
記住我
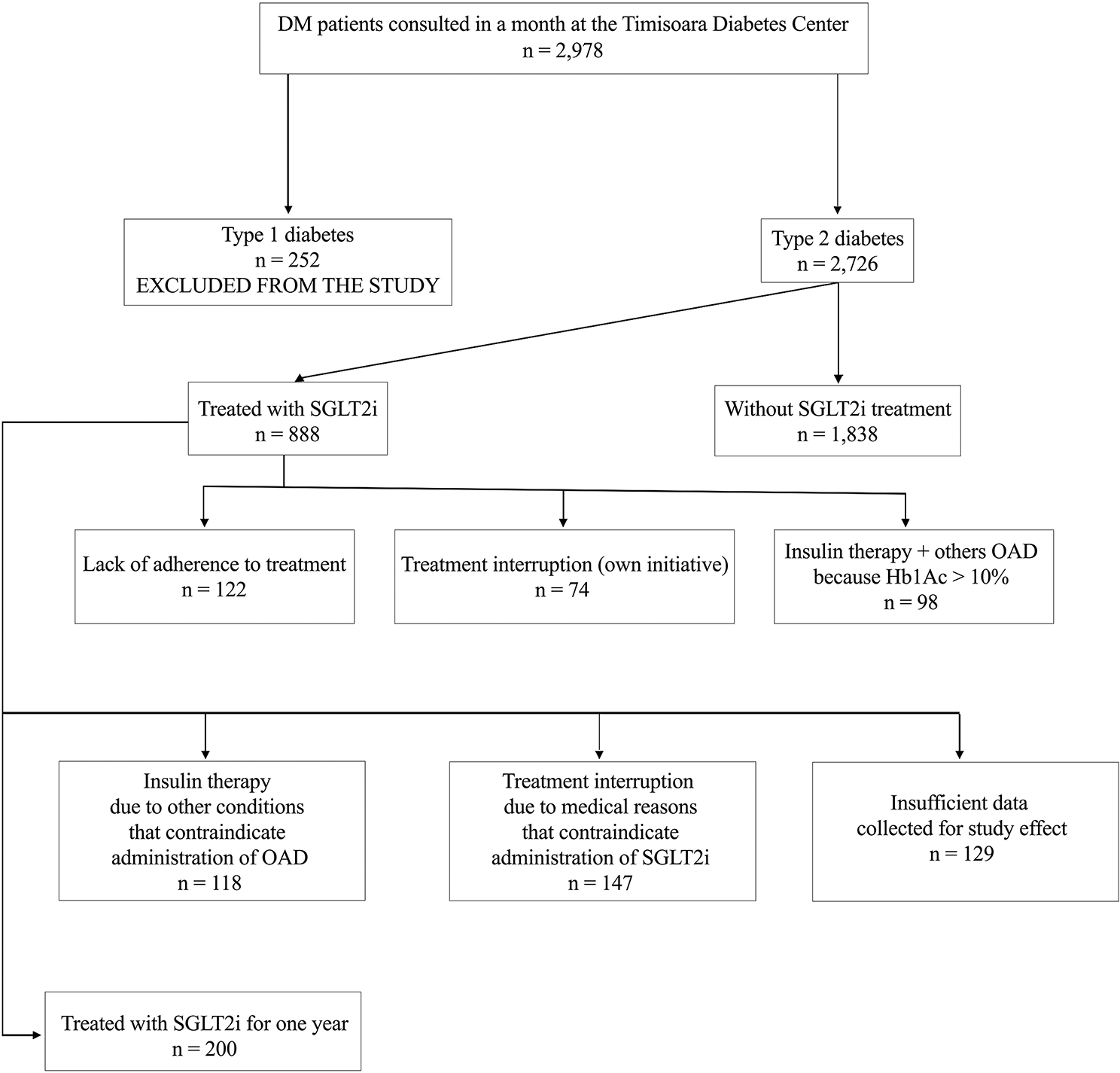
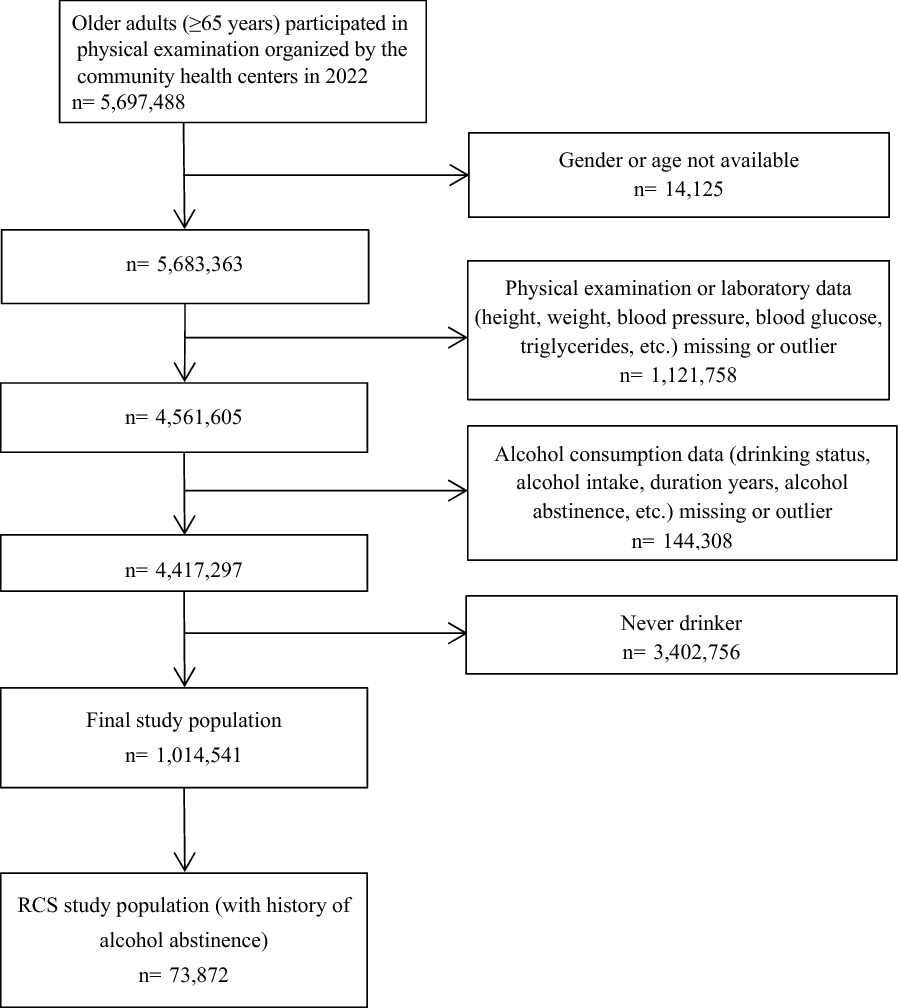
For our study, six cycles of continuous NHANES 2007–2018 data were employed, with 10,487 participants diagnosed Mets included. Individuals aged < 20 years and without complete data of diet, physical activity, PHQ9 and mortality were excluded, resulting in 8301 subjects included in our analysis. Figure 1 illustrates the process of participant inclusion.
Fig. 1
Flowchart of NHANES participants with Mets enrolled in this study
Participants in the National Health and Nutrition Examination Survey (NHANES) with Mets (N = 8301) from 2007 to 2018 were examined. Up to the end of 2019, their unique vital status was connected to the National Death Index. After a median follow-up of 6.3 years, 1080 out of the 8301(about 13.0%) individuals with MetS died. They were categorized into below median (aMED scores 0–3), median (aMED scores 4), and above median (aMED scores 5–9) groups based on their aMED scores. Table 1 suggested participants in the above median aMED (scores 5–9) appeared to be older, had a considerably smaller waist circumference, and have higher HDL levels. These participants in the aMED (scores 5–9) had diets higher in MUFA/SFA, lower in meat and higher in vegetables, fruits, whole grains, legumes, nuts and seafood. This group had a lower percentage of depressive symptoms and a higher percentage of recreational activities. According to another diagnostic criterion of MetS, we finally enrolled 9302 MetS participants from 2007 to 2018 in NHANES. After a median follow-up of 6.2 years, 1274 out of the 9302(about 13.7%) individuals with MetS died. They were also categorized into 3 groups. There are 4084, 2118 and 3100 MetS participants in Below median (aMED scores 0–3) group, median (aMED scores 4) and above median (aMED scores 5–9) groups, respectively.
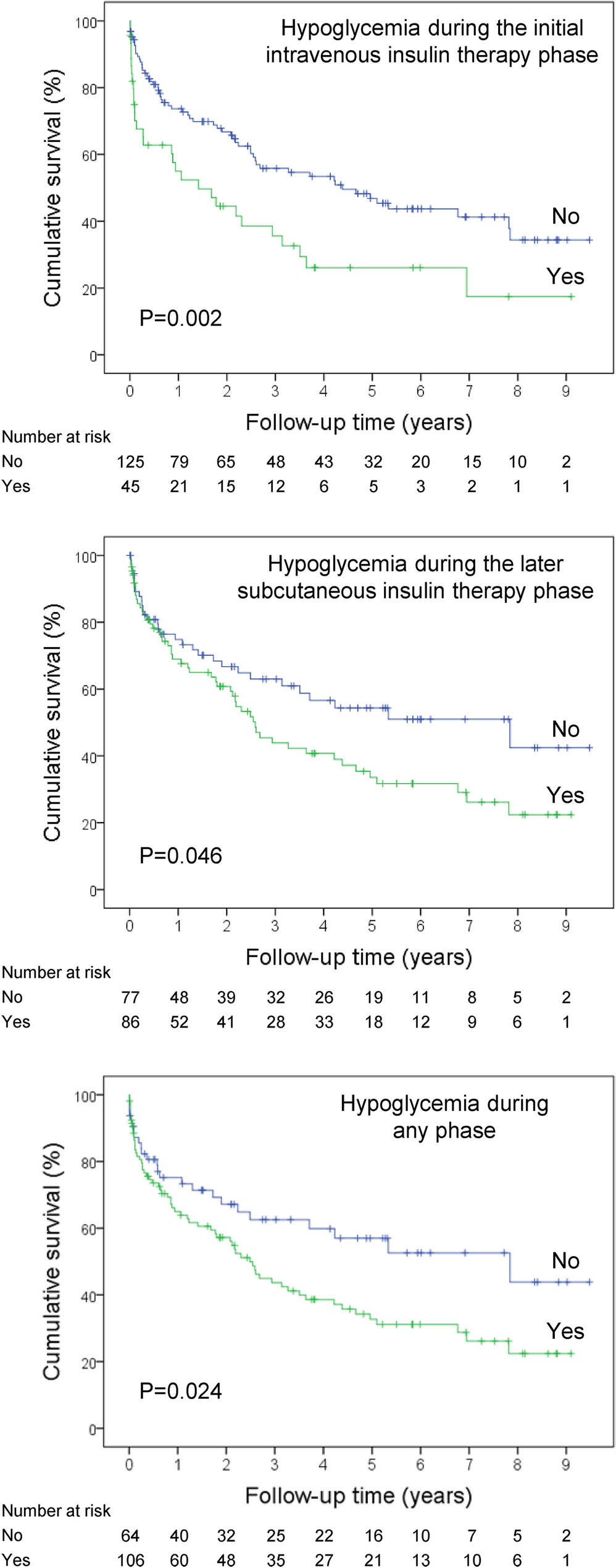
Table 1 Baseline demographics of NHANES participants with MetS in different Mediterranean diet score groups Cox regression analysis of factors associated with all-cause and cardiovascular mortality in MetS participantsTo explore independent predictors strongly associated with all-cause mortality and cardiovascular mortality of MetS participants, the cox regression analysis was performed. The cox regression analysis showed that alternative Mediterranean diet score (Median and Above Median), physical activity, work activity, recreation activity, treatment for hypertension and treatment for diabetes were significantly associated with a lower HR for all-cause mortality while depression, sedentary behavior, smoking, cardiovascular disease were significantly associated with a higher HR for all-cause mortality after adjustment for age, sex, race, education, marital status and poverty to income ratio. The cox regression analysis also showed that alternative Mediterranean diet score (Median and Above Median), recreation activity and treatment for diabetes were significantly associated with a lower HR for cardiovascular mortality whereas sedentary behavior and cardiovascular disease were significantly associated with a higher HR for cardiovascular mortality after adjustment for age, sex, race, education, marital status and poverty to income ratio. These results are presented in Table 2. Figure 2 shows the survival curves of different dietary classes with all-cause death and cardiovascular death after adjustment for age, sex, race, education, marital status and poverty to income ratio, cardiovascular disease and smoking, respectively.
Fig. 2
Survival curves of different dietary classes with all-cause mortality and cardiovascular mortality, respectively. aMED: alternative Mediterranean diet score, LaMED: below median alternative Mediterranean diet score, MaMED: median alternative Mediterranean diet score, HaMED: above median alternative Mediterranean diet score. Model was adjusted for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease and smoking
Table 2 Factors associated with all-cause and cardiovascular mortality in MetS participants Cox regression analysis of participants with MetS for all-cause and cardiovascular mortality in different dietary classes with and without sedentary behaviorTo investigate the joint effect of the Mediterranean diet and sedentary behavior on all-cause mortality and cardiovascular mortality in participants with MetS, we divided all paticipants with MetS into the following six groups: HaMED-non S (MetS participants with above median aMED without sedentary behavior), MaMED-non S (MetS participants with median aMED without sedentary behavior), LaMED-non S (MetS participants with below median aMED without sedentary behavior), HaMED-S (MetS participants with above median aMED with sedentary behavior), MaMED-S (MetS participants with median aMED with sedentary behavior) and LaMED-S (MetS participants with below median aMED with sedentary behavior). Cox regression analysis of the all-cause mortality risk for MaMED-non S, LaMED-non S, HaMED-S, MaMED-S, LaMED-S groups using HaMED-non S group as the control group showed that, after the adjustment for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease, smoking, treatment for hypertension, treatment for diabetes and treatment for cholesterol, there was no significant difference in HR between HaMED-non S, MaMED-non S and LaMED-non S groups. HaMED-S and MaMED-S groups showed a similar increased HR in all-cause mortality (HR, 1.55; 95% CI, 1.15–2.09; P = 0.00), (HR, 1.38; 95% CI, 1.00–1.93; P = 0.05) compared to HaMED-non S group. While LaMED-S group showed the biggest risk in all-cause mortality (HR, 2.45; 95% CI, 1.90–3.17; P = 0.00), which suggested high-quality Mediterranean diet might attenuate the risk of all-cause mortality resulting from sedentary behavior. In terms of cox regression analysis of the cardiovascular mortality risk, there was no significant difference in HR between HaMED-non S, MaMED-non S group, LaMED-non S, HaMED-S groups. As for MaMED-S, LaMED-S groups, HR of two groups was progressively increasing and statistically significant. LaMED-S group also shows the biggest risk in cardiovascular mortality (HR, 2.91; 95% CI, 1.77–4.79; P = 0.00). In MetS participants with sedentary behavior, participants with HaMED shows no difference in HR compared to HaMED-non S group while participants with MaMED or LaMED showed increased HR in cardiovascular mortality, which suggested high-quality Mediterranean diet could completely offset the adverse effects of sedentary behavior to cardiovascular mortality (Table 3). Figure 3 visualizes the results of the cox regression analysis. To further verify the reliability of our conclusions, MetS population under another version of definition was used to perform the above statistical analysis (Appendix 1). Surprisingly, the similar conclusions were also drawn. The only difference is that in MetS participants without sedentary behavior, LaMED is an independent risk factor for all-cause mortality (HR, 1.27; 95% CI, 1.00–1.60; P = 0.05), which also demonstrated high-quality Mediterranean diet could reduce all-cause mortality in MetS participants without sedentary behavior.
Table 3 Cox regression analysis of participants with MetS for all-Cause and cardiovascular mortality according to aMED and sedentary behavior Fig. 3
Forest plot of cox regression analysis of participants with MetS for all-cause and cardiovascular mortality according to aMED and sedentary behavior
HaMED-non S, High aMED without sedentary behavior; MaMED-non S, Medium aMED without sedentary behavior; LaMED-non S, Low aMED without sedentary behavior; HaMED-S, High aMED with sedentary behavior; MaMED-S, Medium aMED with sedentary behavior; LaMED-S, Low aMED with sedentary behavior. Model was adjusted for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease, smoking, treatment for hypertension, treatment for diabetes and treatment for cholesterol.
Cox regression analysis of participants with MetS all-cause and cardiovascular mortality in different dietary classes with and without depressionTo investigate the joint effect of the Mediterranean diet and depression on all-cause mortality and cardiovascular mortality in participants with MetS, we divided all paticipants with MetS into the following six groups: HaMED-non D (MetS participants with above median aMED without depression), MaMED-non D (MetS participants with median aMED without depression), LaMED-non D (MetS participants with below median aMED without depression), HaMED-D (MetS participants with above median aMED with depression), MaMED-D (MetS participants with median aMED with depression) and LaMED-D (MetS participants with below median aMED with depression). Cox regression analysis of the all-cause mortality risk for MaMED-non D, LaMED-non D, HaMED-D, MaMED-D, LaMED-D groups using HaMED-non D group as the control group showed that, after the adjustment for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease, smoking, treatment for hypertension, treatment for diabetes and treatment for cholesterol, there was no significant difference in HR between HaMED-non D group and MaMED-non D group. However, LaMED-non D group showed a increased HR in all-cause mortality (HR, 1.27; 95% CI, 1.04–1.55; P = 0.02) compared to HaMED-non D group, which means in participants with MetS without depression, lower-quality Mediterranean diet significantly increases all-cause mortality. Similar results can still be observed in participants with MetS with depression. LaMED-D group had the highest all-cause mortality (HR, 1.97; 95% CI, 1.45–1.269; P = 0.00). Interestingly, even when MetS participants combined with depression, but with a higher quality Mediterranean diet, all-cause mortality was not significantly increased and was even lower than those without depression but with a lower quality Mediterranean diet. A similar trend can be observed in cardiovascular mortality. Compared to HaMED-non D group, MaMED-non D, HaMED-D and MaMED-D groups did not show significant difference in HR in cardiovascular mortality. Combined low-quality Mediterranean diet shows higher cardiovascular mortality, regardless of depression, in participants with MetS. LaMED-non D group shows the notable risk in cardiovascular mortality (HR, 1.50; 95% CI, 1.02–2.23; P = 0.04) while LaMED-D group shows the biggest risk in cardiovascular mortality (HR, 1.99; 95% CI, 1.09–3.65; P = 0.03) (Table 4). Figure 4 visualizes the results of the cox regression analysis. To further enhance the robustness of the conclusions, we did the same statistical analysis described above in MetS participants defined by another diagnostic criteria. Similar results are presented in Appendix 2, which again confirms the reliability of the conclusions.
Table 4 Cox regression analysis of participants with MetS for all-cause and cardiovascular mortality according to aMED and depressionHaMED-non D, High aMED without depression; MaMED-non D, Medium aMED without depression; LaMED-non D, Low aMED without depression; HaMED-D, High aMED with depression; MaMED-D, Medium aMED with depression; LaMED-D, Low aMED with depression. Model I was adjusted for age, sex, race, education, marital status and poverty to income ratio; Model II was adjusted for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease and smoking; Model III was adjusted for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease, smoking, treatment for hypertension, treatment for diabetes and treatment for cholesterol.
Fig. 4
Forest plot of cox regression analysis of participants with MetS for all-cause and cardiovascular mortality according to aMED and depression
HaMED-non D, High aMED without depression; MaMED-non D, Medium aMED without depression; LaMED-non D, Low aMED without depression; HaMED-D, High aMED with depression; MaMED-D, Medium aMED with depression; LaMED-D, Low aMED with depression. Model was adjusted for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease, smoking, treatment for hypertension, treatment for diabetes and treatment for cholesterol.
Associations of individual food components of the Mediterranean diet with all-cause and cardiovascular in NHANES participants with MetSTo examine in depth the association between Mediterranean diet components and all-cause mortality and cardiovascular mortality in MetS participants, cox regression analysis was utilized. Among the components of the MED diet, greater vegetables, legumes, nuts intake and high MUFA/SFA ratio were significantly associated with lower all-cause mortality after adjustment for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease, smoking, treatment for hypertension, treatment for diabetes and treatment for cholesterol in participants with MetS (Table 5). Greater vegetables intake was significantly associated with lower cardiovascular mortality after adjustment for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease, smoking, treatment for hypertension, treatment for diabetes and treatment for cholesterol in participants with MetS while more red/processed meat intake was significantly associated with higher cardiovascular mortality. Similar results were also shown for another diagnostic criterion of MetS (Appendix 3). One difference is that under this version of the criteria, greater vegetable intake does not significantly reduce cardiovascular mortality in participants with MetS.
Table 5 Associations between Mediterranean diet components and all-cause and cardiovascular mortality in participants with MetSModel was adjusted for age, sex, race, education, marital status, poverty to income ratio, cardiovascular disease, smoking, treatment for hypertension, treatment for diabetes and treatment for cholesterol.
留言 (0)