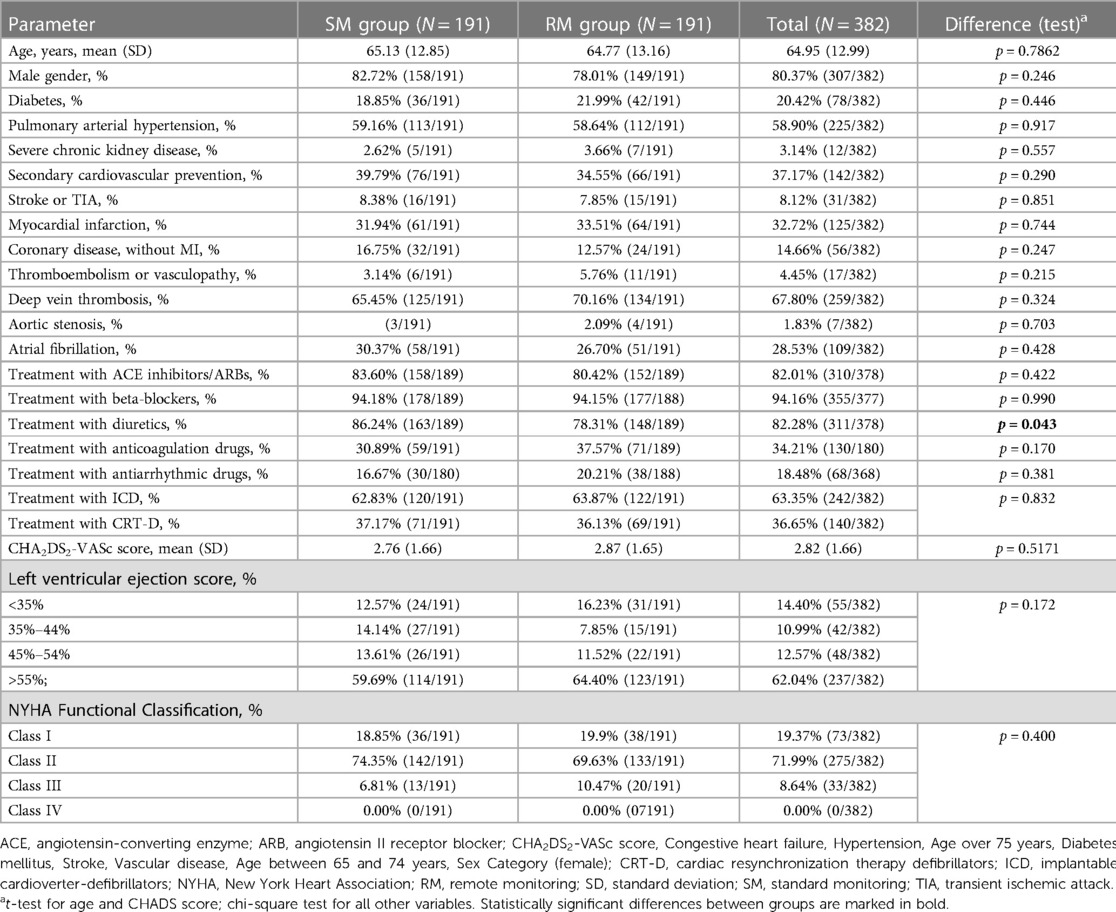
Results Baseline characteristics and adjustment after propensity score matchingIn the enrollment period (January 2011 to February 2022), N = 402 patients carrying either ICD or CRT-D devices met the inclusion criteria and were included in the analysis. Among the population of N = 402 patients overall, N = 189 patients (47.0% of the cohort), mainly enrolled in early years (2011 or 2012), were followed through SM, while the remaining N = 213 patients (53.0% of the cohort) entered the RM program, which consisted of regular RM control plus in-office visits. Given some imbalance of baseline characteristics (overall, the SM cohort seemed more severe than the RM cohort, and some differences were statistically significant at the p = 0.05 level; Supplementary Table S1), PSM with common support was applied to minimize such differences and minimize effect of confounding factors on the outcomes. A probit regression model was used to identify variables predicting assignment to the RM group (Supplementary Figure S1). The PSM model was efficient, with only 3 out of 194 valid RM observations being not suitable for control matching. After matching, baseline characteristics of the two groups were balanced, except for the proportion of patients treated with diuretics (Table 3).
Table 3. Patients’ charactristics at baseline (after propensity score macthing).
There were N = 42 episodes of device malfunctioning in N = 36 patients, of whom N = 13 were managed through remote control (only one third of the patients with malfunction). This suggests that RM may provide early indications of functional problems and avoid device malfunctioning. None of these N = 42 episodes were correlated with patient death.
There were N = 97 interventions of device change in N = 97 patients, of whom N = 49 were managed through remote control. The information about explant is not available in the database.
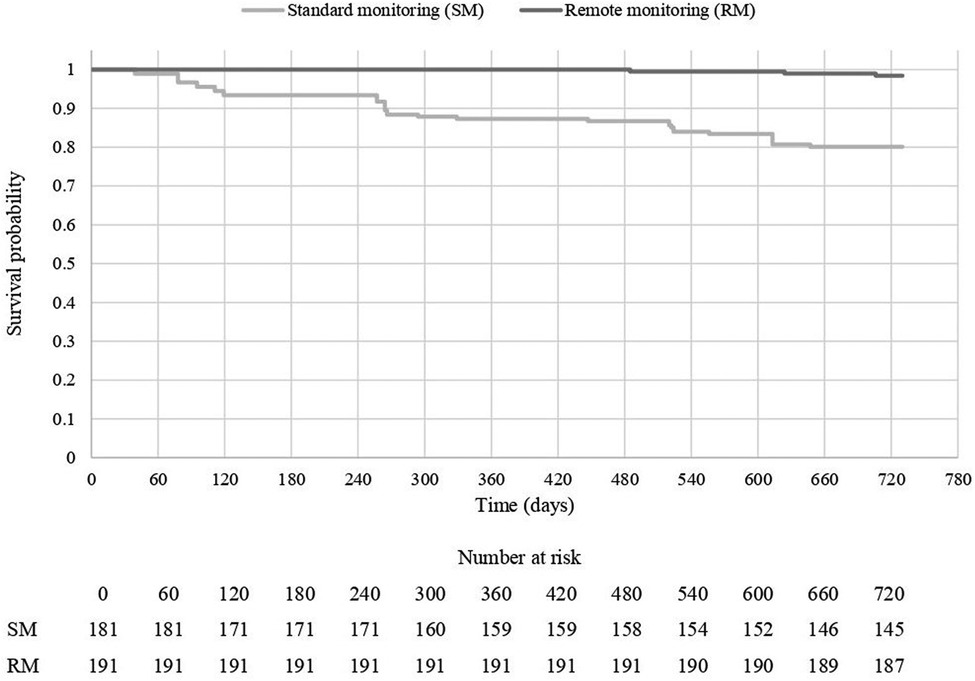
Survival and CV-related hospitalization ratesFrom a clinical perspective, the association between RM and mortality (for any cause), as well as CV-related morbidity was assessed. After a follow-up of 2 years since CIED implantation, mortality rate for any cause was 1.6% (N = 3 out of 191 patients) in the RM group and 19.9% (N = 36 out of 191 patients) in the SM group (log-rank test, p < 0.0001; Figure 1).
Figure 1. 2-year mortality (any cause), by treatment group.
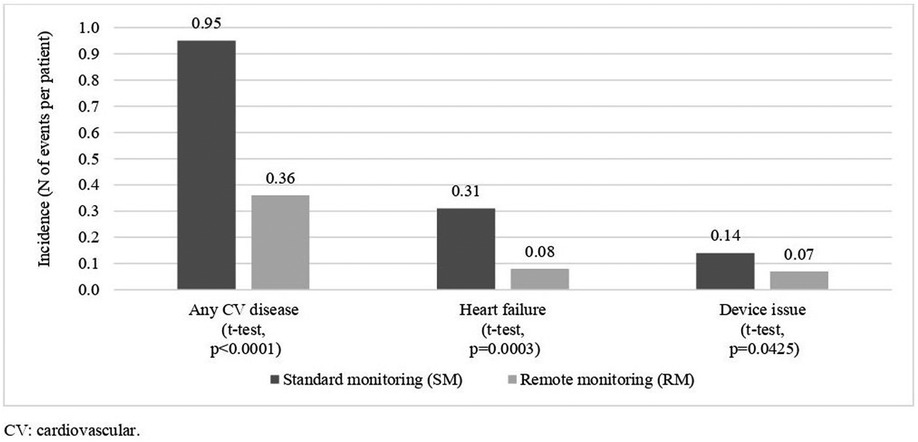
During the study period, a lower proportion of patients in the RM group, 25.1% (N = 48 out of 191 patients) were hospitalized for CV-related reasons, compared to the SM group (51.3%; N = 98 out of 191 patients; p < 0.0001, two-sample test for proportions). A similar lower rate of hospitalizations was observed for other types of hospitalizations, such as hospitalizations for heart failure (7.3% in the RM group, 18.8% in the SM group; p = 0.0008) and hospitalizations for device issues (5.2% in the RM group, 13.6% in the SM group; p = 0.0051). Figure 2 shows the 2-year incidence rates of hospitalizations for any CV cause, for heart failure, and for device issues in the two groups. The incidence rates of CV-related and HF-related hospitalizations were significantly lower in the RM group, compared to the SM group (p < 0.05). The length of stay per hospital admission was similar between the two groups (6.0 days/admission in the SM group, vs. 6.8 days days/admission in the RM group (p = 0.3619, two-sample t-test).
Figure 2. 2-year CV-hospitalization incidence rates, by treatment.
Interestingly, a similar number of in-office visits was registered in the RM group (4.51 visits/patient the 2-year period), vs. the SM group (4.32 visits/patient; (p = 0.5490, two-sample t-test), in contrast with the expected occurrence of more visits in the RM group, triggered by device alerts, inducing physicians to request a follow-up in-office visit to examine the patient.
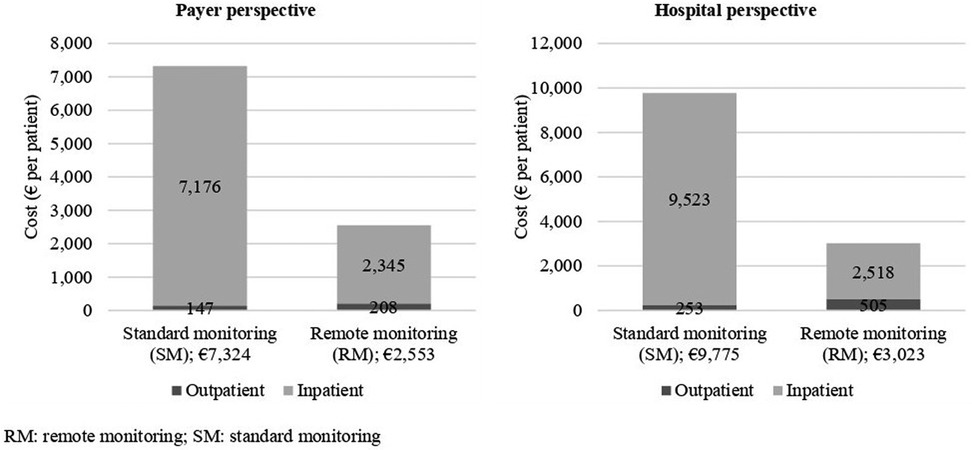
Costs for inpatient careAdopting the payer perspective, RM was associated with a lower average cost of hospital admission for any CV reason of 62% vs. SM. Over the 2-year period, costs were €2,345/patient and €7,176/patient in the RM and SM groups, respectively (difference: -€4,831; t-test, p < 0.0001). An even larger difference was also observed in the hospital perspective (where production costs, instead of DRG tariffs, were used to estimate the costs for the hospital). In the hospital perspective analysis, costs were €2,518/patient and €9,523/patient in the RM and SM groups, respectively (difference: −€-7,005; t-test, p < 0.0001). The large cost difference between the two groups was driven by the significant difference in the hospitalization rates, which favored the RM group.
Costs for outpatient careWhen tariffs were used to calculate the economic impact of outpatient care under the payer perspective, costs amounted to €147 in the SM group, and €207 in the RM group (difference: +€60; t-test, p < 0.0001), over the 2-year study period. As expected, implementation of RM lead to higher costs (+41%), that were attributable to the cost of RM visits, and to an increase of in-office visits triggered by RM control. A cost increase was also seen in terms of production costs, with costs in the RM group (€505) being 100% higher than in the SM group, €253 (difference: +€253; t-test, p < 0.0001).
Total cost of care (inpatient + outpatient care)Overall, the implementation of the RM program in the Trento territory emerged as cost saving in both payer and hospital perspectives. The relatively small investment required to fund RM (a fee for service in the payer perspective, and staffing costs for hospitals), was more than offset by the lower rate of hospitalizations for CV-related disease. Figure 3 shows that RM adoption generated savings of −€4,771 and −€6,752 per patient in 2 years, in the payer and hospital perspective, respectively.
Figure 3. Total cost of care, by (A) payer and (B) hospital perspective.
For completeness, few non-parametric tests were conducted to confirm the cost difference between RM and SM. First, we tested the proportion of patients exceeding a certain cost threshold of €1,000 in the follow-up period; this analysis confirmed that fewer patients had a cost above this threshold in the RM group (26.7%), compared to the SM group (51.3%; p < 0.0001, two-sample test for proportions). Second, when patients were stratified by cost quartiles, the distribution of patients was different in the two groups, with much fewer SM than RM patients in the highest quartile (16.75% vs. 30.37%, respectively; p < 0.0001, Pearson chi square test).
DiscussionThe organizational model for RM management, including the identification of roles and responsibilities, the involvement of healthcare professionals, and the setup of an action plan in response to CIED system of alarms, is crucial to optimize the efficiency of this intervention, and make sure it guarantees the “promised” results, namely improvement of clinical outcomes and reduction of acute care costs. Such organizational aspects have to be carefully considered, as important elements for explaining the clinical and economic results associated with RM implementation (20).
The RM management model currently used in the Trento Cardiology Unit of the Santa Chiara Hospital is the result of progressive changes that have fixed the initial issues and inefficiencies, while integrating the constant technological improvements in the cardiology space. Scientific literature has shown that adopting an efficient model is as important as selecting the best healthcare technologies and solutions for patients; even the most effective therapeutic intervention is destined to fail if it is not used properly (21–24).
This retrospective analysis of observational data provides evidence that RM of patients carrying CIEDs can have significantly lower short-term (2-year) morbidity and mortality risks, compared to standard monitoring based on the traditional in-office visit approach. These results are in line with the IN-TIME trial (11), and highlight a benefit not demonstrated by other prospective studies on remote monitoring with implanted devices (25–27).
The immediate, plausible consequence of this lower hospitalization rate is a significant drop of the inpatient costs, which alleviates the economic burden for the healthcare service. The reduction of hospital admissions in our Trento territory has generated savings from both payer and hospital perspective. The different saving observed in the two perspectives depends on the fact that while remuneration of inpatient services, through the DRG system, is fixed within a certain length of stay, production costs for the hospital increase almost linearly with length of stay. For instance, the remuneration for an episode of heart failure (DRG 127) amounts to €4,089, regardless the length of stay (provided that this is comprised between 2 and 21 days, otherwise beyond the 21st day, an additional remuneration of €263.02 applies), while the hospital cost of a 21-day stay would be about ten times higher than that of a 2-day stay. The implementation of the RM system led to a slight increase of both payer and hospital costs. More specifically, RM increased costs by €88 per patient/year in the payer perspective, and by €100 per patient/year in the hospital perspective. The increase of visits in the RM group (+33% compared to the SM group) deviates from what observed in literature, for example, in the RM-ALONE (10) and TARIFF (28) studies. However, the data used for the present analysis refer to about 40% of the total CIED population of the Trento territory, therefore we do not know (i.e., do not have complete data) whether this trend applied to the full cohort of patients. In any case, an increase of the in-office visits is still plausible. Patients under RM are followed through a system of “alerts & alarms”, and they could be called back by their physicians because of this exchange of information, which is critical to prevent further disease worsening. However, even if the RM model could be made more efficient and less expensive (perhaps by replacing some in-office visits with phone or video calls), the investment in RM is minimal and the return of investment for avoided hospitalization clearly offsets the investment. Alternatives to conventional methods of payment and reimbursement, such as risk-sharing arrangements have been proposed (29) and could be considered also for remote monitoring, in the settings where its value is of proven benefit. As for most observational studies, certain methodological issues could limit the validity of results of the present study. First, as already mentioned, the analysis, refers to less, than half of the CIED patients receiving care in our territory. Despite the sample was relatively large (N = 402 patients in total, N = 391 after propensity score matching) and we used propensity score matching to minimize selection bias, we cannot be totally sure the results would be the same, if the full cohort had been analysed; therefore, we aim to conduct a new analysis when data on the full cohort will be available. Of course, the facts 40% is a quite large proportion of the total portion of the full cohort and that results of the propensity matched analyses were not largely different from unadjusted comparison (not report in this article for the sake of simplicity), are encouraging signals the outputs of the analysis are reliable.
Therefore, based on real-world clinical experience of Hospital S. Chiara of Trento, the use of RM for the follow-up of patients carrying ICD and CRT-D appears associated with a reduced mortality for all causes and hospitalizations for cardiovascular causes, thus confirming the most positive findings reported in literature, which is not homogeneous with regard to the benefits associated with RM (20, 21, 24, 30–33).
The reduction of the hospitalization burden generates savings for both the hospital and the regional healthcare system, with respect of a modest increase in costs for the management of remote control. Although these initial observations need further confirmation (broader sample, longer follow-up) the organizational model seems efficient, and the current evidence suggests the strategy can be fine-tuned to become more cost-effective.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributionsConception and design of the work: MM, VL, FA, QS, MM, and BG. Substantial contributions to the acquisition of data for the work: VL, BE, DFCF, and MM. Substantial contributions to the analysis of data for the work: MM, DFCF, FA, and BG. Substantial contributions to the interpretation of data for the work: MM, DFCF, QS, FA, and BG. Drafting the work: MM, VL, QS, and BG. Revising the draft of the work critically for important intellectual content: DFCF, FA, MM, GF, CA, BPP, BR. Final approval of the version to be published: MM, VL, DFCF, FA, BE, QS, MM, GF, CA, BPP, BR, and BG. All authors contributed to the article and approved the submitted version.
FundingThis analysis was financially supported by Boston Scientific.
AcknowledgmentsThe authors would like to thank all participants who participated in the study.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1151167/full#supplementary-material
References1. Mensah GA, Wei GS, Sorlie PD, Fine LJ, Rosenberg Y, Kaufmann PG, et al. Decline in cardiovascular mortality: possible causes and implications. J Adolesc Health. (2017) 120:366–80. doi: 10.1161/CIRCRESAHA.116.309115
CrossRef Full Text | Google Scholar
2. Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, et al. Forecasting the impact of heart failure in the United States: a policy statement from the American heart association. Circ Heart Fail. (2013) 6(3):606–19. doi: 10.1161/HHF.0b013e318291329a
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Olofsson M, Jansson JH, Boman K. Predictors for hospitalizations in elderly patients with clinical symptoms of heart failure: a 10-year observational primary healthcare study. J Clin Gerontol Geriatr. (2016) 7(2):53–9. doi: 10.1016/j.jcgg.2015.11.001
CrossRef Full Text | Google Scholar
4. Díez-Villanueva P, Jiménez-Méndez C, Alfonso F. Heart failure in the elderly. J Geriatr Cardiol. (2021) 18(3):219. doi: 10.1161/CIRCHEARTFAILURE.117.004669
CrossRef Full Text | Google Scholar
5. Rethy L, Mccabe M, Pool LR, Vu THT, Kershaw KN, Yancy C, et al. Contemporary rates of hospitalization for heart failure in young and middle-aged adults in a diverse US state. Circ Cardiovasc Qual Outcomes. (2020) 13(11):e007014. doi: 10.1161/CIRCOUTCOMES.120.007014
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Maggioni AP, Orso F, Calabria S, Rossi E, Cinconze E, Baldasseroni S, et al. The real-world evidence of heart failure: findings from 41 413 patients of the ARNO database. Eur J Heart Fail. (2016) 18(4):402–10. doi: 10.1002/ejhf.471
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Cleland JGF, Swedbergb K, Follath F, Komajda M, Cohen-Solal A, Aguilar JC, et al. The EuroHeart failure survey programme—a survey on the quality of care among patients with heart failure in Europe part 1: patient characteristics and diagnosis. Eur Heart J. (2003) 24(5):442–63. doi: 10.1016/S0195-668X(02)00823-0
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Gardner RS, Singh JP, Stancak B, Nair DG, Cao M, Schulze C, et al. Heartlogic multisensor algorithm identifies patients during periods of significantly increased risk of heart failure events: results from the MultiSENSE study. Circ Hear Fail. (2018) 11(7). doi: 10.1136/jim-2016-000199
CrossRef Full Text | Google Scholar
9. Alotaibi S, Hernandez-Montfort J, Ali OE, El-Chilali K, Perez BA. Remote monitoring of implantable cardiac devices in heart failure patients: a systematic review and meta-analysis of randomized controlled trials. Heart Fail Rev. (2020) 25:469–79. doi: 10.1007/s10741-020-09923-1
PubMed Abstract | CrossRef Full Text | Google Scholar
10. García-Fernández FJ, Asensi JO, Romero R, Lozano IF, Larrazabal JM, Ferrer JM, et al. Safety and efficiency of a common and simplified protocol for pacemaker and defibrillator surveillance based on remote monitoring only: a long-term randomized trial (RM-ALONE). Eur Heart J. (2019) 40:1837–46. doi: 10.1016/j.hrthm.2016.09.008
CrossRef Full Text | Google Scholar
11. Hindricks G, Taborsky M, Glikson M, Heinrich U, Schumacher B, Katz A, et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): a randomised controlled trial. Lancet. (2014) 384(9943):583–90. doi: 10.1016/S0140-6736(14)61176-4
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Lin MH, Yuan WL, Huang TC, Zhang HF, Mai JT, Wang JF. Clinical effectiveness of telemedicine for chronic heart failure: a systematic review and meta-analysis. J Investig Med. (2017) 65(5):899–911. doi: 10.1136/jim-2016-000199
PubMed Abstract | CrossRef Full Text | Google Scholar
13. McDonagh TA, Metra M, Adamo M, Gardner R, Baumbach A, Böhm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2021) 42(36):3599–726. doi: 10.1093/eurheartj/ehab368
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Boriani G, Palmisano P, Guerra F, Bertini M, Zanotto G, Lavalle C, et al. Impact of COVID-19 pandemic on the clinical activities related to arrhythmias and electrophysiology in Italy: results of a survey promoted by AIAC (Italian association of arrhythmology and cardiac pacing). Intern Emerg Med. (2020) 15(8):1445–56. doi: 10.1007/s11739-020-02487-w
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Boriani G, Vitolo M. COVID-19 pandemic: complex interactions with the arrhythmic profile and the clinical course of patients with cardiovascular disease. Eur Heart J. (2021) 42(5):529–32. doi: 10.1093/eurheartj/ehaa958
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Boriani G, Guerra F, De Ponti R, D’Onofrio A, Accogli M, Bertini M, et al. Five waves of COVID-19 pandemic in Italy: results of a national survey evaluating the impact on activities related to arrhythmias, pacing, and electrophysiology promoted by AIAC (Italian association of arrhythmology and cardiac pacing). Intern Emerg Med. (2022) 18(1):1–13. doi: 10.1007/s11739-022-03140-4
CrossRef Full Text | Google Scholar
17. Provincia Autonoma di Trento. Deliberazione della Giunta Provinciale n. 936/2012 - Determinazione delle tariffe per le prestazioni di assistenza ospedaliera.
18. Provincia Autonoma Di Trento. Deliberazione di Giunta Provinciale 13.06.2016, n. 1010 - Integrazione del Nomenclatore delle prestazioni di assistenza specialistica ambulatoriale, di diagnostica per immagini e di laboratorio erogabili nell’ambito del Servi.
19. Azienda Provinciale per i Servizi Sanitari (APSS) Trento. Internal costs registered by the controlling department of APSS.
20. van Steenbergen G, Ben Jaddi O, Theuns D, van Veghel D, Dekker L, Simmers T. The value of remote care in the reduction of healthcare utilization in implantable cardioverter-defibrillator patients. Pacing Clin Electrophysiol. (2021) 44(12):2005–14. doi: 10.1111/pace.14390
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Imberti JF, Vitolo M, Boriani G. Remote monitoring of cardiac implantable electronic devices: from data to clinical actions. Acta Cardiol. (2022) 5. doi: 10.1080/00015385.2022.2118955
CrossRef Full Text | Google Scholar
22. Zanotto G, Melissano D, Baccillieri S, Campana A, Caravati F, Maines M, et al. Intrahospital organizational model of remote monitoring data sharing, for a global management of patients with cardiac implantable electronic devices: a document of the Italian association of arrhythmology and cardiac pacing. J Cardiovasc Med (Hagerstown). (2020) 21(3):171–81. doi: 10.2459/JCM.0000000000000912
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Palmisano P, Melissano D, Zanotto G, Perego GB, Toselli T, Landolina M, et al. Change in the use of remote monitoring of cardiac implantable electronic devices in Italian clinical practice over a 5-year period: results of two surveys promoted by the AIAC (Italian association of arrhythmology and cardiac pacing). J Cardiovasc Med (Hagerstown). (2020) 21(4):305–14. doi: 10.2459/JCM.0000000000000950
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Boriani G, Imberti JF, Vitolo M. Atrial fibrillation and remote monitoring through cardiac implantable electronic devices in heart failure patients. Eur J Heart Fail. (2020) 22(3):554–6. doi: 10.1002/ejhf.1745
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Boriani G, Da Costa A, Quesada A, Pietro RR, Favale S, Boscolo G, et al. Effects of remote monitoring on clinical outcomes and use of healthcare resources in heart failure patients with biventricular defibrillators: results of the MORE-CARE multicentre randomized controlled trial. Eur J Heart Fail. (2017) 19(3):416–25. doi: 10.1002/ejhf.626
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Morgan JM, Kitt S, Gill J, McComb JM, Andre Ng G, Raftery J, et al. Remote management of heart failure using implantable electronic devices. Eur Heart J. (2017) 38(30):2352–60. doi: 10.1093/eurheartj/ehx227
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Klersy C, Boriani G, De Silvestri A, Mairesse GH, Braunschweig F, Scotti V, et al. Effect of telemonitoring of cardiac implantable electronic devices on healthcare utilization: a meta-analysis of randomized controlled trials in patients with heart failure. Eur J Heart Fail. (2016) 18(2):195–204. doi: 10.1002/ejhf.470
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Ricci RP, Vicentini A, D’Onofrio A, Sagone A, Rovaris G, Padeletti L, et al. Economic analysis of remote monitoring of cardiac implantable electronic devices: results of the health economics evaluation registry for remote follow-up (TARIFF) study. Hear Rhythm. (2017) 14(1):50–7. doi: 10.1016/j.hrthm.2016.09.008
CrossRef Full Text | Google Scholar
29. Boriani G, Vitolo M, Svennberg E, Casado-Arroyo R, Merino JL, Leclercq C. Performance-based risk-sharing arrangements for devices and procedures in cardiac electrophysiology: an innovative perspective. Europace. (2022) 24(10):1541–7. doi: 10.1093/europace/euac045
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Zito A, Princi G, Romiti GF, Galli M, Basili S, Liuzzo G, et al. Device-based remote monitoring strategies for congestion-guided management of patients with heart failure: a systematic review and meta-analysis. Eur J Heart Fail. (2022) 24(12):2333–41. doi: 10.1002/ejhf.2655
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Sgreccia D, Mauro E, Vitolo M, Manicardi M, Valenti AC, Imberti JF, et al. Implantable cardioverter defibrillators and devices for cardiac resynchronization therapy: what perspective for patients’ apps combined with remote monitoring? Expert Rev Med Devices. (2022) 19(2):155–60. doi: 10.1080/17434440.2022.2038563
PubMed Abstract | CrossRef Full Text | Google Scholar
32. Imberti JF, Tosetti A, Mei DA, Maisano A, Boriani G. Remote monitoring and telemedicine in heart failure: implementation and benefits. Curr Cardiol Rep. (2021) 23(6):55. doi: 10.1007/s11886-021-01487-2
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Chew DS, Zarrabi M, You I, Morton J, Low A, Reyes L, et al. Clinical and economic outcomes associated with remote monitoring for cardiac implantable electronic devices: a population-based analysis. Can J Cardiol. (2022) 38(6):736–44. doi: 10.1016/j.cjca.2022.01.022
留言 (0)