
記住我





The main goals of surgery for a tibial plateau fracture are to reestablish joint stability, achieve normal limb alignment, and restore the articular surface1,2. Achieving these surgical goals reduces the risk of posttraumatic osteoarthritis and the subsequent need for total knee arthroplasty (TKA)3. However, adequate reduction is not always possible because of comminution and severe fracture displacement. A suboptimal operative result has been reported in up to 30% of surgically treated tibial plateau fractures4. Also, the initial irreversible damage to the articular surface may induce posttraumatic osteoarthritis despite a good operative result5,6. Therefore, pre- and postoperative radiographic assessments of fracture displacement and tibial alignment are important to estimate risks of conversion to TKA at follow-up.
Adequate preoperative assessment of fractures is essential to determine the treatment strategy and counsel patients regarding the prognosis. Initial fracture displacement, which can be assessed by measuring the intra-articular gap and step-off on preoperative computed tomography (CT) scans, is among the decisive factors in the choice between nonoperative and operative management. The results of surgical treatment are usually assessed on postoperative radiographs by measuring the quality of the reduction and tibial alignment. Since these radiographic measurements are important for both treatment decisions and patient counseling about prognosis, it is important to understand their relationship with the clinical outcome. Even though existing research suggests that initial fracture displacement, quality of reduction, and postoperative tibial alignment contribute to the development of posttraumatic osteoarthritis and the need for TKA, the actual impact of these parameters has not yet been clarified3,6,7.
We hypothesized that initial fracture displacement, quality of reduction, and postoperative tibial alignment are predictors of conversion to TKA. The aim of this study was to answer the following research questions: (1) What is the association between the preoperative fracture displacement, in terms of gap and step-off as measured on CT scans, and the risk of conversion to TKA at the time of follow-up? (2) What is the association between the postoperative fracture reduction and knee alignment, as measured on radiographs, and the risk of conversion to TKA at the time of follow-up?
Materials and Methods Study DesignAll patients who underwent tibial plateau fracture surgery between 2003 and 2018 in 4 trauma centers (2 level-1, 2 level-2) were eligible for this retrospective multicenter cross-sectional study if they had a preoperative CT scan, postoperative anteroposterior and lateral radiographs, and follow-up of >1 year. Patients who required amputation, were <18 years old, were deceased, or had an unknown address were excluded. The baseline characteristics of the included patients were retrieved from the electronic patient file. Patients were approached by mail and asked whether they still had their own, native knee (without conversion to TKA) and whether they had undergone any reoperations. If no response was received, a reminder was sent after 3 weeks. Written informed consent was obtained from all patients. The institutional review board of each center approved the study procedures (registry: 201800411), and the research was performed in accordance with the relevant guidelines and regulations. This study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guideline8.
Image ReviewAll images were reassessed by 2 authors (N.A., F.F.A.IJ.) to determine the fracture classification according to the AO/OTA system9. Follow-up radiographs were assessed to verify whether or not patients had undergone conversion to TKA. Measurements were performed in a medical image viewer (Sectra UniView). Radiographs and CT scans were made using standard settings for the x-ray tube or CT scanner. All measurements represented a consensus by the 2 observers (i.e., the observers performed the measurements together).
Preoperative Fracture AssessmentPreoperative CT scans were assessed in the axial, sagittal, and coronal planes. The largest gap and step-off within any of these 3 planes was determined and reported (Fig. 1).
 Fig. 1:
Fig. 1: Gap and step-off measurements performed on separate coronal slices. Upper right: step-off measurement, defined as the separation of fracture fragments perpendicular to the articular surface. Lower right: gap measurement, defined as the separation of fracture fragments along the articular surface.
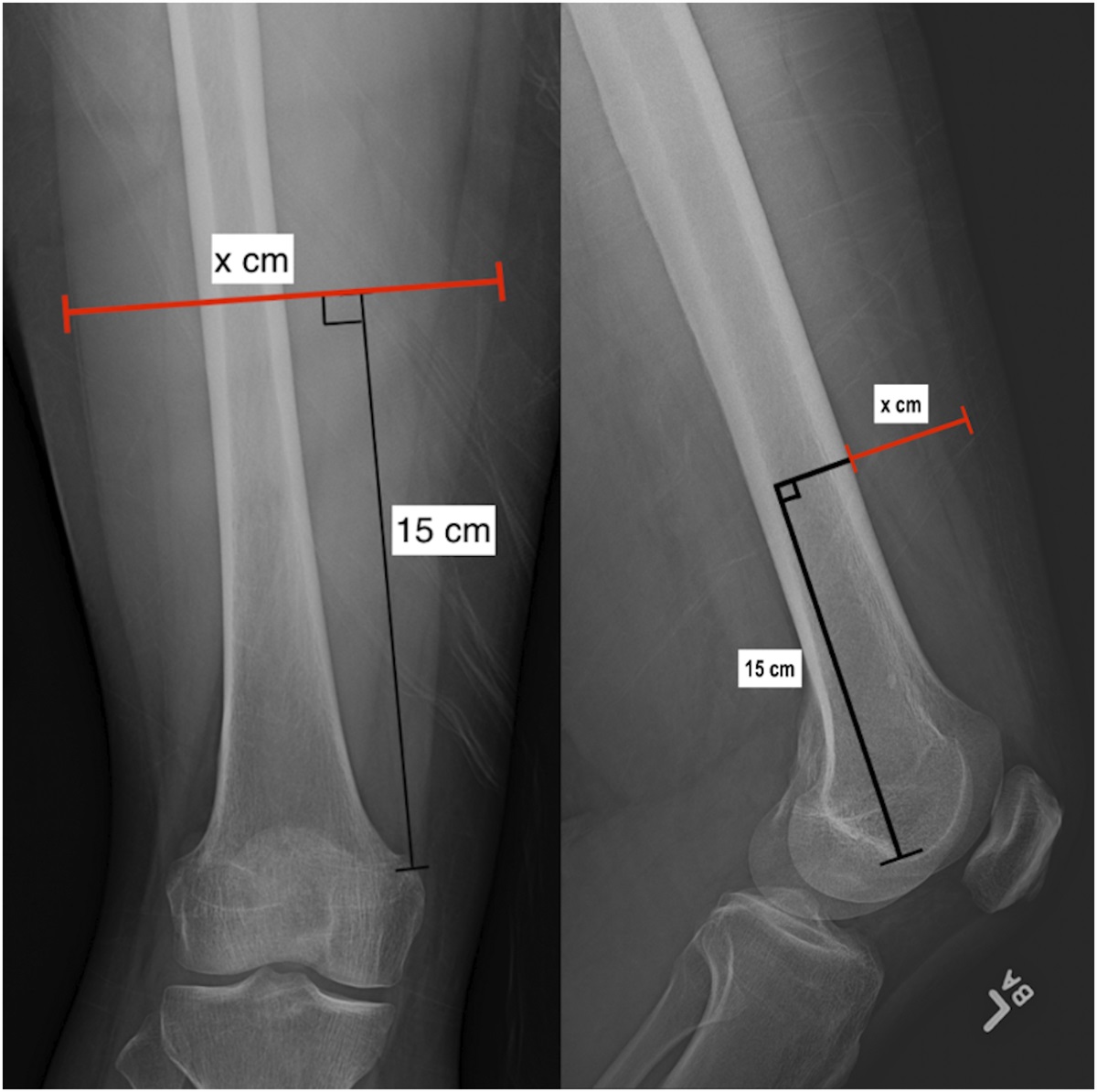
Postoperative Fracture AssessmentThe quality of the fracture reduction and tibial alignment was evaluated on radiographs made ≤2 weeks postoperatively, using 4 radiographic parameters: articular fracture reduction, coronal alignment, sagittal alignment, and condylar widening. Fracture reduction was assessed by measuring the residual intra-articular incongruity (maximum gap and step-off). Coronal alignment was assessed by measuring the medial proximal tibial angle (MPTA) on the anteroposterior radiograph, and sagittal alignment was assessed by measuring the posterior proximal tibial angle (PPTA) on the lateral radiograph (Fig. 2). Condylar widening was assessed as described by Johannsen et al. (Fig. 3)10. Measurements were considered adequate if they were within the normal range. The articular reduction was considered adequate when both the gap and step-off were <2 mm; coronal alignment, when the MPTA was 87° ± 5°; sagittal alignment, when the PPTA was 9° ± 5°; and condylar widening, when it was between 0 and 5 mm11–13.
 Fig. 2:
Fig. 2: Proximal tibial alignment measurements. Fig. 2-A Coronal alignment, or medial proximal tibial angle (MPTA; normal range, 82° to 92°). Fig. 2-B Sagittal alignment, or posterior proximal tibial angle (PPTA; normal range, 4° to 14°).
 Fig. 3:
Fig. 3: Condylar widening measurement. Lateral condylar widening (normal range, 0 to 5 mm) is measured by drawing 2 lines perpendicular to the medial tibial articular surface, one along the most lateral aspect of the distal femoral condyle and the other along the most lateral aspect of the proximal tibia. The measured distance between these lines is considered condylar widening.
Statistical AnalysisMann-Whitney U and chi-square tests were performed to assess differences in baseline characteristics between responders and nonresponders. Critical cutoffs for the preoperative gap and step-off were determined by identifying the point that maximized sensitivity and specificity after plotting a receiver operating characteristic (ROC) curve. For each of the 6 measurements of interest, patients were stratified into groups on the basis of the identified cutoff value or normal range, and Kaplan-Meier curves were plotted for the groups. Log-rank tests were performed to assess differences between these groups. The proportionality assumption was assessed by inspecting log-minus-log plots and by adding an interaction term with time. Cox regression was performed to identify the adjusted hazard ratio (HR, representing the relative risk of a complication based on comparison of the event rates) for conversion to TKA that was associated with each measurement after correction for potential confounders (age, sex, smoking, body mass index [BMI], and AO/OTA classification)14–16. The intraobserver variability of each measurement was determined by repeating the measurements for 20 cases (with a >1-month interval) and calculating the intraclass correlation coefficient (ICC). We used a 2-way mixed, single-measurement model with absolute agreement. Statistical analysis was performed using SPSS (version 23; IBM). A p value of <0.05 was considered significant.
Source of FundingThere was no external funding source for this study.
Results Patient CharacteristicsBetween 2003 and 2018, 1,035 patients were treated surgically for a tibial plateau fracture. Of these, 5 had an amputation, 45 were <18 years old, 97 were deceased at the time of follow-up, and 18 had an unknown address. Eight additional patients were excluded because of insufficient quality of the postoperative radiographs, leaving 862 patients eligible for follow-up. All of these patients were approached, and 477 responded (55% response rate). Table I displays patient demographics. Sixty-seven (14%) of the patients had conversion to TKA and none had conversion to unicompartmental knee arthroplasty. Comparison of the responders with the nonresponders demonstrated small differences in age (mean and standard deviation, 53 ± 14 versus 50 ± 16 years, respectively, p = 0.011) and in the proportion of women (68% versus 61%, p = 0.038).
TABLE I - Patient Characteristics (N = 477) Age*(yr) 53 ± 14 Female 326 (68%) BMI*(kg/m 2 ) 26.1 ± 5 Smoking 113 (24%) AO/OTA classification 41-B1 27 (6%) 41-B2 75 (16%) 41-B3 260 (55%) 41-C1 24 (5%) 41-C2 9 (2%) 41-C3 82 (17%) Operative treatment Plate osteosynthesis 393 (82%) Screw osteosynthesis 84 (18%) Conversion to knee arthroplasty 67 (14%) Unicompartmental knee arthroplasty 0 (0%) Total knee arthroplasty 67 (14%) Follow-up*(yr) 6.5 ± 4.1 Reinterventions during follow-up Elective removal of osteosynthesis material 186 (39%) Reoperation for fracture-related infection 15 (3%) Revision surgery for residual displacement 8 (2%) Reoperation for meniscal or ligamentous repair 7 (2%)*The values are given as the mean ± standard deviation.
Patients who underwent conversion to TKA had a significantly wider preoperative gap (10.1 ± 6.5 versus 6.6 ± 5.9 mm, p < 0.001) and greater step-off (10.6 ± 7.3 versus 7.5 ± 6.1 mm, p < 0.001) compared with those without conversion to TKA. The intraobserver comparison showed an ICC of 0.79 for the gap and 0.78 for step-off. The area under the ROC curve was 0.68 for the preoperative gap and 0.67 for step-off (Fig. 4). The critical cutoff values derived from the ROC analysis were 8.5 mm for the preoperative gap and 6 mm for the step-off.
 Fig. 4:
Fig. 4: Receiver operating characteristic (ROC) curve demonstrating the association of preoperative fracture gap (CTGAP, blue) and step-off (CTSTEP, green) with conversion to total knee arthroplasty.
Postoperative Fracture AssessmentThe group with conversion to TKA had significantly higher percentages of patients with inadequate condylar widening (25% versus 13%, p = 0.008), inadequate articular congruity (64% versus 44%, p = 0.002), coronal malalignment (46% versus 22%, p < 0.001), and sagittal malalignment (64% versus 21%, p < 0.001) compared with patients who did not undergo conversion to TKA and still had their own, native knee (Table II). The intraobserver comparison showed an ICC of 0.8 for condylar widening, 0.8 for articular incongruity, 0.7 for MPTA, and 0.8 for PPTA.
TABLE II - Pre- and Postoperative Measurements for Patients with and without Conversion to TKA Measurement Conversion to TKA P Value* Yes (N = 67) No (N = 410) Preoperative Gap > 8.5 mm 36 (54%) 99 (24%) <0.001 Step-off > 6.0 mm 49 (73%) 185 (45%) <0.001 Postoperative Condylar widening > 5 mm 17 (25%) 53 (13%) 0.008 Articular incongruity > 2 mm 43 (64%) 179 (44%) 0.002 MPTA < 82° or > 92° 31 (46%) 90 (22%) <0.001 PPTA < 4° or > 14° 43 (64%) 87 (21%) <0.001*All p values were significant.
Kaplan-Meier survival curves showed an overall survival rate of 84% for the native knee (free of conversion to TKA) at 10-year follow-up. When stratified on the basis of the critical cutoff value for the preoperative gap, the 10-year knee survival was 91% in the group with a preoperative gap of ≤8.5 mm versus 67% in the group with a gap of >8.5 mm (Fig. 5). When stratified on the basis of a preoperative step-off of ≤6 versus >6 mm, the survival rates were 93% and 75%, respectively. When stratified on the basis of tibial alignment, 10-year survival was 88% in patients with adequate coronal alignment versus 72% in patients with malalignment. When stratified on the basis of adequate versus inadequate sagittal alignment, 10-year survival was 92% versus 63%, respectively. The log-rank test showed that the difference between the survival curves was significant for each measurement (p ≤ 0.011).
 Fig. 5:
Fig. 5: Kaplan-Meier survival curves comparing groups stratified on the basis of preoperative gap (log-rank p < 0.001) (Fig. 5-A) and step-off (log-rank p < 0.001) (Fig. 5-B), condylar widening (log-rank p = 0.011) (Fig. 5-C), postoperative articular incongruity (log-rank p = 0.002) (Fig. 5-D), coronal alignment (log-rank p < 0.001) (Fig. 5-E), and sagittal alignment (log-rank p < 0.001) (Fig. 5-F).
Independent Risk Factors for Conversion to TKAAn HR of 3.3 (95% confidence interval [CI] = 2.0 to 5.4, p < 0.001) was found for patients with a preoperative gap of >8.5 mm, meaning that the instantaneous rate of receiving a TKA at any time during follow-up was 3.3 times higher among patients with a gap of >8.5 mm compared with those with a gap of ≤8.5 mm. Patients with a step-off of >6.0 mm showed an HR of 3.6 (95% CI = 2.0 to 6.3, p < 0.001). Similar results were found after adjusting for confounders (Table III).
TABLE III - Multivariate Analysis of the Association of Radiographic Characteristics with Conversion to TKA Measurement Unadjusted HR (95% CI) P Value Adjusted HR* (95% CI) P Value Preoperative Gap > 8.5 mm 3.3 (2.0-5.4) <0.001† 2.6 (1.5-4.5) <0.001† Step-off > 6.0 mm 3.6 (2.0-6.3) <0.001† 3.0 (1.6-5.6) <0.001† Postoperative Condylar widening > 5 mm 2.0 (1.1-3.5) 0.013† 1.2 (0.7-2.1) 0.59 MPTA < 82° or > 92° 2.9 (1.8-4.7) <0.001† 1.6 (1.0-2.8) 0.05† PPTA < 4° or > 14° 5.2 (3.2-8.7) <0.001† 3.7 (2.1-6.3) <0.001† Articular incongruity <2.0 mm (reference) — — — — 2.0-4.0 mm 0.9 (0.5-1.9) 0.919 0.6 (0.3-1.2) 0.176 >4.0-6.0 mm 5.0 (2.8-9.2) 0.006† 2.7 (1.4-5.0) 0.002† >6.0 mm 5.2 (2.4-11.3) <0.001† 5.0 (2.4-11.2) <0.001†*Adjusted for age, sex, smoking, BMI, and AO/OTA classification. †Significant.
Condylar widening was not associated with conversion to TKA after adjusting for confounders. However, certain other postoperative measurements were associated with conversion. The risk of conversion to TKA was higher among those with an abnormal MPTA (HR = 1.6, 95% CI = 1.0 to 2.8, p = 0.05) and PPTA (HR = 3.7, 95% CI = 2.1 to 6.3, p = 0.001). With regard to articular incongruity, displacement of 2 to 4 mm did not significantly affect the risk compared with the reference group (<2.0 mm). Although the adjusted HR of 0.6 corresponded to an estimated 40% decrease in the (instantaneous) risk of conversion to TKA, the estimated HR was also consistent with an increase of up to 20% according to the CI (HR = 0.6, 95% CI = 0.3 to 1.2, p = 0.176). As the gap or step-off increased beyond 4 mm, the risk of conversion to TKA increased as well. The conversion rate among those with a gap or step-off between 4.0 and 6.0 mm was 2.7 (95% CI = 1.4 to 5.0, p = 0.002) times higher than among the reference group. A gap or step-off of >6.0 mm further increased the risk of conversion to TKA (HR = 5.0, 95% CI = 2.4 to 11.2, p <0.001).
DiscussionAchieving anatomical restoration of the articular surface, adequate tibial alignment, and joint stability are the main goals in surgical treatment of tibial plateau fractures. However, comminuted fractures do not always allow for anatomical reduction. Controversy remains regarding the impact of articular incongruity and tibial alignment on clinical outcome. Our study presents a cohort of surgically treated tibial plateau fractures in which radiographic parameters measuring pre- and postoperative fracture displacement were found to be associated with clinical outcome in terms of conversion to TKA at the time of follow-up. Assessment of preoperative CT scans indicated that substantial initial fracture displacement was independently associated with the need for conversion to TKA. Assessment of postoperative radiographs demonstrated that sagittal and coronal malalignment were strongly associated with conversion to TKA. In contrast to common belief, postoperative gaps or step-offs of <4 mm were not associated with an increased risk of TKA. However, more severe postoperative articular incongruity of >4 mm was associated with an increased risk of conversion to TKA.
Osteoarthritis may still develop after adequate fracture reduction because of extensive irreversible damage to the articular surface caused by the initial trauma. Several studies have indicated that the severity of the fracture is predictive of early-onset osteoarthritis6,17. Additionally, Parkkinen et al. showed that a preoperative step-off of >3.4 mm in medial tibial plateau fractures was predictive of the development of moderate to severe osteoarthritis7. Nevertheless, literature on the association between initial fracture displacement and the risk of conversion to TKA after surgical treatment of tibial plateau fractures is still limited. In line with previous studies6,7,17, we found that substantial initial fracture displacement was a strong predictor of the development of progressive osteoarthritis eventually requiring conversion to TKA. In addition, our results indicated that not only the step-off but also the gap was predictive of the clinical outcome7. Knowledge about the association between substantial initial fracture displacement and an increased risk of conversion to TKA at the time of follow-up may aid in expectation management and patient counseling about the prognosis.
Postoperative assessments of residual incongruity and tibial alignment are essential for decision-making about revision surgery and patient counseling about the prognosis. Much controversy exists regarding the degree of residual displacement that can be accepted. Residual displacement of <2 mm as measured by the gap or step-off is generally considered an adequate reduction11,12. Recent studies have reconfirmed that a residual step-off of >2 mm, as measured on a postoperative radiograph, is associated with worse functional outcomes3,7. However, a review by Giannoudis et al. showed that controversy remains regarding the degree of articular incongruity that can be tolerated in tibial plateau fracture management18. Our recent study demonstrated that a fracture gap or step-off of ≤4 mm, as measured on CT scans, could result in good functional outcomes in patients who opt for nonoperative fracture management19. In addition to these studies, our current results seem to indicate that initial displacement of up to 4 mm does not affect the risk of conversion to TKA. Therefore, the arbitrary 2-mm limit for gaps and step-offs in tibial plateau fractures might be revisited. However, our study did show that greater postoperative incongruity, with displacement exceeding 4 mm, was associated with an increased risk of TKA. Although much literature has focused on residual articular incongruity, hardly any studies have reported on the relationship between the achieved tibial alignment and functional outcome. Recently, Van den Berg et al. reported that sagittal malalignment was associated with worse outcomes and emphasized the importance of restoring the sagittal alignment when treating posterior tibial plateau fractures13. Additionally, Parkkinen et al. showed that coronal malalignment was associated with the development of osteoarthritis and worse pain3,7. However, those studies were limited by small sample sizes and a focus on specific fracture types, and they did not provide HRs. Our study adds to the literature by including >450 patients with all tibial plateau fracture types. Our results indicated that both the postoperative coronal and sagittal malalignment of the tibia were strong predictors of conversion to TKA. Therefore, surgeons should be aware of the importance of restoring tibial alignment when performing surgical management of complex tibial plateau fractures.
This study has several limitations. First, selection bias caused by loss to follow-up and nonresponse is inherent to a cross-sectional study design. Second, meniscal and/or ligamentous injuries might be considered an important confounder, but it was challenging to identify whether the patients in this retrospective study had any meniscal injuries because magnetic resonance imaging or arthroscopy is not regularly performed within our clinics. Nevertheless, we gathered as much information as possible about the impact of concomitant soft-tissue injuries. All patients were contacted and asked whether they had undergone any reintervention, and patient files were verified. Only 7 (0.15%) of 477 patients underwent a reoperation for meniscal or ligamentous repair. Future studies should incorporate concomitant soft-tissue injury and assess its impact on patient outcome. Third, not all radiographs were made by the same radiology technician, and some radiographs may not have been aligned perfectly in the anteroposterior and lateral views or may have had slight differences in magnification since the radiographs were not calibrated. However, this is inherent to clinical practice. Furthermore, there are concerns regarding the interobserver reliability of radiographic measurements even though these measurements are still the gold standard in clinical practice5,20. Gap and step-off measurements in particular are prone to interobserver variability21,22, although measurements of tibial alignment have shown good reliability23,24. Nevertheless, intraobserver measurements within this study showed good reliability for all measurements. Fourth, the number of patients who underwent conversion to TKA was limited since conversion to TKA is relatively uncommon. Finally, our findings may be parochial to the clinical environment from which the substrate was developed and therefore cannot be assumed to be generalizable to other clinical environments. Performance in other clinical contexts should be tested to ensure validity. Given these limitations, this work can only be considered hypothesis-generating and not prescriptive.
Worldwide, fracture displacement and tibial alignment are generally still determined on radiographs and 2-dimensional CT slices. However, more advanced 3-dimensional (3D) imaging techniques are increasingly used in treatment of tibial plateau fractures25. For example, we recently introduced a novel 3D technique to measure intra-articular incongruity in tibial plateau fractures21. Measurements of sagittal alignment of the tibia might also be improved by using 3D technology26. We envision that novel 3D measurements will be increasingly used in addition to current classification systems in order to evaluate the true fracture extent and estimate the prognosis. Furthermore, we chose conversion to TKA as the sole end point in this study since it is a commonly used and unambiguous end point, but the results of surgical treatment could also be evaluated using outcome measures. Future research should therefore focus on the association between radiographic measurements and the risk of poor results as measured by patient-reported outcomes.
In summary, this large multicenter study of medium-term clinical outcomes after tibial plateau fracture surgery demonstrated that substantial initial fracture displacement is a strong independent predictor of conversion to TKA. Moreover, this study showed that postoperative incongruity of >4 mm and sagittal and coronal malalignment were strong independent predictors of conversion to TKA at the time of follow-up. These findings can be used as a guideline for counseling patients with complex tibial plateau fractures and could help to estimate the prognosis.
References 1. Tscherne H, Lobenhoffer P. Tibial plateau fractures. Management and expected results. Clin Orthop Relat Res. 1993 Jul;(292):87-100. 2. Prat-Fabregat S, Camacho-Carrasco P. Treatment strategy for tibial plateau fractures: An update. EFORT Open Rev. 2017 Mar 13;1(5):225-32. 3. Parkkinen M, Madanat R, Mustonen A, Koskinen SK, Paavola M, Lindahl J. Factors predicting the development of early osteoarthritis following lateral tibial plateau fractures: mid-term clinical and radiographic outcomes of 73 operatively treated patients. Scand J Surg. 2014 Dec;103(4):256-62. 4. Meulenkamp B, Martin R, Desy NM, Duffy P, Korley R, Puloski S, Buckley R. Incidence, Risk Factors, and Location of Articular Malreductions of the Tibial Plateau. J Orthop Trauma. 2017 Mar;31(3):146-50. 5. Marsh JL, Buckwalter J, Gelberman R, Dirschl D, Olson S, Brown T, Llinias A. Articular fractures: does an anatomic reduction really change the result? J Bone Joint Surg Am. 2002 Jul;84(7):1259-71. 6. Manidakis N, Dosani A, Dimitriou R, Stengel D, Matthews S, Giannoudis P. Tibial plateau fractures: functional outcome and incidence of osteoarthritis in 125 cases. Int Orthop. 2010 Apr;34(4):565-70. 7. Parkkinen M, Lindahl J, Mäkinen TJ, Koskinen SK, Mustonen A, Madanat R. Predictors of osteoarthritis following operative treatment of medial tibial plateau fractures. Injury. 2018 Feb;49(2):370-5. 8. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Bull World Health Organ. 2007 Nov;85(11):867-72. 9. Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Introduction: fracture and dislocation classification compendium-2018. J Orthop Trauma. 2018 Jan;32(Suppl 1):S1-170. 10. Johannsen AM, Cook AM, Gardner MJ, Bishop JA. Defining the width of the normal tibial plateau relative to the distal femur: Critical normative data for identifying pathologic widening in tibial plateau fractures. Clin Anat. 2018 Jul;31(5):688-92. 11. Barei DP, Nork SE, Mills WJ, Coles CP, Henley MB, Benirschke SK. Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates. J Bone Joint Surg Am. 2006 Aug;88(8):1713-21. 12. Barei DP, Nork SE, Mills WJ, Henley MB, Benirschke SK. Complications associated with internal fixation of high-energy bicondylar tibial plateau fractures utilizing a two-incision technique. J Orthop Trauma. 2004 Nov-Dec;18(10):649-57. 13. Van den Berg J, De Boer AS, Assink N, Haveman R, Reul M, Link BC, Ijpma FFA, Verhofstad MHJ, Hoekstra H. Trauma mechanism and patient reported outcome in tibial plateau fractures with posterior involvement. Knee. 2021 Jun;30:41-50. 14. Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, Jordan JM, Kington RS, Lane NE, Nevitt MC, Zhang Y, Sowers M, McAlindon T, Spector TD, Poole AR, Yanovski SZ, Ateshian G, Sharma L, Buckwalter JA, Brandt KD, Fries JF. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med. 2000 Oct 17;133(8):635-46. 15. Prediger B, Tjardes T, Probst C, Heu-Parvaresch A, Glatt A, Dos Anjos DR, Bouillon B, Mathes T. Factors predicting failure of internal fixations of fractures of the lower limbs: a prospective cohort study. BMC Musculoskelet Disord. 2021 Sep 16;22(1):798. 16. Heidari B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: Part I. Caspian J Intern Med. 2011 Spring;2(2):205-12. 17. Jansen H, Frey SP, Doht S, Fehske K, Meffert RH. Medium-term results after complex intra-articular fractures of the tibial plateau. J Orthop Sci. 2013 Jul;18(4):569-77. 18. Giannoudis PV, Tzioupis C, Papathanassopoulos A, Obakponovwe O, Roberts C. Articular step-off and risk of post-traumatic osteoarthritis. Evidence today. Injury. 2010 Oct;41(10):986-95. 19. Vaartjes TP, Assink N, Nijveldt RJ, van Helden SH, Bosma E, El Moumni M, Duis KT, Hogervorst M, Doornberg JN, de Vries JPM, Hoekstra H, IJpma FFA. Long-term functional outcome after nonoperative management of tibial plateau fractures: what sizes of gaps and step-offs can be accepted? Clin Orthop Relat Res. 2022 Dec 1;480(12):2288-2295. 20. Martin J, Marsh JL, Nepola JV, Dirschl DR, Hurwitz S, DeCoster TA. Radiographic fracture assessments: which ones can we reliably make? J Orthop Trauma. 2000 Aug;14(6):379-85. 21. Assink N, Kraeima J, Slump CH, Ten Duis K, de Vries JPPM, Meesters AML, van Ooijen P, Witjes MJH, IJpma FFA. Quantitative 3D measurements of tibial plateau fractures. Sci Rep. 2019 Oct 7;9(1):14395. 22. Meesters AML, Ten Duis K, Kraeima J, Banierink H, Stirler VMA, Wouters PCR, de Vries JPPM, Witjes MJH, IJpma FFA. The accuracy of gap and step-off measurements in acetabular fracture treatment. Sci Rep. 2021 Sep 14;11(1):18294. 23. Gordon JE, Chen RC, Dobbs MB, Luhmann SJ, Rich MM, Schoenecker PL. Interobserver and intraobserver reliability in the evaluation of mechanical axis deviation. J Pediatr Orthop. 2009 Apr-May;29(3):281-4. 24. Bernhardson AS, DePhillipo NN, Daney BT, Kennedy MI, Aman ZS, LaPrade RF. Posterior Tibial Slope and Risk of Posterior Cruciate Ligament Injury. Am J Sports Med. 2019 Feb;47(2):312-7. 25. Assink N, Reininga IHF, Ten Duis K, Doornberg JN, Hoekstra H, Kraeima J, Witjes MJH, de Vries JPM, IJpma FFA. Does 3D-assisted surgery of tibial plateau fractures improve surgical and patient outcome? A systematic review of 1074 patients. Eur J Trauma Emerg Surg. 2022 Jun;48(3):1737-49. 26. Hoch A, Jud L, Roth T, Vlachopoulos L, Fürnstahl P, Fucentese SF. A real 3D measurement technique for the tibial slope: differentiation between different articular surfaces and comparison to radiographic slope measurement. BMC Musculoskelet Disord. 2020 Sep 26;21(1):635.
留言 (0)