
記住我









We conducted a cross-sectional study in both Nairobi and the Coast region of Kenya. These regions were selected since they have unique socioeconomic characteristics that are representative of the country’s diversity. The regions have predominantly youthful populations [17]. Nairobi, which is the capital city and the economic hub of Kenya, has a diversified population made up of people who have migrated from different parts of the country in quests of better prospects. On the other hand, the Coast region has both urban and rural populations, with a significant Muslim community. We chose the two regions in order to capture some of the heterogeneity in the country.
The study was conducted between February and May 2022. In Nairobi County, this study primarily focused on Dagoretti South, which is one of the county's seventeen sub-counties. The area is peri-urban and it consists of five wards including; Riruta, Waithaka, Ngando, Mutuini, and Uthiru-Ruthimitu.
In the Coast region, this study was conducted in Kilifi and Mombasa Counties. Mombasa County, is a major transportation and tourism hub in the country. The county has over 250,000 people (43.8%) between the ages of 15 and 35 [6]. In Mombasa County, the study was conducted in Jomvu sub-county. The sub-county is characterized with informal settlements, including Bangladesh which is one of the oldest and largest informal settlements in Mombasa. Kilifi County is situated North of Mombasa. It lies on the shores of the Indian Ocean and is a major tourist destination in the country mostly due to its sandy and beautiful beaches. In Kilifi, the study was conducted in Kaloleni sub-county, which is primarily rural offering a unique perspective on the region's social and economic dynamics.
Eligibility criteria, and participants’ recruitmentDuring the recruitment, adolescents and their parents were approached by the study mobilizers in their homes and informed about the study. The mobilizers scheduled appointments for the full consenting and the assessments in advance for the potential participants based on the inclusion criteria.
Adolescents were included in the study if;
1.They were aged 13–19 years as established by their birth certificates.
2.Parents of those aged below 18 years could provide parental consent (or caregiver consent in case the parent is absent) and the adolescents could assent.
3.Those aged at least 18 years had identification cards and could self-consent.
4.If they were currently school-going or had dropped out of schools.
5.Could speak either English or Swahili (the official languages of Kenya).
Sample sizeSample size calculations were based on the formula for comparison of the prevalence of two samples [7, 36]. We considered a 95% confidence interval (CI), a design effect of 2, a precision of 0.05, and a non-response rate of 1%, leading to a target sample of 724 participants. Taking into account missing data, participants not meeting the inclusion criteria or other factors that can reduce the final sample size we aimed to recruit a sample of > 750. This was also considered sufficient to conduct sub-group analysis and detect prevalence differences between the school-going and out-of-school populations.
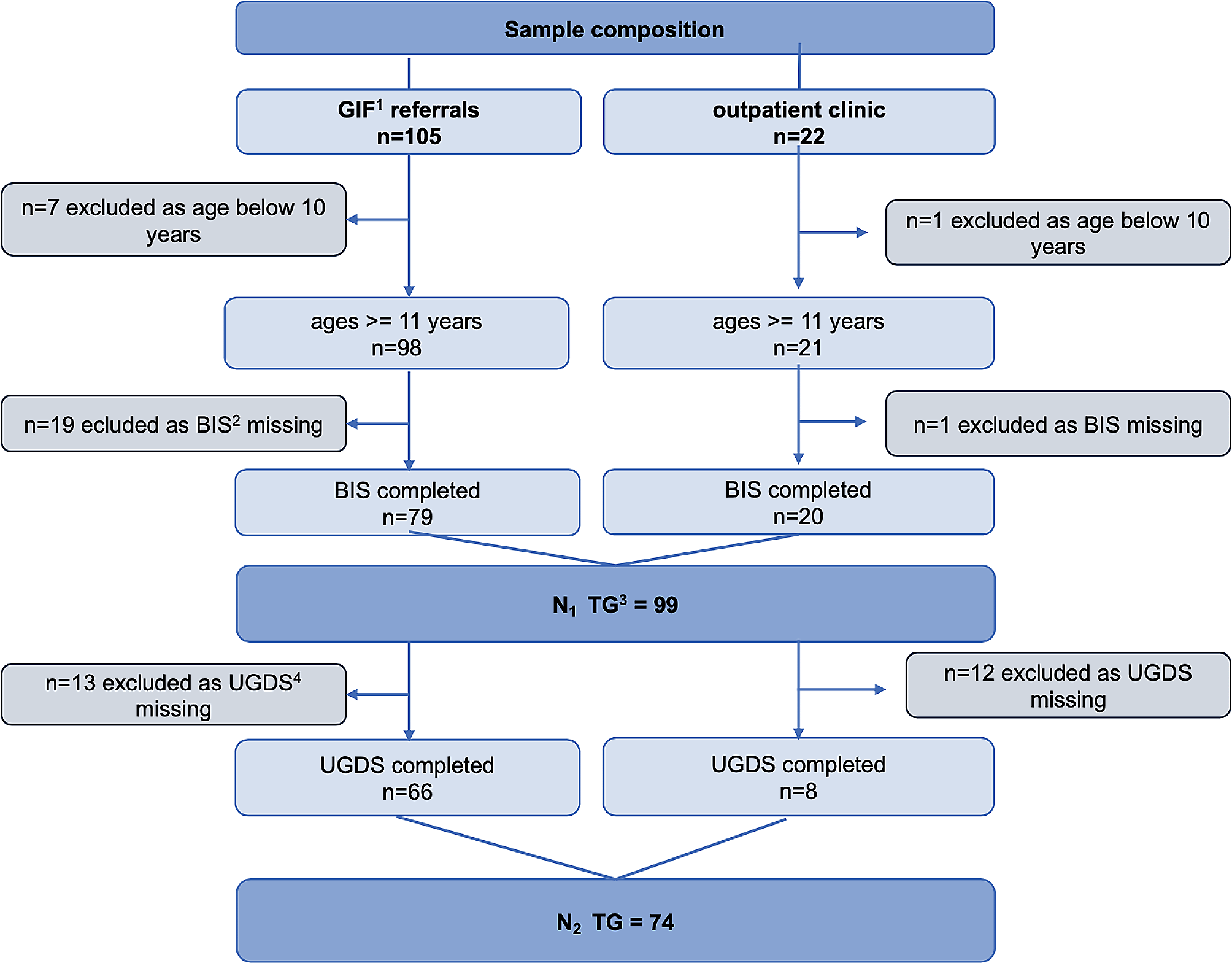
Eight hundred and fifty-two (852) adolescents were approached to participate in the study. Of those, 26 refused to take part in the study. Furthermore, 29 did not meet the full inclusion criteria. Among the participants who completed the baseline survey, 797 were included in the statistical analysis (Fig. 1).
Fig. 1
Participants recruitment flowchart
Data collection proceduresTen research assistants with either diploma or bachelor’s degree qualifications were recruited and trained before conducting the field activities. The authors' GM, RA, AM, MK, and AA facilitated the week-long training in both sites (Nairobi and Coast). Topics covered during the training sessions included: an overview of constructs, a review of tools/questionnaires, psychological first aid, consent, privacy, confidentially and ethics, how to conduct face-to-face interviews, recruitment and mobilization strategy, COVID-19 protocols, and data management. The team spractised how to effectively conduct consent on participants through role plays. Pretesting of the tools used in the quantitative study was done through a pilot study.
For school-going adolescents, we created a list of schools within our study sites and used simple random sampling to select a total of 10 schools (out of a list of all existing schools including primary, and secondary schools, stratified in such a way that schools are geographically spread out). Since the field activities were conducted when schools were closed for holidays, we worked with a School Health Focal Person (SHFP) from the Ministry of Education (MOE), teachers, community health volunteers (CHVs), and community health assistants (CHAs) to recruit students from the communities who met our inclusion criteria and where from the schools selected.
For the out-of-school adolescents, we worked with the Community Focal Person (CFP) from the county government, CHAs, and CHVs to recruit participants who met our inclusion criteria. Out-of-school adolescents were defined as adolescents who were not enrolled in either primary or secondary schools [14]. Adolescents who had completed primary school or secondary school exams in February and March 2022 respectively and were waiting for the government directive to advance to the next level of their education were not considered to be part of the out-of-school population. However, those who had completed primary-level national exams before 2022 and had not progressed to secondary or high school at the time of data collection were deemed out of school. Before the mobilization, all the mobilizers were trained on the study’s mobilization and community engagement strategy and procedures. We drew on the CHVs' and CHAs' knowledge of both the geography and local population of the study sites to identify potential out-of-school adolescents.
During our face-to-face data collection, we ensured all the stipulated COVID-19 guidelines were followed and data collection was carried out in specified sites in each of the counties. Adolescents below eighteen years were accompanied by their parents to ensure they provide consent. The assessments took approximately one hour. After the assessment, a small refreshment was provided to the participants. To ensure that the refreshments offered did not influence participation or responses, we made it clear to all of the participants that the refreshments were being offered as a token of appreciation for their time and effort and that their decision to participate in the study would not be influenced by whether or not they accepted the refreshments. Additionally, refreshments were offered to all mobilized participants, regardless of whether or not they agreed to participate in the study. This ensured that there was no differential treatment of participants based on their willingness to participate. Finally, we used standardized questionnaires and a data collection process, which was administered by trained research assistants who were not involved in the distribution of the refreshments. This minimized the potential for response bias or influence on the data collection process.
Cost incurred such as travel to attend these discussions were reimbursed to the guardians/parents based on standard acceptable rates. Based on various sources of information, we determined a flat rate of transportation rate. This included conducting planning engagements in which we consulted with community leaders to obtain an estimate of the typical cost of transportation in the study area. Secondly, we reviewed previous studies conducted in the area that involved similar participant populations and assessed the transportation costs associated with those studies. The rate agreed upon was also per rates as guided by the Aga Khan University Institute for Human Development participant’s transport payment and reimbursement standard operating procedures. We aimed to ensure that the transportation reimbursement provided was sufficient to cover the cost of transportation to and from the study site, without providing an excessive or undue financial incentive for participation.
MeasuresSocial demographic measureThe information on adolescents' age, gender, school attendance (whether they were in school or not), level of education, religion, economic status, and parental marital status was collected using a socio-demographic survey tool. The household socioeconomic status was evaluated by asking the adolescents about items found in their homes using an assets index that has been used in similar studies focusing on adolescents [1, 39].
Patient health questionnaire- 9 (PHQ-9)PHQ-9 is a multipurpose instrument for screening, diagnosing, and measuring the severity of depression [18]. In this study, PHQ-9 was used to screen for depressive symptoms. The tool consists of 9 items scored on a 4-point Likert scale (0 = not at all, 1 = several days, 2 = more than a week, 3 = nearly every day). The items are summated together, and the total scores range from 0–27. A score of 5–9, 10–14, 15–19, and 20–27 represents the cut-off points for mild, moderate, moderately severe, and severe depression, respectively. PHQ-9 has been used and validated for use in adolescents from Africa [2, 20, 43]. The tool has been validated in the Swahili language [24]. Psychometric analysis performed on the PHQ-9 scale for the current study showed a relatively high internal reliability of the scale (Cronbach’s alpha = 0.83).
General anxiety disorder- 7 (GAD-7)The GAD-7 tool was used to assess anxiety among adolescents. The tool consists of seven items, with responses on a Likert scale ranging from 0 (not at all) to 3 (more than half the days) [38]. The scale's total score ranges from 0 to 21, with cutoffs of 5–9, 10–14, and 15–21 equating to mild, moderate, and severe anxiety symptoms, respectively. GAD-7 has been extensively used [, 3, 30] and has been validated in similar settings while maintaining its unidimensional latent structure with favourable psychometric characteristics [27]. In this study, results from reliability analysis showed that the GAD-7 scale had good internal reliability (Cronbach’s alpha = 0.81).
Strengths and difficulties questionnaire (SDQ)The SDQ is a brief 25-item emotional and behavioural screening tool for children and young people [12]. The SDQ questionnaire contains 25 items, grouped into five subscales (emotional symptoms, conduct issues, hyperactivity/inattention, peer relationship issues, and prosocial behaviour) and the item scores are 0 (not true), 1 (somewhat true), and 2 (certainly true). The scores of all except the prosocial behaviour sub-scale (positive measure) are aggregated to give a total difficulty score ranging from 0 to 40. SDQ has been widely used in Africa to assess internalizing and externalizing problems among children and adolescents, in which as of 2018 it had been used in 54 studies conducted across 12 countries in Africa, including Kenya [13]. A reliability analysis was carried out including 20 items from the SDQ scale. The analysis showed that the scale had acceptable internal reliability (Cronbach’s alpha = 0.75).
Pandemic anxiety scale (PAS)The PAS was used to identify the specific aspects of the COVID-19 pandemic that cause worries. The PAS is a nine-item scale with ratings on a five-point Likert scale of 0 (strongly disagree) to 4 (strongly agree), with scores ranging from 0 to 36. The scale includes questions about the disease itself as well as concerns and worries about the pandemic's consequences and has good validity and reliability [22]. Item 7 (I am worried about missing schoolwork) was not used in the analysis as it was not relevant to the out-of-school population, hence the highest score based on the remaining eight questions was 32. The scale had acceptable internal reliability based on results from psychometric analysis (Cronbach’s alpha = 0.77).
The World Health Organization- five well-being index (WHO-5)The WHO-5 scale was administered to assess the adolescents' quality of life. The tool has five items scored from 0 (at no time) to 5 (all the time), and the total score ranges from 0 to 25 [46]. A total score of 0 illustrates the worst possible quality of life, while a total score of 25 represents the best probable quality of life. The tool has been used in a similar setting, validated in the Swahili language [5], and has shown good construct validity in measuring the quality of life in younger populations [44]. Psychometric analysis of the current study showed that the WHO-5 tool had acceptable internal reliability (Cronbach’s alpha = 0.75).
Covid-19 related questionnaireWe administered the questionnaire to evaluate how the COVID-19 pandemic had affected adolescent mental health care-seeking behaviour, school attendance, peer relationships in the school setting, and interactions with parents.
Assembled items for the Kilifi adolescent health risk behavior questionnaireThe tool was used to assess health risk behaviours among adolescents such as alcohol and drug abuse use, sexual behaviours, and violence among others. The tool is easy to use and has acceptable test–retest reliability (Gwet’s AC1 = 0.82) [40].
Data managementAll data were collected using Open Data Kit (ODK) through tablets and computers. These electronic instruments were password protected and encrypted to avoid data loss and were only available to authorized personnel. To ensure quality control and safety, the data manager double-checked any inconsistencies in the data before uploading it to the server daily.
Statistical analysisStata version 17, a statistical software, was used to analyze all the data [41]. The sample characteristics of the adolescents were summarized using proportions, means, and standard deviations. The differences between the in-school and out-of-school groups were investigated using the independent t-test for continuous variables and Pearson's chi-squared test for categorical variables. For depression and anxiety, the point prevalence and corresponding 95% confidence intervals (95% CI) were calculated. The figures and tables were used to present the results.
A linear regression model was used to evaluate the socio-demographic characteristics, COVID-19-related questions, parents and peer relationships, psychosocial stressors associated with quality of life, pandemic anxiety, and emotional and behavioural problems. First, a univariate linear model was fitted for each outcome, and the variables with a p-value < 0.25 were included in the multivariable linear regression model [4]. Plots and statistical tests were used to evaluate the model assumptions; linearity, normality, multicollinearity, homoscedasticity, and the presence of outlying observations [11].
Subsequently, a logistic regression model was used to assess factors associated with depression and general anxiety disorders. A univariate logistic model was fitted, and variables with a p-value < 0.25 were included in the multivariable logistic regression model. The odds ratios (ORs) with corresponding 95% confidence intervals (CIs) and associated P-values were reported. A 5% significance level was used for this study. Furthermore, in the present study, Cronbach’s coefficient α was used to calculate the internal reliability coefficients of the items used in the regression models. A score of > 0.70 was considered an acceptable value of Cronbach’s alpha based on the reliability analysis [42].
留言 (0)