
記住我




Amyotrophic lateral sclerosis (ALS) is the most common problem of motor neuron diseases, being invariably characterized by the progressive degeneration of both upper and lower motor neurons (Hardiman et al., 2017). Respiratory failure is the most common cause of death in ALS patients and occurs generally after a median time of 2–3 years after disease onset but with great variability among patients according to different phenotypic features (Chio et al., 2022). Early prediction of respiratory failure in ALS is of undoubted importance to start ventilation at the right time. Several respiratory tests and arterial blood gas analysis (ABGs) parameters have been evaluated, showing a different efficacy in the correct evaluation of initial respiratory dysfunction among ALS phenotypes (Heiman-Patterson et al., 2018). In recent studies, maximum inspiratory pressure (MIP), overnight pulse oximetry (OvOx; Kelly et al., 2022), serum base excess (SBE), and carbonate (HCO3-; Manera et al., 2020) have been confirmed as the earliest predictors of respiratory dysfunction, being capable of detecting subtle muscle weakness and nocturnal hypoventilation.
Venous serum chloride reflects the degree of respiratory acidosis and correlates with carbonate (HCO3-) blood levels: respiratory acidosis pushes the renal proximal tubule to increase secretion of hydrogen ions, resulting in higher retention of sodium bicarbonate more than sodium chloride. Although this compensatory mechanism helps in ameliorating acidosis, the final result is compensatory metabolic alkalosis and decreased serum chloride concentrations.
Despite its wide availability and low cost, also considering evidence that comes from other chronic pulmonary conditions (Naal et al., 2018), few data on serum chloride as a prognostic marker exist in literature. Some studies, evaluating ALS clinical trial data (Stambler et al., 1998) and a prospective ALS patient cohort (Hadjikoutis, 2001), observed that serum chloride strictly correlates with prognosis and respiratory symptom development. However, in multidisciplinary ALS clinics, serum chloride is barely considered as a marker of impending respiratory failure (Melo et al., 1999), and many of the most recent studies on early predictors of respiratory decline did not even mention it (Michels et al., 2022).
In the present study, we evaluated serum chloride values at diagnosis as a prognostic biomarker for overall survival and non-invasive ventilation (NIV) adaptation in a retrospective center-based cohort of ALS patients.
2. Methods 2.1. Study populationWe collected all ALS patients with serum chloride assessment at diagnosis, identified through the Piemonte and Valle d’Aosta Register for ALS, and diagnosed between 1 January 2007 and 31 December 2019. All patients met the revised El Escorial diagnostic criteria for definite, probable and probable laboratory-supported ALS. We restricted analyses to individuals with available blood exam data within 3 months of ALS diagnosis. Previous and concomitant diseases were assessed, and participants with significant renal comorbidities or other medical conditions that could influence serum chloride levels were excluded. For each patient, we collected sex, date of onset, site of onset, date of diagnosis, ALSFRS-R at diagnosis, weight at diagnosis, weight before disease onset, forced vital capacity (FVC%) at diagnosis, serum chloride (mmol/L), serum sodium (mmol/L), serum potassium (mmol/L), white blood cell count (WBC, 109/L), neutrophils count (109/L), lymphocyte count (109/L), data of NIV start, and date of death/tracheostomy from 1 January 2007 until 31 December 2021 (censoring date). The ALSFRS slope at the time of diagnosis (ΔALSFRS-R) was calculated for each patient using the following formula: (48 – ALSFRS-R score at diagnosis)/(time from onset to diagnosis). Moreover, the neutrophil-to-lymphocyte ratio (NLR) was calculated and used as a marker of inflammatory status (Leone et al., 2022).
2.2. Statistical analysisDifferences of discrete and continuous variables of interest were analyzed using the χ2-test Mann–Whitney U-test, as appropriate. A p-value <0.05 was considered to be statistically significant. Correlation analysis among serum chloride, clinical features and exams, and other serum biomarkers was performed using Pearson’s correlation coefficient. Time-to-event analysis was modeled performing backward stepwise Cox regression (unadjusted and adjusted) and Kaplan–Meier curves with the log-rank test were then performed to predict survival and NIV start. The variables included in the time-to-event analysis have already been recognized as significant prognostic factors in previous studies (Calvo et al., 2017; Westeneng et al., 2018) and showed also in our cohort a significant prognostic effect in univariate analysis.
Anonymous data were collected in an Excel (Version 14.0.4760.1000, 64 bit) dataset. Data were analyzed using IBM SPSS Statistics for Windows, version 28.0.1.0 (Armonk, NY: IBM Corp.).
2.3. Standard protocol approvals, registrations, and patient consentsThe study design was approved by the Ethical Committee of the Azienda Ospedaliero-Universitaria Città della Salute (Prot. N. 0036344). All patients signed a written informed consent.
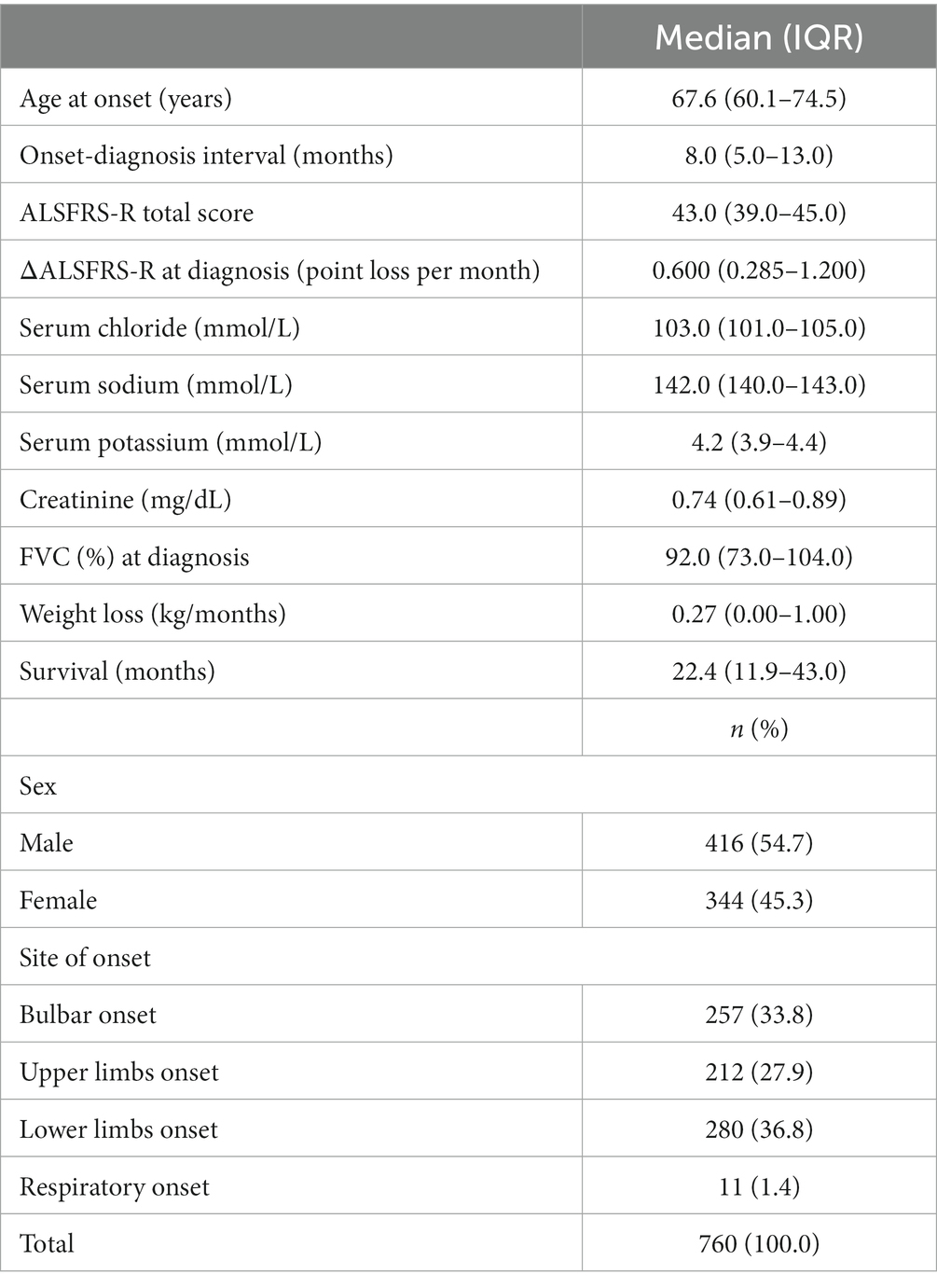
3. ResultsWe collected serum chloride values for 760 ALS patients at diagnosis. The descriptive statistics of the cohort are summarized in Table 1.
Table 1. Descriptive statistics.
Our population statistics generally reflected the median values of the general PARALS populations in terms of sex ratio, age at onset, site of onset, FVC%, and rate of progression. Median serum chloride values were 103.0 mmol/L (IQR 101.0–105.0 mmol/L), without showing any significant difference according to sex (Mann–Whitney U-test p = 0.936) and between patients with bulbar and spinal onset (Mann–Whitney U-test p = 0.329). Respiratory onset patients (N = 11) showed significantly lower serum chloride values when compared with other patients (median 98 mmol/L, IQR 94–105 mmol/L vs. median 103 mmol/L, IQR 101–105 mmol/L, p = 0.024).
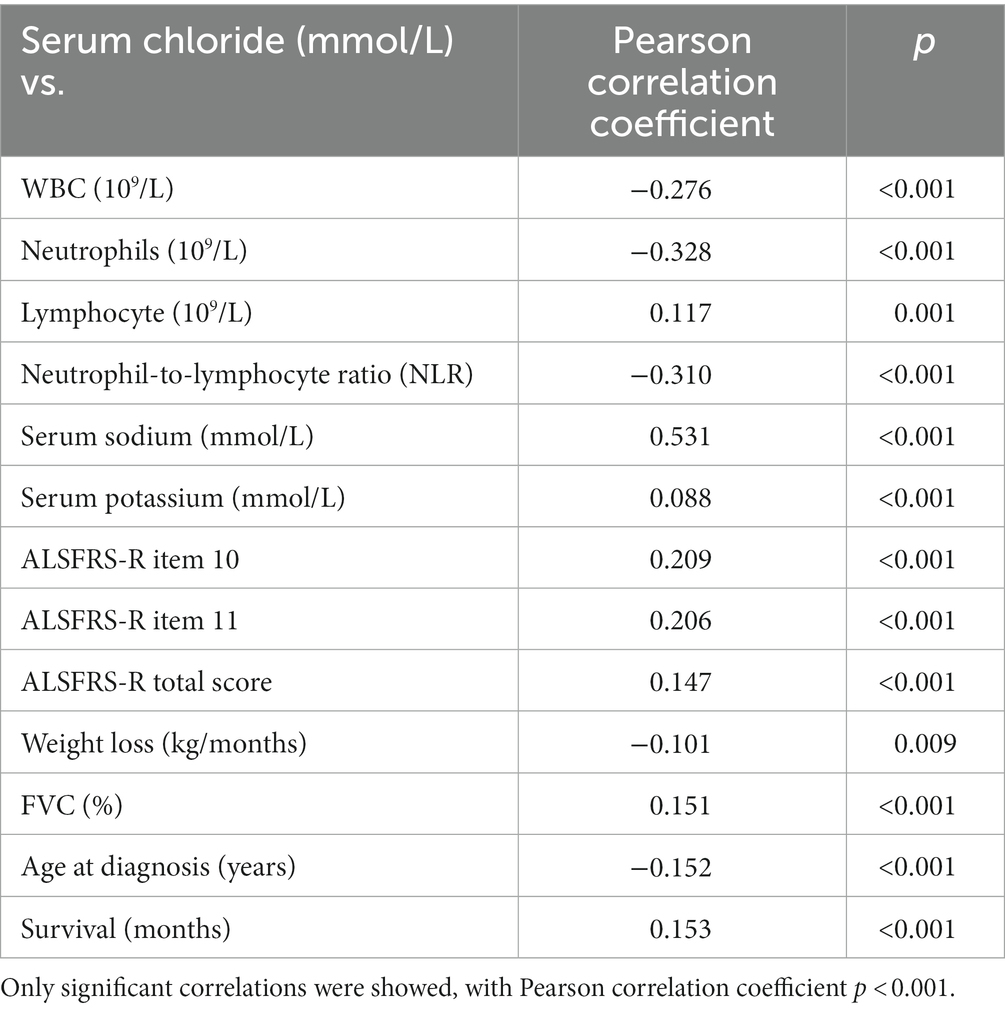
Correlation analysis (Table 2) pointed out significant negative low-moderate correlation between serum chloride and inflammatory status markers, such as WBC count, neutrophils count, and NLR, while a positive low correlation with lymphocyte count was found. Serum sodium was moderately correlated to serum chloride, and similarly, FVC%, ALSFRS-R item 10 and 11, and survival. Age at diagnosis and weight loss was negatively correlated with serum chloride values.
Table 2. Correlations between serum chloride at diagnosis and other clinical features and blood biomarkers.
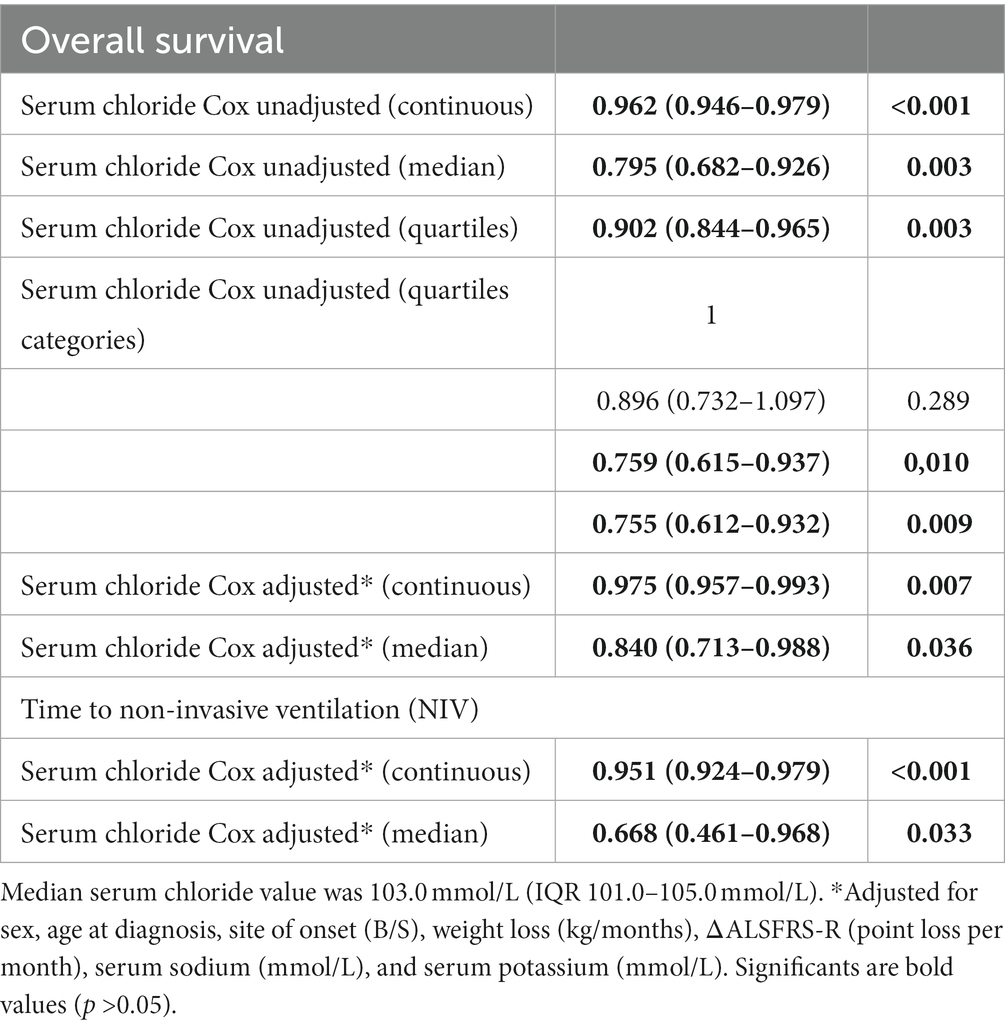
Time-to-event analysis confirmed both in univariate analysis and after multiple confounders’ adjustment that serum chloride value at diagnosis significantly influenced survival and time to NIV start (Table 3). A reduction in hazard ratio (HR) was observed by using both continuous values and after categorization: serum chloride >103.0 mmol/L determined an HR of 0.840 (IQR 0.713–0.988, p = 0.036) for death/tracheostomy and an HR of 0.668 (IQR 0.461–0.968, p = 0.033) for NIV start, after adjustment for sex, age at diagnosis, site of onset (B/S), weight loss (kg/months), ΔALSFRS-R (point loss per month), serum sodium (mmol/L), and serum potassium (mmol/L). Stratifying the Cox model by site of onset, serum chloride resulted to be highly predictive for NIV start in both bulbar onset (HR 0.850, IQR 0.766–0.942, p = 0.002) and spinal onset patients (HR 0.918, IQR 0.875–0.963, p < 0.001), while for respiratory onset patients, due to the limited number of patients (N = 11), the time-to-event analysis resulted in non-significance.
Table 3. Time-to-event analysis using Cox proportional hazard models.
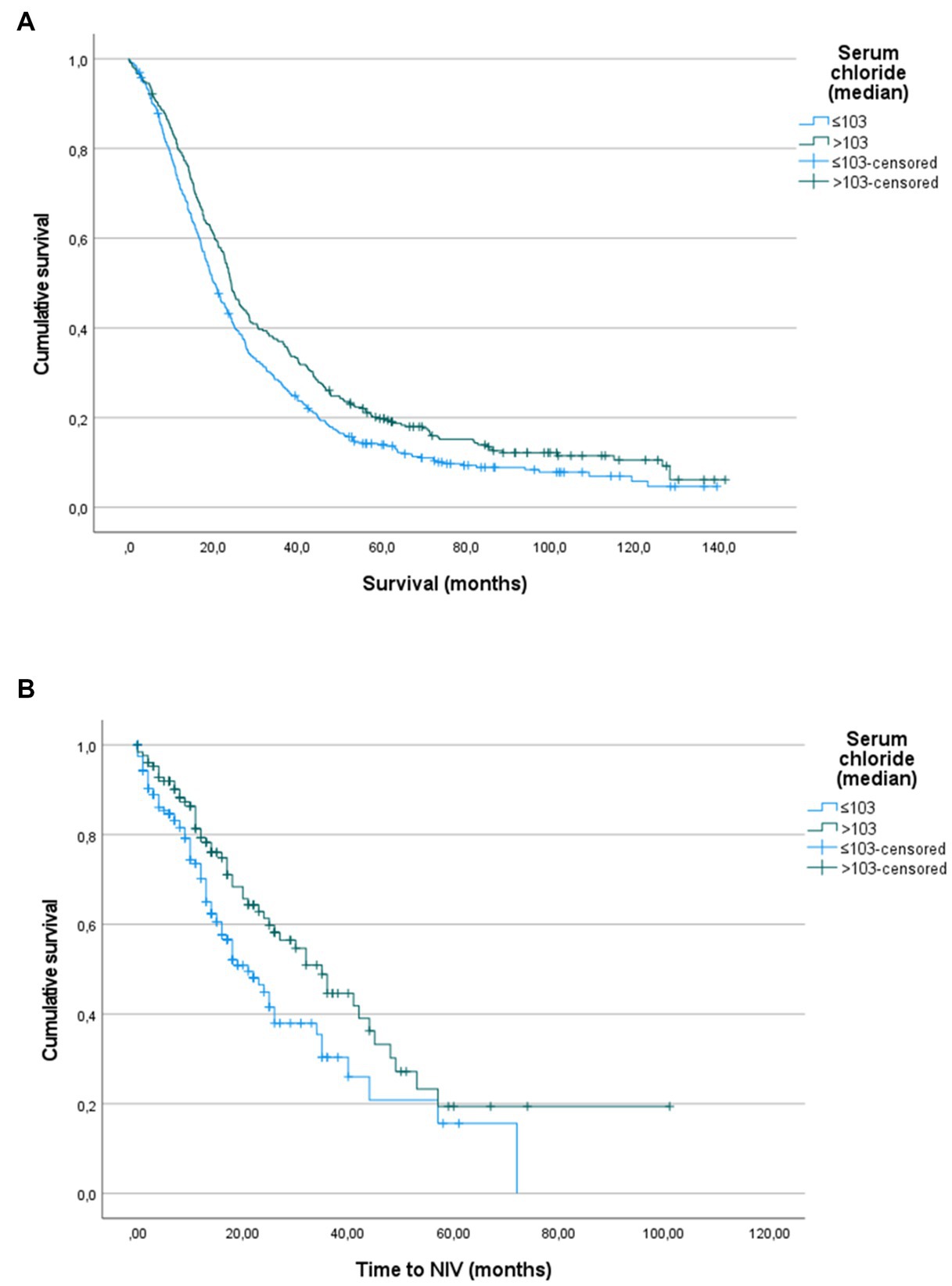
The Kaplan–Maier curves (Figure 1) confirmed this trend both for survival (p = 0.003, log-rank for pairwise comparison) and NIV indication (p = 0.010, log-rank for pairwise comparison).
Figure 1. (A) Kaplan–Meier analysis on overall survival, performed comparing patients divided by serum chloride median value (103.0 mmol/L). Log-rank test p = 0.003. (B) Kaplan–Meier analysis on time to non-invasive ventilation (NIV) start, performed comparing patients divided by serum chloride median value (103.0 mmol/L). Log-rank test p = 0.010.
4. DiscussionIn this study, we confirmed with solid analysis on a large cohort that serum chloride determined at diagnosis could be used as a low-cost marker of impending respiratory decompensation in ALS patients. Its easy availability, through venous blood sampling, allows to add it among the serum prognostic biomarkers that should be performed in the early phases of the disease in order to stratify patients into different prognostic categories.
Serum chloride has already been identified as a metabolic indicator of the degree of respiratory acidosis, also in ALS patients’ cohorts, but essentially using data from a clinical trial (245 patients enrolled in the placebo group of the ALS CNTF Treatment Study Group—ACTS study; Stambler et al., 1998) or from very small prospective cohorts followed up for a short time (23 ALS patients followed up for 15 months; Hadjikoutis, 2001).
In the ACTS study, the longitudinal evaluation of serum chloride and carbon dioxide allowed to observe that mean serum chloride declined slowly at first and then dropped sharply starting at nearly 4–5 months before death (Stambler et al., 1998). In our cohort, 22.1% of patients showed serum chloride ≤100 mmol/L and 10.3% values lower than 98 mmol/L being actually definable as hypochloremic at diagnosis.
Another study (Qureshi et al., 2008), using a random effects model multivariate analysis, observed that survival was shorter in participants who had low blood chloride (HR = 0.76, p = 0.020) or high bicarbonate levels (HR = 1.37, p = 0.006). Vital capacity declined faster in individuals with lower serum chloride (p < 0.0001), or higher bicarbonate (p = 0.002). Serum chloride at the baseline affected the rate of progression of the %VC, with a decrease by 0.62 in %VC slope for each serum chloride unit decreased. Lower chloride levels were also associated in our ALS patients with a faster ALSFRS-R rate of decline.
Serum chloride was also significantly associated with systemic inflammation, measured by the increase of neutrophils and NLR values in patients with low serum chloride. This could further confirm the role of serum chloride as a marker of nocturnal hypoventilation because several recent studies found a significant association between obstructive sleep apnea syndrome, nocturnal desaturation, and some inflammatory indexes, such as the NLR (Uygur et al., 2016; Bozkuş et al., 2018).
Despite these observations, the most recent studies on blood ALS biomarkers did not include serum chloride among the evaluated candidate (Sun et al., 2020). Moreover, the majority of studies on the predictive factors of respiratory decline mainly focused on respiratory symptoms, arterial blood gas parameters, and pulmonary function tests (Michels et al., 2022). Considering both the phenotype heterogeneity and the high variability of respiratory failure expression, the use of different respiratory measures as a complementary aspect helps to better assess different aspects of respiratory function as suggested (Murray et al., 2021).
NIV is generally considered as the mainstay treatment for decreasing respiratory muscle strength and respiratory failure, affecting both quality of life (the EFNS Task Force on Diagnosis and Management of Amyotrophic Lateral Sclerosis; Bourke et al., 2006; Piepers et al., 2006; Andersen et al., 2012) and survival (Lechtzin et al., 2007). A recent survey on NIV clinical use, evidenced a substantial lack of uniformity in NIV prescription across U.S. and Europe (Heiman-Patterson et al., 2018). To the best of our knowledge, serum chloride is not considered as a respiratory biomarker in any American or European guideline.
A possible study limitation is the absence of data on concomitant nocturnal oximetry, ABGs, and MIP/MEP tests, which could allow to confirm and further evaluate the relationship between serum chloride and early respiratory failure. This limitation is due to the retrospective nature of our study and needs to be addressed in future prospective studies. Moreover, we were not able to evaluate serum chloride values during disease progression due to the lack of longitudinal data systematically collected.
Nevertheless, our data suggest that serum chloride evaluation should be included as an effective and low-cost marker of hidden or impending respiratory failure in ALS patients. Its wide availability and operator independence confirmed its potential role both in spinal and bulbar onset patients, being able to provide screening information that could guide more detailed respiratory function tests.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThe studies involving human participants were reviewed and approved by Ethical Committee of the Azienda Ospedaliero-Universitaria Città della Salute (Prot. N. 0036344). The patients/participants provided their written informed consent to participate in this study.
Author contributionsUM and MG contributed to conception and design of the study and wrote the first draft of the manuscript. UM, MG, EM, AB, RV, MT, and PC organized the database. UM performed the statistical analysis. CM and ACan wrote sections of the manuscript. ACh and ACal revised the manuscript critically for important intellectual content. All authors contributed to manuscript revision, read, and approved the submitted version.
FundingThis study was in part supported by the Italian Ministry of Health (Ministero della Salute, Ricerca Sanitaria Finalizzata, grant RF-2016-02362405), the European Commission’s Health Seventh Framework Programme (FP7/2007–2013 under grant agreement 259867), the Italian Ministry of Education, University and Research (Progetti di Ricerca di Rilevante Interesse Nazionale, PRIN, grant 2017SNW5MB), the Joint Programme—Neurodegenerative Disease Research (Strength and Brain-Mend projects), granted by Italian Ministry of Education, University and Research, the European Union’s Horizon 2020 Research and Innovation Programme (Brainteaser Project, grant GA101017598). This study was performed under the Department of Excellence grant of the Italian Ministry of Education, University and Research to the “Rita Levi Montalcini” Department of Neuroscience, University of Torino, Italy.
AcknowledgmentsThe authors would like to thank to our colleagues Alessio Mattei, Nicola Launaro, Giuseppe Tabbia, Marco Michele Bardessono, Fulvia Ribolla, Michela Bellocchia, Paola Calvi, Chiara Chiappero, Luana Focaraccio, Elena Rindone, Cinzia Ferrero, Ennio Mantellini, Biagio Polla, Federica Arcadipane, Sabrina Dal Fior, Lorenzo Appendini, Alessandro Mastinu, Andrea Tagliabue, and Sandro Longu for their valuable collaboration in ALS patients’ respiratory management.
Conflict of interestACal received research grant from Cytokinetics. ACh served on scientific advisory boards for Mitsubishi Tanabe, Roche, Biogen, Denali Pharma, AC Immune, Biogen, Lilly, and Cytokinetics. The sponsor organizations had no role in data collection and analysis and did not participate to writing and approving the manuscript. The information reported in the manuscript has never been reported elsewhere.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ReferencesAndersen, P. M., Abrahams, S., Borasio, G. D., de Carvalho, M., Chio, A., Van Damme, P., et al. (2012). EFNS guidelines on the clinical Management of Amyotrophic Lateral Sclerosis (MALS) – revised report of an EFNS task force. Eur. J. Neurol. 19, 360–375. doi: 10.1111/j.1468-1331.2011.03501.x
CrossRef Full Text | Google Scholar
Bourke, S. C., Tomlinson, M., Williams, T. L., Bullock, R. E., Shaw, P. J., and Gibson, G. J. (2006). Effects of non-invasive ventilation on survival and quality of life in patients with amyotrophic lateral sclerosis: a randomised controlled trial. Lancet Neurol. 5, 140–147. doi: 10.1016/S1474-4422(05)70326-4
PubMed Abstract | CrossRef Full Text | Google Scholar
Bozkuş, F., Dikmen, N., Samur, A., Bilal, N., Atilla, N., and Arpağ, H. (2018). Obez olan ve olmayan OSAS’lı olgularda nötrofil lenfosit oranının önemi var mı? Tuberkuloz ve Toraks 66, 8–15. doi: 10.5578/tt.66535
PubMed Abstract | CrossRef Full Text | Google Scholar
Calvo, A., Moglia, C., Lunetta, C., Marinou, K., Ticozzi, N., Ferrante, G. D., et al. (2017). Factors predicting survival in ALS: a multicenter Italian study. J. Neurol. 264, 54–63. doi: 10.1007/s00415-016-8313-y
CrossRef Full Text | Google Scholar
Chio, A., Moglia, C., Canosa, A., Manera, U., Vasta, R., Grassano, M., et al. (2022). Respiratory support in a population-based ALS cohort: demographic, timing and survival determinants. J. Neurol. Neurosurg. Psychiatry 93, 1024–1026. doi: 10.1136/jnnp-2021-327968
PubMed Abstract | CrossRef Full Text | Google Scholar
Hadjikoutis, S. (2001). Venous serum chloride and bicarbonate measurements in the evaluation of respiratory function in motor neuron disease. QJM 94, 491–495. doi: 10.1093/qjmed/94.9.491
CrossRef Full Text | Google Scholar
Hardiman, O., Al-Chalabi, A., Chio, A., Corr, E. M., Logroscino, G., Robberecht, W., et al. (2017). Amyotrophic lateral sclerosis. Nat. Rev. Dis. Primers. 3:17071. doi: 10.1038/nrdp.2017.71
CrossRef Full Text | Google Scholar
Heiman-Patterson, T. D., Cudkowicz, M. E., De Carvalho, M., Genge, A., Hardiman, O., Jackson, C. E., et al. (2018). Amyotrophic lateral sclerosis and frontotemporal degeneration understanding the use of NIV in ALS: results of an international ALS specialist survey understanding the use of NIV in ALS: results of an international ALS specialist survey. Amyotroph Lateral Scler. Frontotemporal Degener. 19, 331–341. doi: 10.1080/21678421.2018.1457058
PubMed Abstract | CrossRef Full Text | Google Scholar
Kelly, C. R., Parra-Cantu, C., Thapa, P., Boynton, B., Selim, B. J., Sorenson, E. J., et al. (2022). Comparative performance of different respiratory test parameters for detection of early respiratory insufficiency in patients with ALS. Neurology 99, e743–e750. doi: 10.1212/WNL.0000000000200758
PubMed Abstract | CrossRef Full Text | Google Scholar
Lechtzin, N., Scott, Y., Busse, A. M., Clawson, L. L., Kimball, R., and Wiener, C. M. (2007). Early use of non-invasive ventilation prolongs survival in subjects with ALS. Amyotroph. Lateral Scler. 8, 185–188. doi: 10.1080/17482960701262392
CrossRef Full Text | Google Scholar
Leone, M. A., Mandrioli, J., Russo, S., Cucovici, A., Gianferrari, G., Lisnic, V., et al. (2022). Neutrophils-to-lymphocyte ratio is associated with progression and overall survival in amyotrophic lateral sclerosis. Biomedicine 10:354. doi: 10.3390/biomedicines10020354
PubMed Abstract | CrossRef Full Text | Google Scholar
Manera, U., Torrieri, M. C., Moglia, C., Viglione, M., Daviddi, M. A. R., Matteoni, E., et al. (2020). The role of arterial blood gas analysis (ABG) in amyotrophic lateral sclerosis respiratory monitoring. J. Neurol. Neurosurg. Psychiatry 91, 999–1000. doi: 10.1136/jnnp-2020-323810
PubMed Abstract | CrossRef Full Text | Google Scholar
Melo, J., Homma, A., Iturriaga, E., Frierson, L., Amato, A., Anzueto, A., et al. (1999). Pulmonary evaluation and prevalence of non-invasive ventilation in patients with amyotrophic lateral sclerosis: a multicenter survey and proposal of a pulmonary protocol. J. Neurol. Sci. 169, 114–117. doi: 10.1016/S0022-510X(99)00228-2
PubMed Abstract | CrossRef Full Text | Google Scholar
Michels, S., Widmann, P., Rapp, D., Willkomm, F., Ludolph, A. C., and Dorst, J. (2022). Predictive parameters of early respiratory decline in amyotrophic lateral sclerosis. Eur. J. Neurol. 29, 3170–3176. doi: 10.1111/ENE.15486
PubMed Abstract | CrossRef Full Text | Google Scholar
Murray, D., Rooney, J., Al-Chalabi, A., Bunte, T., Chiwera, T., Choudhury, M., et al. (2021). Correlations between measures of ALS respiratory function: is there an alternative to FVC? Amyotrophic Lateral Scler. Frontotemporal Degener. 22, 495–504. doi: 10.1080/21678421.2021.1908362
PubMed Abstract | CrossRef Full Text | Google Scholar
Naal, T., Abuhalimeh, B., Khirfan, G., Dweik, R. A., Tang, W. H. W., and Tonelli, A. R. (2018). Serum chloride levels track with survival in patients with pulmonary arterial hypertension. Chest 154, 541–549. doi: 10.1016/J.CHEST.2018.04.022
PubMed Abstract | CrossRef Full Text | Google Scholar
Piepers, S., Van Den Berg, J., Kalmijn, S., Van Der Pol, W., Wokke, J. H. J., Lindeman, E., et al. (2006). Effect of non-invasive ventilation on survival, quality of life, respiratory function and cognition: a review of the literature. Amyotroph. Lateral Scler. 7, 195–200. doi: 10.1080/14660820500514974
PubMed Abstract | CrossRef Full Text | Google Scholar
Qureshi, M., Shui, A., Dibernardo, A. B., Brown, R. H., Schoenfeld, D. A., and Cudkowicz, M. E. (2008). Medications and laboratory parameters as prognostic factors in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. 9, 369–374. doi: 10.1080/17482960802163614
PubMed Abstract | CrossRef Full Text | Google Scholar
Stambler, N., Charatan, M., and Cedarbaum, J. M. (1998). Prognostic indicators of survival in ALS. Neurology 50, 66–72. doi: 10.1212/WNL.50.1.66
CrossRef Full Text | Google Scholar
Sun, J., Carrero, J. J., Zagai, U., Evans, M., Ingre, C., Pawitan, Y., et al. (2020). Blood biomarkers and prognosis of amyotrophic lateral sclerosis. Eur. J. Neurol. 27, 2125–2133. doi: 10.1111/ENE.14409
CrossRef Full Text | Google Scholar
Uygur, F., Tanriverdi, H., Aktop, Z., Erboy, F., Altinsoy, B., Damar, M., et al. (2016). The neutrophil-to-lymphocyte ratio in patients with obstructive sleep apnoea syndrome and its relationship with cardiovascular disease. Heart Lung 45, 121–125. doi: 10.1016/j.hrtlng.2016.01.002
PubMed Abstract | CrossRef Full Text | Google Scholar
Westeneng, H.-J., Debray, T. P. A., Visser, A. E., van Eijk, R. P. A., Rooney, J. P. K., Calvo, A., et al. (2018). Prognosis for patients with amyotrophic lateral sclerosis: development and validation of a personalised prediction model. Lancet Neurol. 17, 423–433. doi: 10.1016/S1474-4422(18)30089-9
留言 (0)