
記住我
A total of 103 patients were included, of whom 32 from AMS, 36 from OXF and 35 from BAR. Conventional treatment was performed in 59 patients, EVASC in 23, EVT in 12, transanal suturing in 6 and redo-anastomosis in 3. More patients had received no neoadjuvant therapy after conventional treatment (61%) and EVT (58%), compared to EVASC (39%) and transanal suturing (33%). The proportion of diverting stoma after primary resection was similar after conventional treatment (59%) and EVASC (48%), but was higher after EVT (75%) and transanal suturing (83%), see also Fig. 1. For all baseline characteristics, see Table 1.
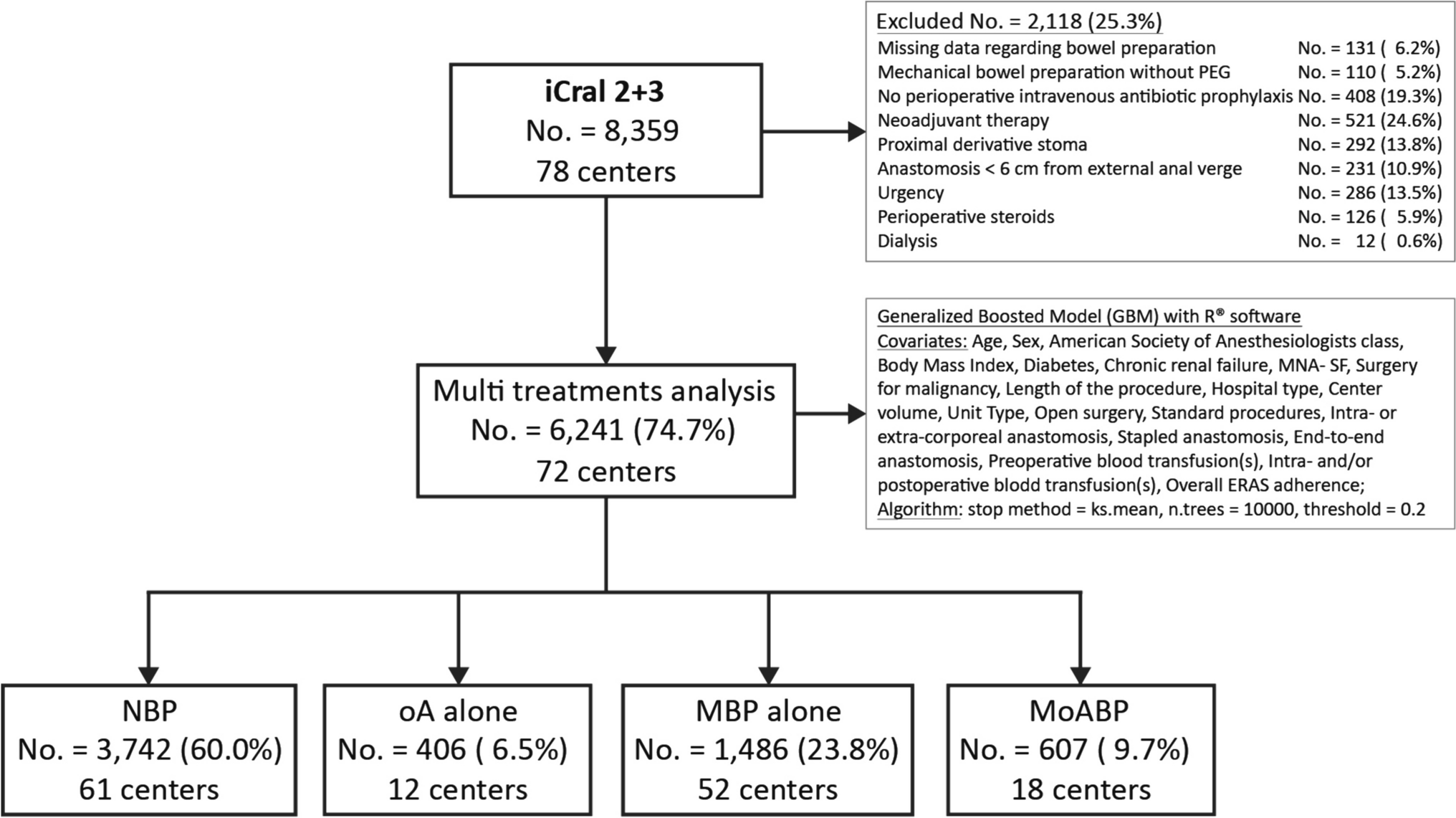
Fig. 1
Flow diagram. AL anastomotic leakage, LAR low anterior resection, EVASC endoscopic vacuum-assisted surgical closure, EVT endoscopic vacuum therapy
Table 1 Baseline characteristicsAL diagnosisTiming of AL diagnosis is displayed in Table 2. AL was diagnosed within 14 days after index operation in 68% in the conventional group, compared to 78% in the EVASC group, 83% in EVT-no closure and 67% in the transanal suturing group. Differences in median interval from LAR to initiation of treatment were similar to time to diagnosis.
Table 2 Timing of leakage diagnosis and subsequent treatment with detailed description of reinterventions and readmissionsReinterventionsReintervention rate excluding stoma creation/closure was only 53% in the conventional group, compared to 100% in the other groups. The median number of reinterventions was highest in the EVT group (8, IQR 4–15), followed by EVASC (7, IQR 5–10), transanal suturing (1.5, IQR 1–4) and conventional treatment (1, IQR 0–1).
Resection of the anastomosis with creation of end-colostomy was performed most often in the EVT group (33%), followed by conventional treatment (24%), transanal suturing (17%) and EVASC (17%).
ReadmissionsReadmission excluding stoma creation/closure was highest in transanal suturing (83%), followed by EVT (75%), EVASC (70%) and conventional treatment (54%). Median number of readmissions was higher in EVT and transanal suturing (2, IQR 0–3 and 2, IQR 1–3), compared to conventional and EVASC (1, IQR 0–1 and 1, IQR 0–3). Reasons for readmission were mainly for treatment of AL. Median total length of stay excluding stoma closure/creation was highest after EVT (52 days, IQR 33–84), followed by EVASC (25 days, IQR 19–34), transanal suturing (18 days, IQR 10–37) and conventional treatment (16 days, IQR 9–28).
Surgical outcomesThe outcomes regarding anastomotic healing and bowel continuity after a median follow-up of 25–39 months are displayed in Table 3. The percentage of healed anastomosis at the end of follow-up was 61% after conventional treatment, 78% after EVASC, 42% after EVT and 83% after transanal suturing.
Table 3 Surgical outcomesMedian interval from LAR to healed anastomosis was shortest after transanal suturing (104 days, IQR 60–252), followed by EVASC (114 days, IQR 48–210), conventional treatment (141 days, IQR 77–216) and EVT (304 days, 197–567).
The highest proportion of patients with a functional anastomosis was found for transanal suturing (83%), followed by EVASC (78%), conventional treatment (54%) and EVT (33%). Median interval from LAR to functional anastomosis was shortest in EVASC (185 days, IQR 146–292), compared to conventional (267 days, IQR 142–368), transanal suturing (296 days, IQR 207–353) and EVT (364 days, IQR 325–676).
Pairwise comparison and subgroup analysisPairwise comparison showed a higher healed anastomosis rate after EVASC compared to conventional treatment (78% vs. 61%), although this was not statistically significant (p = 0.139) (Table 4). The functional anastomosis rate was significantly higher after EVASC, when compared to conventional treatment (78% vs. 54%, p = 0.045). In the EVASC group more surgical reinterventions were performed (median 3 vs. 2, p < 0.001), more readmissions (median 2 vs. 1, p < 0.001) and a longer length of stay (median 30 vs. 19 days, p = 0.004) were seen, compared to conventional treatment. More planned readmissions were seen after EVASC (median 1 vs. 2, p < 0.001), but no difference in unplanned readmissions was seen (median 0 vs. 0, p = 0.479).
Table 4 Pairwise comparison and subgroup analysisIf EVASC was started in the first 7 days after surgery, the healed anastomosis rate was higher (100% vs. 55%, p = 0.008), compared to late initiation (> 7 days). Similarly, the functional anastomosis rate was higher (100% vs. 55%), with similar median number of reinterventions (9 vs. 8, p = 0.880) and length of stay (29 vs. 30 days, p = 0.566), but fewer readmissions (1 vs. 4, p < 0.001).
If mucosal approximation was obtained this led to higher healed anastomosis rate (81% vs. 58%, p = 0.021) and higher functional anastomosis rates (81% vs. 51%, p = 0.003), when compared to passive closure or other treatments. Median numbers of reinterventions (8 vs. 2, p < 0.001) and readmissions (2 vs. 1, p < 0.001) were higher after mucosal approximation, compared to passive closure or other treatments.
留言 (0)