
記住我








Patients may feel better prepared and thus more able to participate actively in decisions concerning their treatment when they get a decision coaching and/or decision aid before the consultation takes place. Therefore, usual care, i.e. standard consultation with the physician without decision aid and/or decision coaching, was chosen as comparator. Patients without additional decisional support are expected to participate less in the consultation.
Intervention descriptionEligible patients will be randomized in equal proportions between the intervention group (i.e., decision coaching with decision aid) and the control group (i.e., usual care/standard consultation) according to the characteristic of preferred decision-making at baseline (expressions: physician should decide; patient would like to decide alone; patient and physician should decide together).
Intervention groupThe intervention consists of the use of the decision aid, accompanied by a decision coaching session.
Decision aidThe decision aid HELP consists of a brochure for defining information and decision-making needs, including the patient’s personal values, as well as an overview of the most common forms of therapy. Both components are also available in digitalized form as a web app (htttps://awhelp.herokuappcom/#/).
The brochure entitled “What is important to me for my treatment?” includes questions on the patient’s information needs (e.g., information on the disease, treatment options, and side effects) and a section with questions on the patient’s decision-making behavior, i.e., how or with whom they want to make the treatment decision (alone, with the doctor, with relatives). The brochure ends with a clarification of the patient’s personal values (value clarification) and a section for open questions for the physician.
The second brochure entitled “Overview of common forms of therapy” includes information about the process, effect, duration and effort, side effects, and advantages vs. risks of common therapies, i.e., palliative therapy, chemotherapy, radiotherapy, immunotherapies, and targeted therapies.
Decision coachingThe coaching takes place in person or, if necessary, by telephone or online. The coaching process follows the sections of the HELP decision aid: patient’s information needs, the preferred method of decision-making, and the clarification of central personal values.
After the coaching session and before the consultation with the physician, participants fill in the questionnaires (Decisional Conflict Scale, Decision Self-Efficacy Scale, Preparation for Decision Making Scale, EQ 5D, Hospital Anxiety and Depression Scale) before their consultation with the physician. After the consultation, the post-survey questionnaires are handed out or mailed to participants (Patient Involvement in Care Scale, EQ-5D, Hospital Anxiety and Depression Scale).
Control groupThe participants in the control group get usual care, i.e., the doctor-patient conversation takes place without preliminary coaching and deliberation about their preferences and goals.
Before the consultation with their physician, participants fill in the pre-survey questionnaires (Decisional Conflict Scale, Decision Self-Efficacy Scale, EQ 5D, Hospital Anxiety and Depression Scale). After the consultation, the post-survey questionnaires are handed out or mailed to them (Patient Involvement in Care Scale, EQ-5D, Hospital Anxiety and Depression Scale).
Criteria for discontinuing or modifying allocated interventionsPatients can leave the study at any time for any reason, without any consequences. If a patient’s health status declines and they are no longer able to answer the survey questions, they will be treated as a dropout. The same applies for participants who withdraw their consent for any other reason. Patient data collected up to that moment will not be included in the analysis.
Strategies to improve adherence to interventionsThe adherence to fill out the questionnaires before and after the conversation with the physician takes place is ensured by friendly reminders via phone call or mail. Intervention adherence, i.e., ensuring that patients show up for the arranged coaching session, is ensured by reminding patients via phone call one day ahead of the appointment.
Relevant concomitant care permitted or prohibited during the trialAs the intervention does not consist of any form of medical treatment, there are no restrictions concerning medical treatments.
Provisions for post-trial careNo provisions for ancillary and post-trial care will be provided, due to the absence of any physical intervention and the shortness of study.
OutcomesThe main objective is to investigate the effectiveness of the developed decision support and decision coaching for lung cancer patients. Effects will be measured by the sum score of the dimension “clarity of personal attitude” (items 4-6) of the Decisional Conflict Scale (DCS) [16, 17] after the decision coaching.
In addition, the effects of the HELP intervention on patients’ self-efficacy, their perceived preparation for and participation in treatment decision-making, and the patients’ emotional state will be assessed.
Primary outcomeThe primary outcome is the sum score of the dimension “clarity of personal attitude” in the Decisional Conflict Scale (DCS) after the decision coaching has taken place. The questionnaire is validated in German and shows good reliability [16, 17].
A clinically relevant difference of 10 points in the primary outcome between the two treatment groups was assumed to be appropriate for case planning.
Secondary outcomesSecondary outcomes are the effects of the HELP intervention on patients’ self-efficacy, their perceived preparation for and involvement in treatment decision-making, and their emotional state. All questionnaires listed in Table 1 are validated and show good reliability (see item 18b).
Table 1 Outcomes and instrumentsParticipant timelineParticipation in the study includes the completion of two questionnaires for each participant (before and after the medical consultation at intervals of 1–4 weeks). The questionnaires will be handed over personally (including a stamped return envelope) or sent by e-mail. The time needed to answer the questionnaires is about 10 min.
In addition to the questionnaire survey, the application of the decision aid incl. decision coaching will be carried out with participants in the intervention group. This can take place, depending on the patient’s wishes, either in the clinic or at another location, by telephone or by video conference. The time frame is about 30–45 min for the decision aid and the accompanying conversation. Appointments are made in person, by phone, or by mail.
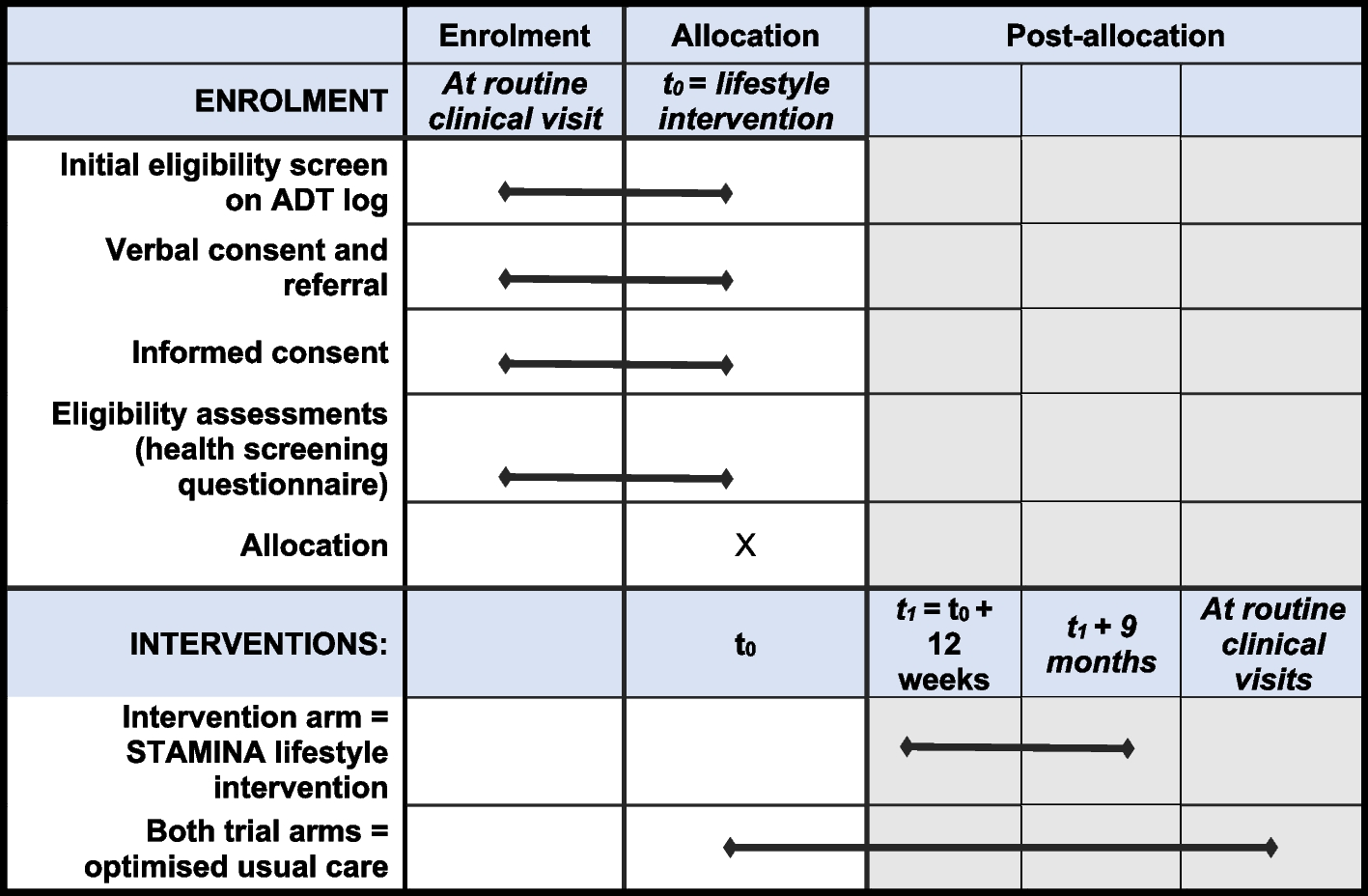
The total study-related time required is therefore about 20 min for persons who participate exclusively in the questionnaire survey and about 50 to a maximum of 65 min for persons who are invited both to the questionnaire survey and to the decision coaching (Figs. 1 and 2).
Fig. 1
Schedule of enrolment, interventions, events, and assessments (SPIRIT figure). ** Timepoint: t3= consultation with physician (decision making), −t1 and t0 = 6–8 days before physician consultation, t1 and t2 = 2–5 days before physician consultation, t4 = 1–14 days after physician consultation
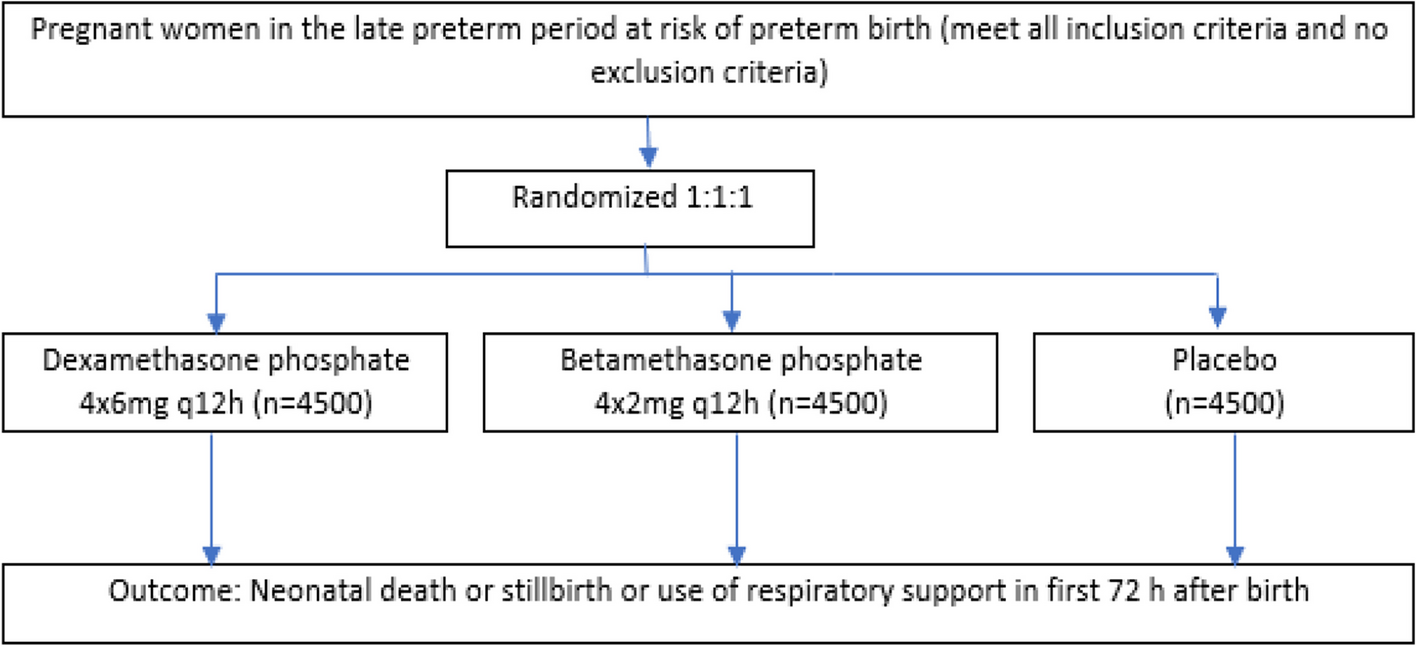
Fig. 2 Sample size
Sample size A clinically relevant difference of 10 points in the primary outcome between the two treatment groups was assumed to show a sufficient clinical difference for case planning. In addition, the standard deviation was estimated to be 20.6 from the literature [12]. Under these assumptions, n=71 patients per group are needed to demonstrate the assumed difference between the two groups at a two-sided significance level of 5% with a power of 80% using a Mann-Whitney U test. The calculation was performed by means of 100,000 simulation runs using the case number software PASS v 16.0.4. Taking into account a dropout rate of approx. 20%, 71/(1–0.20)=89 patients per group are included. These results in a total number of cases of n=178 patients are to be included in the study.
RecruitmentPatients are identified by the recruiting research assistants in CT- and indication conferences and tumor board meetings and on oncological wards. If patients meeting the eligibility criteria are identified, recruitment takes place when the patients are in the clinic for their examination appointments like MRT, bronchoscopy, etc. The expected recruitment rate is five to eight patients per week from March 2022 to December 2022.
The research assistants introduce themselves and the study to the patients and, if patients are willing to participate, they get the information sheet and sign the consent form. After that, randomization takes place.
留言 (0)