The anterior anatomical and surgical approach to the vertebral vessels is of interest for clinical and surgical teaching to undergraduate students, graduates, and surgical residents devoted to the craniocervical region; for medico-legal experts and practitioners of forensic clinical anatomy; and for scientific research [14, 18].
In the forensic field, there are many areas of application, generally aimed at the analysis of injury mechanisms, such as traumatic vertebral artery injuries due to penetrating (i.e., firearm or stab wound related) or nonpenetrating trauma (i.e., blunt force, hyperextension and rotation of the neck) [17, 25,26,27]. Several studies emphasize the clinical relevance of the vertebral artery and the opportunity to routinely examine it in all cases of fatal traumatic head and neck injuries [26, 28,29,30]. This is true for adults and even more so for infants and young children. For this latter, the neck is supported by a weaker musculoskeletal system and is therefore exposed to whiplash injury for sudden extension-and-flexion movement, as reported in shaken baby syndrome [31].
In adults, traumatic vertebral artery injury may be due to motor vehicle accidents, related to seat belt injury or assault with/without intent to kill [32,33,34]. In those settings, a subarachnoid hemorrhage could result from the trauma, or a misdiagnosed delayed laceration/dissection of the vertebral artery could lead to death, which can, in turn, raise issues of medical malpractice [35]. The precipitating event could be a minor trauma such as hyperextension or sudden rotation, causing a lesion of the vertebral artery [36]. This sometimes occurs during surgical and anesthesia procedures or chiropractic manipulation, raising hypotheses of medical malpractice [37,38,39]. The trauma could occur during sports participation, such as rugby, ice hockey, martial arts, golf, and running. It is due to specific mechanical stresses on the vertebral artery, which could be potentially fatal to the sportsman [40].
However, its examination is often neglected because of the difficulty of accessing by dissection procedure to the vertebral arteries, and no workarounds are available [30, 41]. Indeed, there are no specialist tools for cutting of anterior lamina of the transverse process of the cervical vertebrae. Instead, several devices have been adapted for the purpose, with consequences for efficacy, precision, and accuracy of dissection. Other instruments are used to section and remove bone parts of the spine at many levels but are not explicitly aimed at the anterior laminae of the transverse processes of the cervical vertebrae [30]. The use of generic instruments has been noted, such as electric oscillating saws with circumferential or fan blades, surgical scissors (e.g., Metzenbaum, Mayo), forceps, and ossivorous pliers [42, 43], or even rachiotomes by which the spinal cord can be isolated with bloody, rough, and poorly controllable management [9, 44]. These premises necessarily lead to a high probability of iatrogenic injury to vertebral vessels during anatomical dissection for clinical, surgical, medico-legal, or research purposes [20,21,22]. This, in turn, involves a challenging interpretation of the pathophysiological nature of what has been documented, taking into account anatomical variants [45], pathological entities [46, 47], the consequences of trauma, or a technical error during dissection [48]. The educational, experimental, and cognitive value can be prejudiced and the morphological datum altered [19].
Consequently, a novel dissection tool called the transversoclasiotome was devised and evaluated using anatomical dissections. The composite name “transversoclasiotome” is derived from the Greek -τόμον or -τέμνω, for “cutting,” and -κλᾰ́σῐς, for “rupture,” as the foramen transversarium is opened through cutting and rupture of its anterior lamina. The instrument has been proven suitable for its purpose, comfortable in positioning and maneuvering, and responding adequately to the pressure exerted and resistance felt against the bone lamina. The ergonomic character of the tool was evident, with the operator experiencing no fatigue standing next to the supine-positioned cadaver. The instrument was designed for right-handers and used from the cadaver’s right side, but it can be used on the left side of the neck or applied downward while standing on the left side of the body. The cutting energy could be transferred gradually during the execution of the task. The bone section was cleanly cut and easy to obtain, partially because of the thickness of the anterior lamina of the transverse process (1 mm). The tool did not slide off as it was closed on the bone lamina, acting like a “guillotine” with a wedge effect during the sectioning. As designed, the cutting jaws did not protrude beyond the external/lower profile of the knocker. Hence, the vertebral vessels were not injured during instrument insertion or cutting.
For describing the course of the vertebral artery detected during the anatomical dissections, reference will be made to the individual segments from V1 to V3, omitting segment V4, which is beyond the scope of the present study [49].
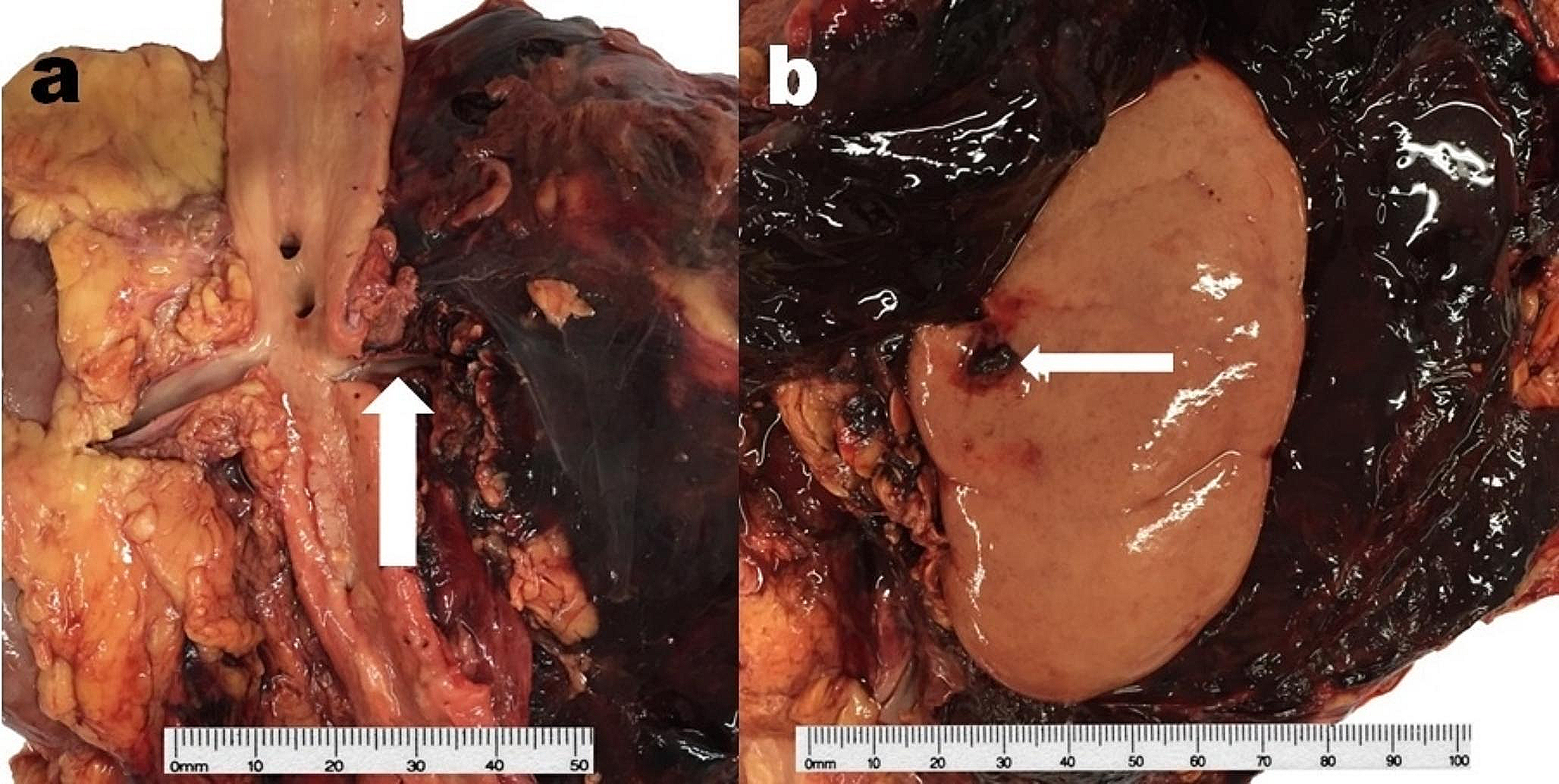
The first part (V1—ostial or preforaminal segment) originates at the posterior surface of the ipsilateral subclavian artery, passes anteriorly to the transverse process of C7, and enters the foramen transversarium of the C6 vertebra [50]. This tract is located, together with the vertebral vein positioned ahead of it, in the triangle of the vertebral artery, delimited by the lateral edge of the longus colli muscle, the medial edge of the anterior scalene muscle, and the first part of the subclavian artery [51]. It is located behind the internal jugular vein, here removed for convenience.
The second part (V2—foraminal segment) rises through the foramina transversaria of the cervical vertebrae from C6 to C1, passing from one foramen transversarium to the next and crossing the roots of the cervical plexus in the intertransverse tract anteriorly. The transverse processes from C4 to C6 are located at the same depth in the neck. The C7 transverse process is posterior owing to the cervical lordosis. Consequently, the vertebral artery passes anteriorly at a significant distance from C7 but reaches the transverse process of C6 with no substantial change of direction [52]. The C2 transverse process is inclined downwards with an oblique lateral and inferior orientation, unlike all the other cervical vertebrae, in which it is horizontal and perpendicular to the vertebral body. This implies that the foramen transversarium has an almost sagittal arrangement, so the vertebral artery has to move laterally to reach the C2 transverse process from C3. This is also because the C2 transverse process is longer than the others below it [52]. The anteroposterior diameter of the foramen transversarium decreases from C6 to C3, while the transverse diameter is minimal at C5 [53]. At the foramina transversaria, the vertebral artery is enclosed in a periosteal sheath that is continuous with the one covering the foramina transversaria, within which the vertebral artery is free to slip very little [52] because, at some points, it adheres to the periosteum, from which it must be detached.
Moreover, at the intertransverse tract, the vertebral artery and the roots of the cervical plexus are enclosed by a fibroligamentous band connected to the lateral part of the uncinate process and the related uncovertebral joint, thus forming a single entity [48]. Overall, these anatomical features allow the vertebral artery to be stretched or compressed during movements of the neck without being injured, at the same time guaranteeing blood flow. The mean diameters of the vertebral arteries and their distances from the midline were in line with literature data, and no anatomical variations (fenestration, duplication, or hypoplasia) or abnormal courses were noted in the present case series [54,55,56].
The third part (V3—suboccipital or extradural or extraspinal segment) extends from the foramen transversarium of C1 to the site of passage through the dura mater. After exiting the foramen transversarium, the vertebral artery curves posteriorly at almost a right angle and then folds medially to engage in the groove for the vertebral artery behind the superior articular facet of the lateral mass of the atlas. In the present case series, there was a standard-shaped groove for the vertebral artery bilaterally, without anterior and posterior osseous bridges arching over the suboccipital segment (V3), transforming the arterial groove into a semi-canal or a complete canal known as the foramen arcuale [57]. This osseous foramen was reported in up to 22% of the general population, housing the vertebral artery, vertebral venous plexus, and suboccipital nerve [57,58,59,60]. Its incomplete variant, the semi-canal, was described in up to 28% of the population [57, 59, 60]. However, a meta-analysis showed that the overall incidences of the complete and the semi-canal variants were lower, with prevalences of 9.1% (95% CI 8.2–10.1%) and 13.6% (95% CI 11.2–16.2%), respectively, males predominating in first case and females in the second [61]. Once it has passed over the groove, the vertebral artery folds anteriorly to enter the dura mater behind the occipital condyles, finally ascending through the foramen magnum. The V3 segment can be divided into three parts: a vertical portion that rises through the foramen transversarium of C1, a horizontal portion that flows into the groove for the vertebral artery, and an oblique portion that penetrates the dura mater. This convoluted course is attributable to its passage through mobile bone structures, which can move without injuring the vessel during neck rotation [62].
The fourth part (V4—intradural or intracranial segment) penetrates the dura mater just below the lateral edge of the foramen magnum, creating an invagination of the dura and the periosteal sheath up to 4 mm, with a double coverage enveloping the vertebral artery. Here, the periosteal sheath forms the distal fibrous ring [52]. The fourth part ends at the vertebrobasilar junction.
Along its route, the vertebral artery emits small branches that can be easily preserved through the transversoclasiotome [63]. The spinal branches pass through the intervertebral foramina to enter the spinal canal and supply the spinal cord, its membranes, the vertebral body, and the periosteum. Muscular branches supply the deep muscles at the C1 level. The posterior spinal artery usually originates from the posteromedial surface of the vertebral artery before perforating the dura mater.
The vertebral vein accompanies the vertebral artery along its path. It appears plexiform, progressively converging to a single vessel before connecting with the brachiocephalic vein after it emerges from the foramen transversarium of the C6 vertebra. Occasionally, two vertebral veins have been described, though not in the case series presented [64].
Overall, the transversoclasiotome has been proven appropriate for sectioning the anterior lamina of the transverse process of the cervical vertebrae. It was easy to handle, reacting promptly to the operator’s movement and action and overcoming the bone lamina’s structural resistance to be cut. The tool grasped the bone safely and stably without sliding off during closing. The vertebral vessels were not injured either during the insertion of the instrument or during the bone cutting.
Its use exposed the vertebral vessels for easy examination of their morphological features and anatomical relationships, as required in clinical anatomy for teaching and training clinicians or surgeons; in forensic clinical anatomy during medico-legal ascertainment; and in research.







留言 (0)