Factors associated with the need for long-term total parenteral nutrition in survivors of acute superior mesenteric artery occlusion
Background
Acute superior mesenteric artery (SMA) occlusion is an uncommon condition associated with high mortality. If extensive bowel resection is performed for patients with acute SMA occlusion and the patient survives, long-term total parenteral nutrition (TPN) may be needed due to short bowel syndrome. This study examined factors associated with the need for long-term TPN after the treatment of acute SMA occlusion.
Methods
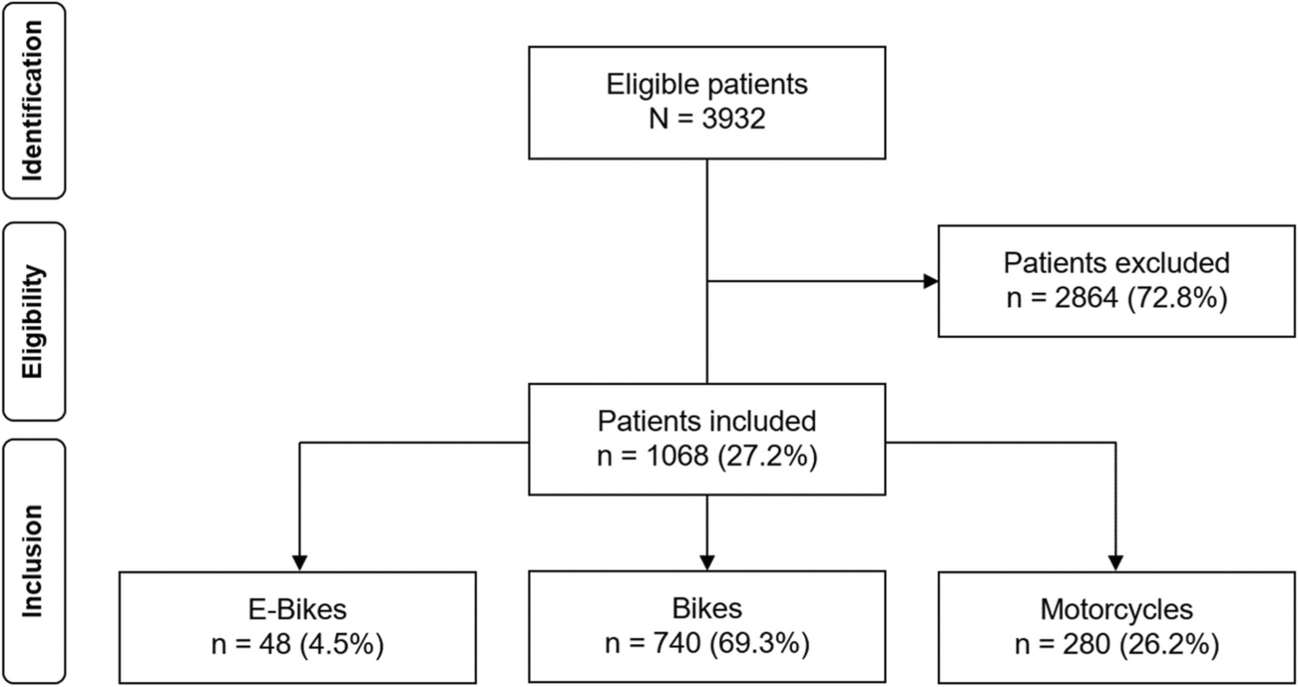
We retrospectively analyzed 78 patients with acute SMA occlusion. Patients were abstracted from a Japanese database from institutions with at least 10 patients with acute SMA occlusive disease from January 2015 through December 2020
Results
Among the initial cohort there were 41/78 survivors. Of these, 14/41 (34%) required permanent TPN who were compared with those who did not require long-term TPN (27/41, 66%). Compared to patients in the non-TPN group, those in the TPN group had significantly shorter remaining small intestine (90.7 cm vs. 218 cm, P<0.01), more patients with time from onset to intervention >6 hours (P=0.02), pneumatosis intestinalis on enhanced computed tomography scan (P=0.04), ascites (Odds Ratio 11.6, P<0.01), and a positive smaller superior mesenteric vein sign (P= 0.03). These were considered significant risk factors for needing long-term TPN. Age, gender, underlying disease, presence of peritoneal sign, presence of shock requiring vasopressors, site of obstruction (proximal vs. distal), and initial treatment (surgery vs. interventional radiology vs. thrombolytic therapy) were not significantly different between the two groups. Long-term TPN was significantly associated with longer hospital stay (52 vs. 35 days, P=0.04). Multivariate analysis identified the presence of ascites as an independent risk factor for needing long-term TPN.
Conclusion
The need for permanent TPN after treatment of acute SMA occlusion is significantly associated with longer hospital stay, longer time to intervention, and characteristic imaging findings (pneumatosis intestinalis, ascites, Smaller SMV sign). Ascites is an independent risk factor.
Level of evidence
III.


留言 (0)