
記住我






Parents of autistic children experience increased levels of caregiver strain and higher rates of general mental health concerns compared to parents of neurotypical (NT) children, and those with other neurodevelopmental disabilities (Abbeduto et al., 2004; Davis and Carter., 2008; Estes et al., 2009, 2013; Hartley et al., 2012). Several studies have reported increased rates of depression (Abbeduto et al., 2004; Hartley et al., 2012; Cohrs and Leslie, 2017) among parents of autistic children. Additionally, in one study of 52 parents of autistic children, researchers reported that 53.8% of the parents show clinically significant mental health concerns (Nikmat et al., 2008), with mothers reporting a greater adverse impact on psychological wellbeing compared to fathers (Nikmat et al., 2008). Understanding parents’ caregiver strain, mental health, and wellbeing is particularly important, as research has demonstrated that parents play an important role in scaffolding their children’s development (e.g., maternal sensitivity influences child expressive language growth; Greenberg et al., 2006; Baker et al., 2010). Caregiver strain is also associated with greater use of maladaptive parenting styles that may exacerbate behavioral regulation difficulties in autistic children (Hutchison et al., 2016). Thus, ignoring parental mental health needs will make it difficult to support child development because of the transactional nature of the relationships among the members of a family system (Gulsrud et al., 2010).
Most of the prior literature exploring predictors of parents’ caregiver strain, mental health, and wellbeing have focused primarily on the impact of autistic children’s autism symptom severity. Specifically, higher rates of adverse parental mental health and increased caregiver strain have previously been attributed to perceived behavioral challenges associated with their child’s autism (Smith et al., 2008; Lyons et al., 2010; Ingersoll and Hambrick, 2011; Hartley et al., 2012; He et al., 2022; Porter et al., 2022). However, less attention has been given to other parent and child factors that may impact caregiver strain and mental health in parents (e.g., wellbeing, depression, anxiety). Further, few studies have explored how parent factors may mitigate the adverse impact of other child factors on mental health and wellbeing in parents of autistic children (Weiss et al., 2012). The present study explored the impact of child and parent-specific factors on parents’ caregiver strain, mental health, and wellbeing. Additionally, we examine the potential mitigating role of parents’ emotion regulation on the impact of child factors on parents’ mental health and wellbeing.
Predictors of caregiver strain, mental health, and wellbeingFactors related to increased caregiver strain among parents of autistic children have been explored in numerous reports, with children’s cognitive challenges and severity of autism symptoms being associated with increased caregiver strain (Abbeduto et al., 2004; Lecavalier et al., 2006; Davis and Carter., 2008; Rao and Beidel, 2009; Hartley et al., 2012; Karst and Van Hecke, 2012; Smith et al., 2012) and depression (Benson and Karlof, 2009; Ingersoll and Hambrick, 2011). Additionally, children’s behavioral concerns, such as dysregulation and externalizing behaviors, have been found to be highly correlated with caregiver strain in parents of autistic children (Davis and Carter., 2008), which in turn was associated with parents’ higher levels of anxiety and depression (Rezendes and Scarpa, 2011). Increased caregiver strain is also related to increased rates of children’s restricted and repetitive behaviors (RRBs), with parents citing difficulty managing these behaviors adding to their own caregiver strain (Mercier et al., 2000; Gabriels et al., 2005; Lecavalier et al., 2006; Bishop et al., 2007). Furthermore, studies suggest that greater parental involvement in a child’s day-to-day activities (e.g., involvement with daily routine, school, domestic duties) may lead to greater caregiver strain and negatively impact the family system (Tehee et al., 2009).
Resilience of parents of autistic childrenData also suggest resiliency, or the ability to positively adapt to the environment in the face of adversity or challenge (Luthar et al., 2000), in many parents of autistic children. Specifically, positive meaning-making (e.g., diagnosis as a strength for the family unit, acknowledging available resources) of the experience as caregivers of autistic children can buffer against stressful situations (Barakat and Linney, 1992; Anuradha, 2004; Wilgosh and Scorgie, 2006). Further, research has demonstrated that social support, hope and spirituality and religiosity are important protective factors for caregiver strain, mental health and wellbeing (Lyons et al., 2010; Ekas et al., 2016; Slattery et al., 2017; Pepperell et al., 2018). Although research has identified a range of resilience factors for parents of autistic children, little is known regarding the impact of parent emotion regulation abilities on caregiver strain and wellbeing in this population.
Emotion regulation as resilienceEmotion regulation (ER) is an umbrella term that refers to the ability to monitor, evaluate and modify emotional reactions (Gross, 1998). In the general population of NT adults, difficulties with ER have been associated with a range of mental health concerns, including increased rates of anxiety and depression (Mennin et al., 2007; Etkin et al., 2010; Cludius et al., 2020). Additionally, ER abilities have been associated with indices of wellbeing in NT adults, with lower ER abilities predicting lower self-reported wellbeing (Haga et al., 2009; Mandal et al., 2011).
Despite the research supporting the impact of ER abilities on individuals’ mental health and wellbeing in the general population, few studies have examined these associations in parents. These studies find that ER abilities play an important role in supporting parents’ mental health and wellbeing. In one recent study of caregivers of NT children during the COVID-19 pandemic, caregivers’ ER abilities predicted their mental health 2 months later (Russell et al., 2022). In another study, researchers provided an online ER intervention to parents, targeting the use of adaptive ER strategies (Preuss et al., 2021). Findings revealed that parents who received the intervention had a significant decrease in parenting stress at follow-up in comparison to the wait-list control group (Preuss et al., 2021). With regard to parents of autistic children, even less is known. To our knowledge, one study to date has examined the association between ER and parenting stress in parents of autistic children. In this study, Hu et al. (2019) found a significant, negative association between parents’ ER abilities and their self-reported parenting stress. Further research is needed to better understand the impact of ER abilities on mental health and wellbeing for parents of autistic children.
Mothers and fathers of autistic childrenIn studies of the general population of heterosexual couples, fathers play important, but distinct, and complementary roles to mothers in many families. However, fathers of children with developmental disabilities, including autism, have been studied infrequently regarding their roles and relationships within the family. In the studies that have been conducted, child characteristics, partner characteristics, and features of the marital relationship have been found to differentially affect mothers and fathers of children with autism or other disabilities (Bristol et al., 1988; Hartley et al., 2016). There is evidence, for example, that fathers are more negatively affected by their autistic child’s behavioral concerns than are mothers (Davis and Carter., 2008). Moreover, it is likely that the psychological state of one parent may affect that of the other parent in two-parent families (Hastings, 2003). In fact, maternal symptoms of depression have been found to predict paternal psychological wellbeing in families with autistic children (Hartley et al., 2012). Research suggests that mothers and fathers also differ in their adaptability (Bendixen et al., 2011) and in the types of support they provide for their families (emotional vs. practical support, respectively; Seligman and Darling, 2009).
There are inconsistent findings with respect to differences in caregiver strain, mental health, and wellbeing between fathers and mothers of autistic children. Studies examining mental health outcomes in parents of autistic children have largely found that mothers report higher levels of depression (Hastings et al., 2005; Ozturk et al., 2014; Foody et al., 2015; Cohrs and Leslie, 2017; Li et al., 2022) and anxiety (Hastings, 2003; Foody et al., 2015; Li et al., 2022) than do fathers of autistic children. Less consistent findings have been found regarding caregiver strain or stress, with some studies reporting higher rates of parenting stress in mothers as compared with fathers (Moes et al., 1992; Sharpley et al., 1997; Tehee et al., 2009; Dabrowska and Pisula, 2010; Falk et al., 2014). Other studies have reported no significant difference in parenting stress between mothers and fathers of autistic children (Hastings, 2003; Davis and Carter., 2008; Nikmat et al., 2008; Ozturk et al., 2014). These studies typically involve small samples thus, they have had limited statistical power to detect differences between mothers and fathers and are limited in potential generalizability. Moreover, studies involving fathers have not focused on the role of ER, or the potential protective factors associated with positive outcomes. Overall, the inconsistencies in these data demonstrate a need for further research into the unique role of mothers and fathers of autistic children.
The current studyThis study was designed to leverage a large sample to explore the relationship between autistic children’s behavioral characteristics and parents’ psychosocial risk and resilience, as well as to evaluate the potential role of ER as a protective factor for parents. In addition, mothers and fathers from the same family are included in analyses, thereby allowing exploration of differences in their psychosocial risk and resilience. It was hypothesized that children’s higher RRBs and behavioral concerns, and lower adaptive functioning abilities (i.e., tasks of daily living), would be associated with increased caregiver strain and adverse mental health. Additionally, it was hypothesized that higher ER abilities in parents would be associated with lower levels of caregiver strain and more positive mental health outcomes, and that ER would moderate the association between child factors and indicators of parents’ mental health and wellbeing. Lastly, it was hypothesized that mothers in our sample would report significantly higher rates of caregiver strain, anxiety and depression than would fathers.
Materials and methods SPARK cohortBeginning in April 2016, SPARK began a nationwide recruitment effort with 21 clinical sites (growing to include 31 in 2021) and an extensive social media campaign. Any individual living in the United States with a professional diagnosis of ASD (obtained from a provider or through school), along with their parents and an unaffected sibling, are eligible to participate in SPARK. Phenotypic data and biospecimens are collected remotely, with online access to the study protocol, making participation more accessible and convenient. Participants consent to share their de-identified data, and to be contacted for future ASD-related research studies for which they may be eligible. Additionally, participants may consent to contribute a saliva sample for genetic analysis and may opt to receive individual genetic results related to ASD, in the event that a primary genetic cause of ASD is identified. For a detailed description of genetic material collection, genomic analyses and return of results to participants see Feliciano et al.’s (2019) publication. SPARK participants are also asked to complete a battery of online questionnaires.
SPARK research matchThe data for the current project was obtained through the SPARK Research Match program, which connects qualified members of the SPARK community with research studies, inviting them to volunteer as participants. Data were accessed by submitting an application to SFARI Base, describing the aims of the study, as well as a description of the inclusion criteria for the proposed project. The application was reviewed and approved by the SPARK Participant Access Committee (PAC), and participants who met study criteria were invited to participate in the current study. Data collection took place between January and February of 2021, during which time the participants completed a battery of online surveys regarding proband characteristics, in addition to psychological risk and resilience for both biological parents.
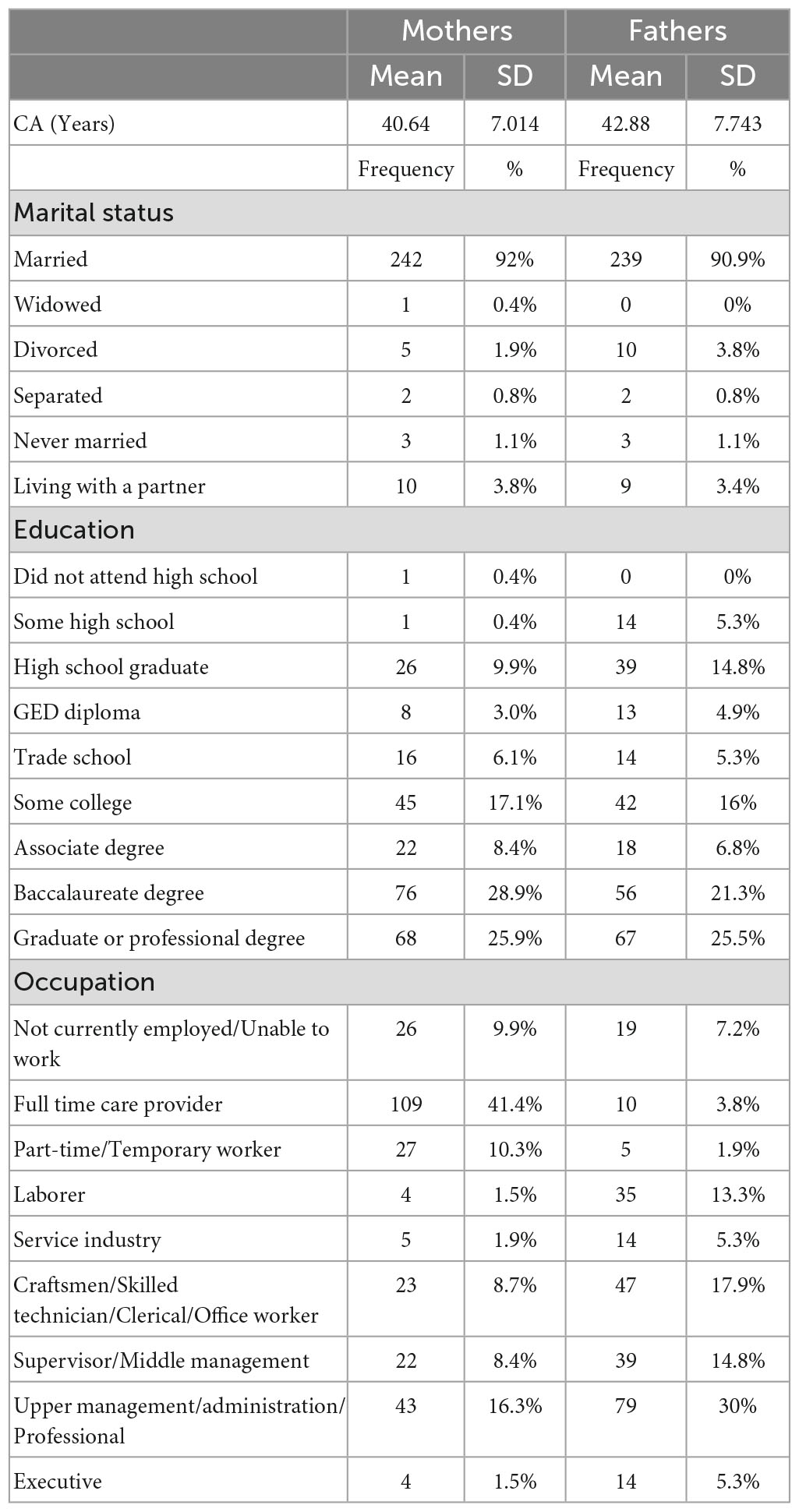
ParticipantsThe overall SPARK sample included 106,577 probands, the parents of whom were invited to participate in the current study if they met the following criteria: (1) the proband was less than 18 years old and (2) both biological parents were available to participate. This resulted in a sample of 263 dyads (biological mother, biological father) that participated in the online survey study. Probands were largely male (77.9%) and had an average age of 7.37 years (SD = 3.92; range = 1–17 years). A majority of probands identified as White (63.9%), with the remainder identifying as Asian (1.1%), African American (4.2%) and Other (3.4%). A portion of the sample identified as having multiple races (9.5%), and 17.9% did not endorse a race. Lastly, 11.0% of the sample identified as ethnically Hispanic. Maternal and paternal demographics are presented in Table 1.
Table 1. Mother and father demographic information.
Child measuresChild Behavior Checklist (CBCL; Achenbach and Rescorla, 2001). The Child Behavior Checklist, now known as the Achenbach System of Empirically Based Assessments, is a parent report questionnaire that measures the presence of behavioral and emotional challenges in children. The most recent version of the CBCL includes two separate forms, one to be used with children between the ages of 1.5 and 5 years and the second to be used with children between the ages of 6 and 18. Both forms of the CBCL have been found to have strong internal consistency (α = 0.92–0.94) and test-retest reliability in the norming sample (r = 0.89–0.92; Achenbach and Rescorla, 2001). Additionally, both scales have been demonstrated to have acceptable construct and criterion validity (Achenbach and Rescorla, 2001). The assessment yields scores across 6 different scales (affective problems, attention-deficit/hyperactivity, anxiety, oppositional defiance, somatic problems, and conduct problems), and three composite scores (Internalizing problems, Externalizing problems and Total Problems). For the purposes of the current study, the Total Problems score was used as a measure of children’s emotional and behavioral concerns (hereafter referred to as behavioral concerns for readability). The choice was made to exclude subscales from the analyses, as two different forms of the CBCL were used (1.5–5 and 6–18) which include different subscales.
Repetitive Behavior Scale–Revised (RBS-R; Bodfish et al., 1999). The RBS-R is an informant-report instrument that measures the presence and severity of restricted and repetitive behaviors, consisting of 43 items across six subscales (Stereotyped Behavior, Self-injurious behavior, Compulsive Behavior, Routine Behavior, Sameness Behavior, and Restricted Behavior). This measure was completed by parents, who rated their child’s behaviors on a 4-point Likert scale, ranging from “0” (behavior does not occur) to “3” (behavior is a severe problem). The measure was found to have good inter-rater reliability (r = 0.88) and test-retest reliability in the norming sample (r = 0.71; Bodfish et al., 1999). The RBS-R yields an overall total raw score, based on summed items scores across subscales, which was used in this study as a measure of individual’s restricted, repetitive behaviors.
Vineland Adaptive Behavior Scale–Third Edition (VABS-3; Sparrow et al., 2016). The VABS-3 is considered the gold-standard measure of adaptive functioning for individuals from birth to 90 years old. Parents in the current study completed the caregiver questionnaire version of the assessment, which has been found to have strong internal consistency (α = 0.96–0.99) and acceptable test-retest reliability in the norming sample (r = 0.80–0.93; Sparrow et al., 2016). The measure has been shown to correlate with other measures of adaptive functioning (Sparrow et al., 2016), including the Bayley Scales of Infant and Toddler Development (Bayley-III; Bayley, 2006) and the Adaptive Behavior Assessment System (ABAS-3; Harrison and Oakland, 2015). The VABS-3 provides composite standard scores (M = 100, SD = 15) across four domains (Communication, Daily Living Skills, Socialization and Motor), in addition to an overall Adaptive Behavior Composite (ABC). The ABC standard score was used for the current study as a measure of overall adaptive functioning. We did not include analyses of the subdomains of the VABS-3 because 3 of the 4 subdomains are not normed for children under the age of 3 years, which would exclude part of our sample.
Parent measuresCaregiver Strain Questionnaire–Short Form (CGSQ-SF; Brannan et al., 1997). The CGSQ-SF is a self-report measure that assesses parenting strain in the previous month. It consists of 10 items derived from the original long form, measuring strain across two subscales: Objective strain (6 items) and Subjective Internalized strain (4 items). Response options are in the form of a 5-point Likert scale, ranging from “Not a problem” (1) to “Very much a problem” (5). The CGSQ-SF Total Score, a score derived from the mean of all items, was used in this study to characterize overall caregiving strain. The CGSQ-SF has strong psychometric properties, with an internal consistency reliability coefficient of 0.90 (Brannan et al., 2012).
Patient Health Questionnaire (PHQ-9; Kroenke and Spitzer, 2002). The PHQ-9 is a self-report questionnaire measuring depression, adapted from the depression module of the PRIME-MD diagnostic instrument for common mental disorders. It consists of 9 items, each of which represents one of nine DSM-IV criteria for major depression. Item responses are measured using a 3-point Likert scale, ranging from “Not at all” (1) to “Nearly every day” (3). The PHQ-9 was found to have strong internal reliability (0.86–0.89; Kroenke and Spitzer, 2002) and test-retest reliability in the norming sample (0.84; Kroenke and Spitzer, 2002). It was also found to have strong construct and criterion validity (Kroenke and Spitzer, 2002). The measure yields a total score that represents the severity of respondents’ depression symptoms.
Generalized Anxiety Disorder (GAD-7; Spitzer et al., 2006). The GAD-7 is a self-report questionnaire that assess symptoms of generalized anxiety, asking participants how often in the previous 2 weeks they have been bothered by anxiety symptoms. The measure consists of 7 items, scored on a 4-point Likert scale ranging from “Not at all” (0) to “Nearly every day” (3). The measure was found to have strong psychometric properties, with good internal consistency (Cronbach α = 0.92; Spitzer et al., 2006) and test-retest reliability in the norming sample (ICC = 0.83; Spitzer et al., 2006). Additionally, this measure was found to have strong evidence of criterion, construct and factorial validity (Spitzer et al., 2006). The measure yields a total score between 0 and 21, with higher scores indicated greater anxiety symptomatology.
Wellbeing Scale (WBS; Ryff and Keyes, 1995; Keyes et al., 2002). A modified version of Ryff’s Scales of Psychological Well Being, the Wellbeing Scale includes a total of 18 items across 6 aspects of wellbeing: self-acceptance, autonomy, environmental mastery, purpose in life, positive relations with others, and personal growth. Responses are measured using a 7-point Likert scale ranging from “Strongly agree” (1) to “Strongly disagree” (7). While there have been mixed findings on the psychometrics of the modified form (Ryff and Keyes, 1995; Springer and Hauser, 2006), it has been widely used in the literature examining wellbeing in diverse samples (Clarke et al., 2001; Sagone and De Caroli, 2014; Khanjani et al., 2018). The measure yields a total mean score, such that a higher score reflects greater wellbeing.
Barkley Deficits in Executive Functioning Scale (BDEFS; Barkley, 2011b). The BDEFS is a self-report measure of individuals’ executive functioning abilities. It is comprised of 89 items that are answered using a 4-point Likert scale ranging from “1” (rarely or not at all) to “4” (very often). It consists of items across five subscales (self-management of time, self-organization/problem-solving, self-restraint, self-motivation and self-regulation of emotions). The measure is reported to have excellent internal consistency in the norming sample (α = 0.92; Barkley, 2011b). For the purposes of the current study, we present scores from the self-regulation of emotions subscale (13 items), as a measure of participants’ ER. Included in the self-regulation of emotions subscale are items designed to measure participants’ ability to regulate negative emotions, such as “Have trouble calming myself down once I am emotionally upset” and “Unable to manage my emotions in order to accomplish my goals successfully or get along with others.” Scores are calculated as a sum of scores across items, such that higher scores indicate poorer ER.
Data analysisPreliminary analyses were conducted to provide sample demographics and summary statistics (means and standard deviations) of all variables of interest. Data were analyzed to confirm that all assumptions of linear mixed effects models were met.
We used linear mixed effects models to assess the contribution of child characteristics to caregiving strain and mental health. Each parental outcome (CGSQ-SF, PHQ, GAD, and WBS) was modeled separately. We first modeled each parental outcome (CGSQ-SF, PHQ, GAD, and WBS) as a function of child characteristics (CBCL, VABS, and RBS-R), parent (mother/father) and all two-way interactions between child characteristics and parent. A random effect was included for each child to account for within-child correlation. Because four outcomes were analyzed, a Bonferroni corrected alpha level of 0.0125 was used to determine significance. If no interactions were significant, main effect only models were fit; otherwise, all interactions were retained in the model. We then tested the possible moderating effect of parents’ ER abilities by including BDEFS-ER as a main effect and two-way (BDEFS-ER*Child characteristic) and three-way interactions (BDEFS-ER*Parent*Child characteristic). All predictors and the moderator were centered and scaled to a mean of 0 and standard deviation of 1. Moderation models were also evaluated at a Bonferroni significance level of 0.0125. Main effects only models were fit if no interactions were significant, but all interactions retained if some were significant. Analyses were conducted using R Statistical Software version 4.2.0.
Results Child and parent characteristicsOn average, children in this sample had a mean Adaptive Behavior Composite Standard Score (ABC-SS) that fell in the “moderately low” range (M = 71.53, SD = 15.18), and a mean Total Problems score in the “clinical” range (M = 65.63, SD = 8.94). Additionally, children in the sample had a mean score of 33.85 on the RBS-R (out of a possible score of 129), with a large amount of variability (SD = 19.66).
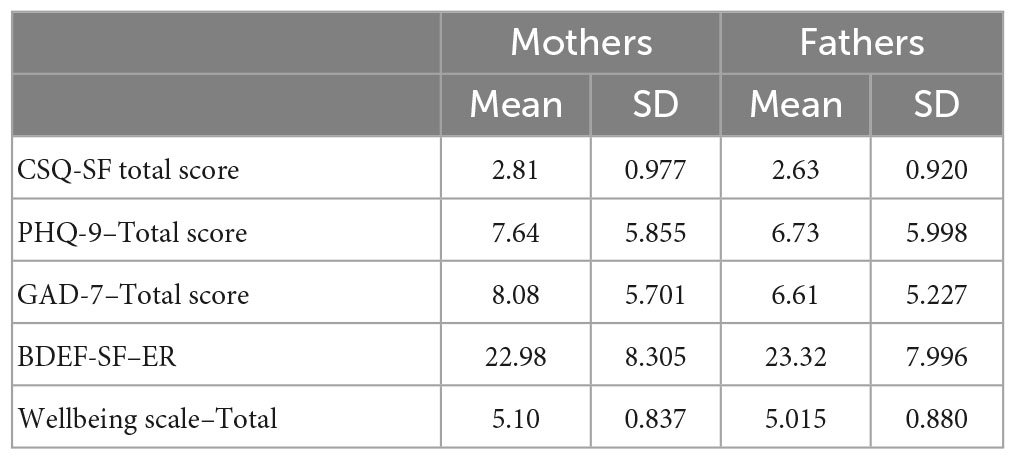
Parents in this sample reported symptoms of mild depression and mild anxiety, as measured by the PHQ-9 and GAD-7, respectively. Additionally, both mothers and fathers in this sample had a CGSQ total score that fell in the “medium” range (see Table 2).
Table 2. Mother and father indicators of risk and resilience.
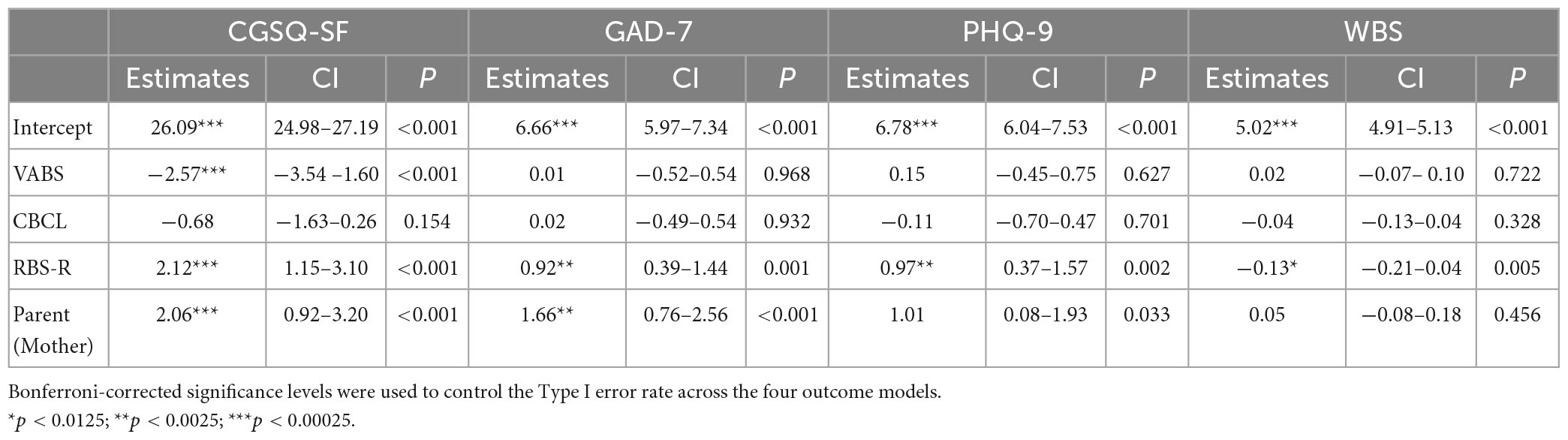
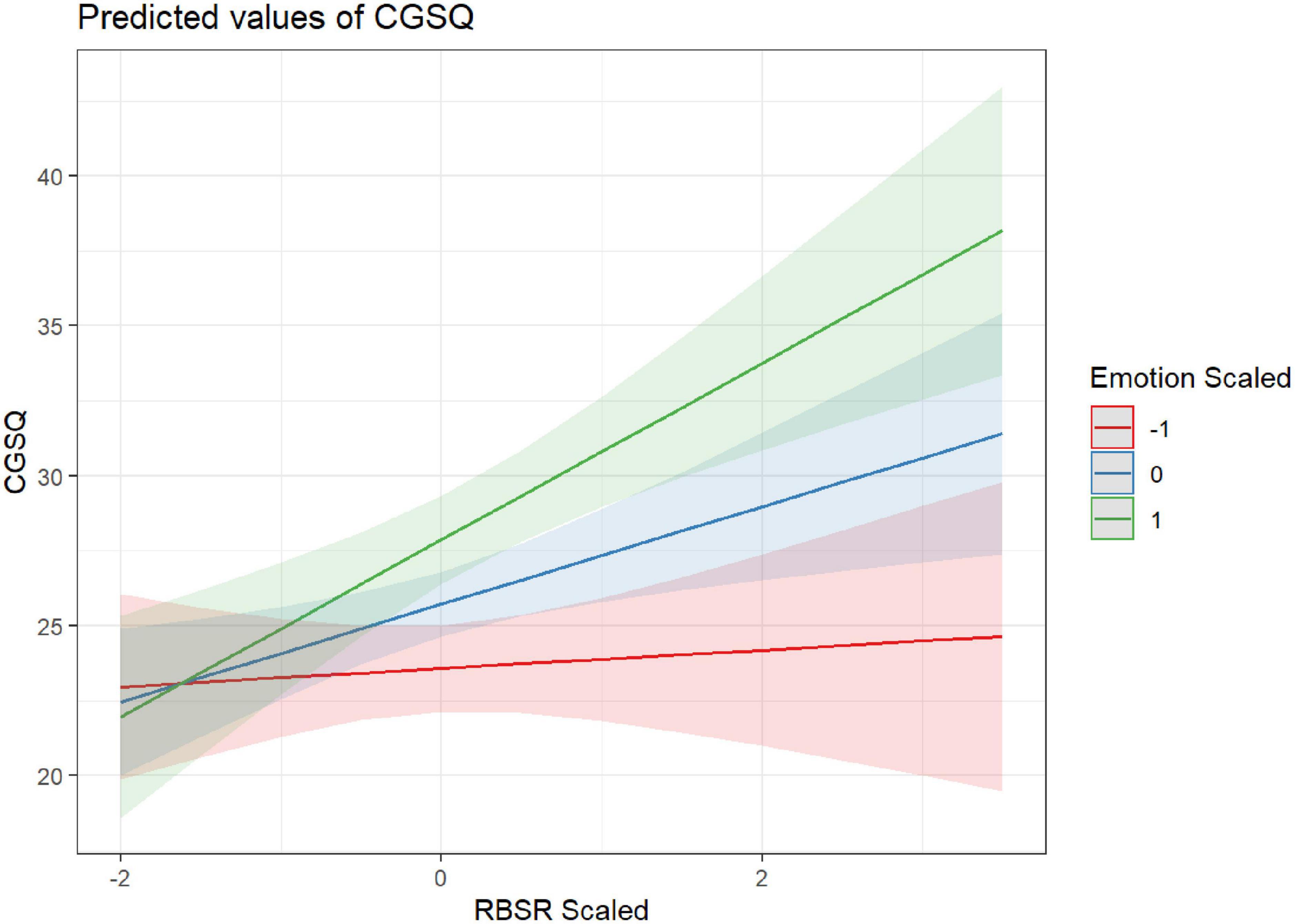
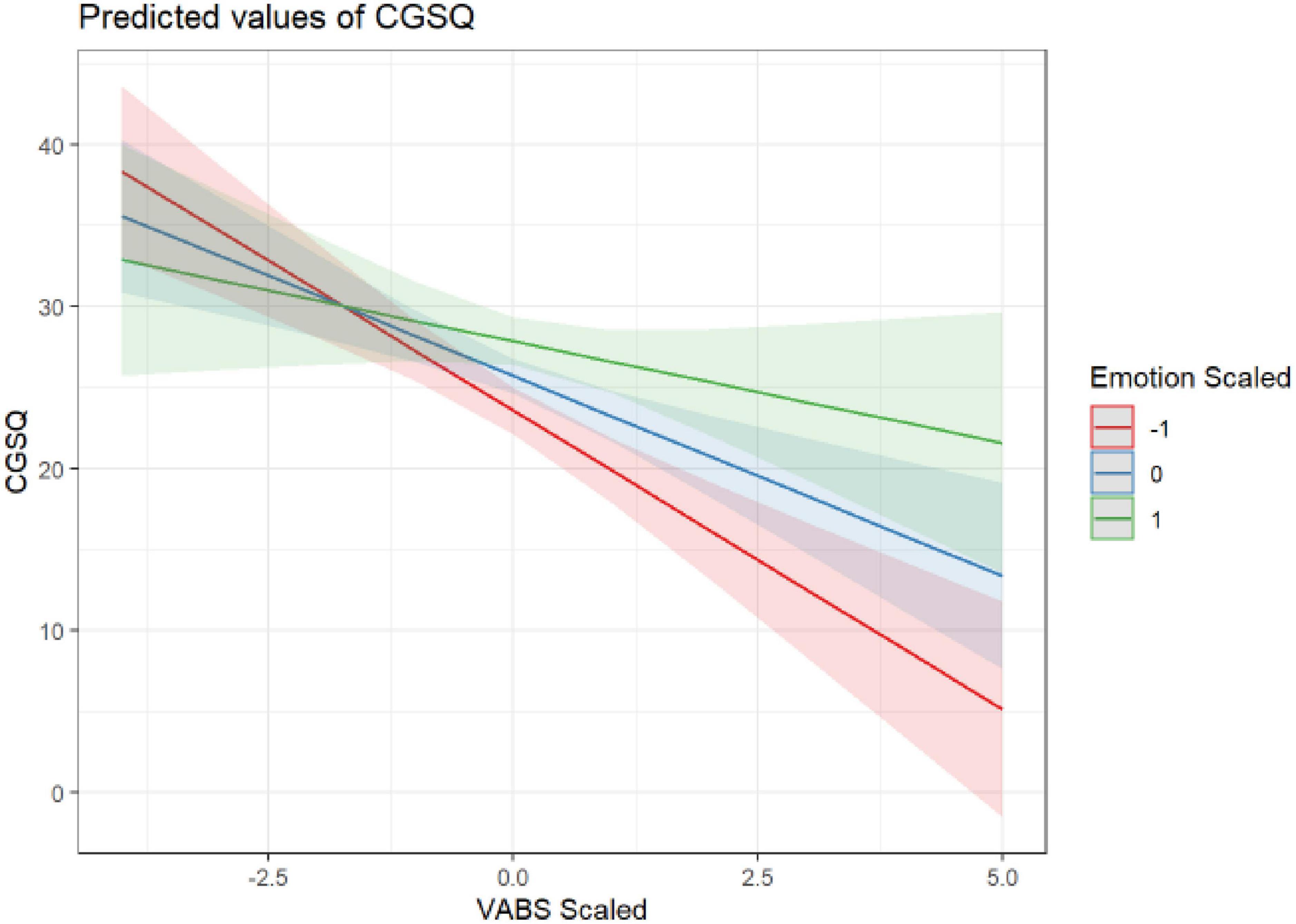
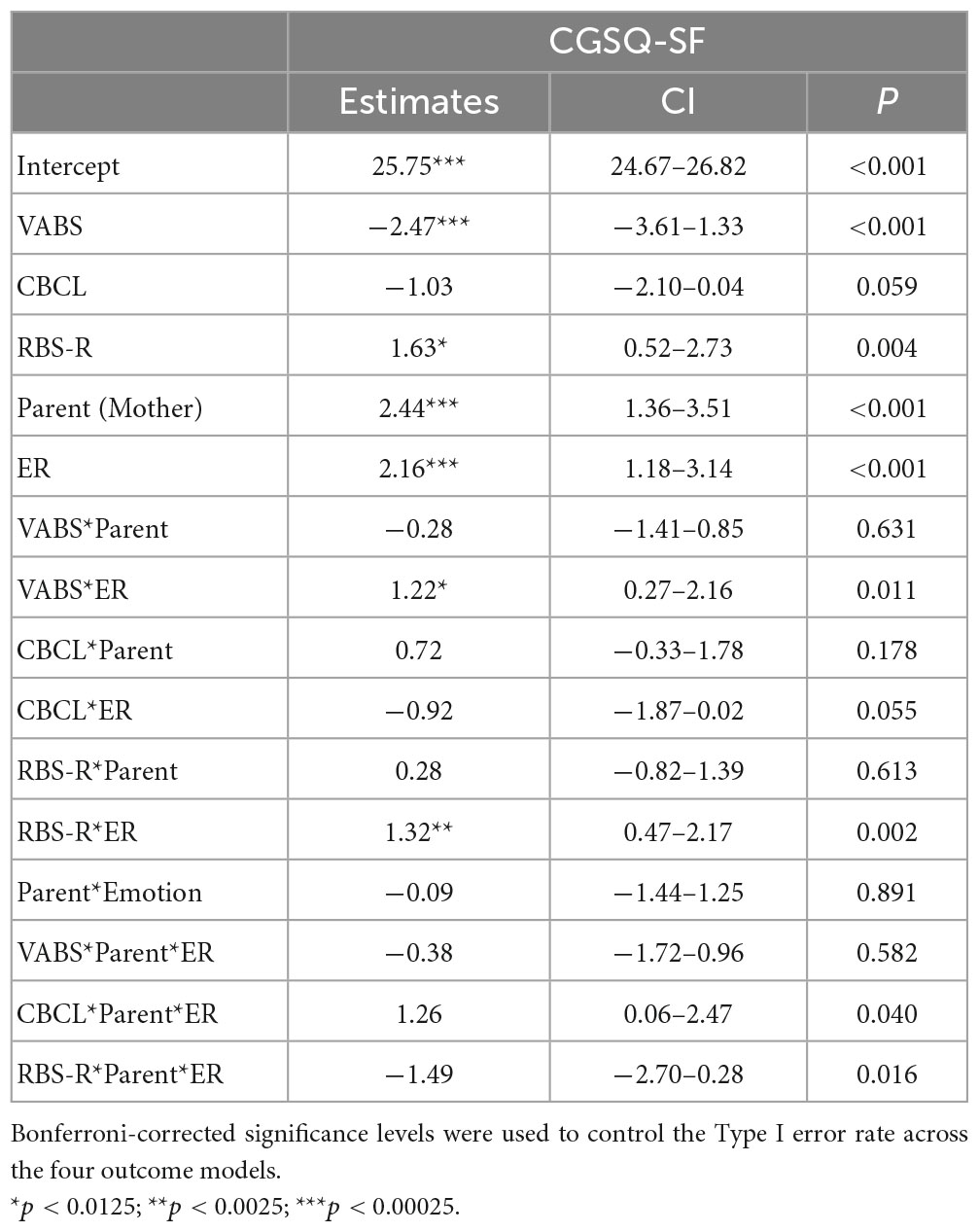
Associations between parental outcomes and child characteristicsTwo child characteristics, adaptive functioning (VABS-3) and repetitive behaviors (RBS-R), significantly predicted parents’ caregiver strain (CGSQ-SF), such that higher caregiver strain was associated with children’s lower adaptive functioning (β = −2.57; p < 0.001) and higher repetitive behaviors [(β = 2.12; p < 0.001; see Table 3)]. These relationships were not found to differ significantly by parent (Supplementary Table 1). Additionally, parents’ ER abilities moderated the effect of children’s RRBs on caregiving strain (β = 1.32; p = 0.002), such that parents with higher ER abilities (indicated by lower scored on BDEFS-ER) experienced smaller increases in caregiver strain for a given increase in a child’s RRBs. Although not statistically significant at the Bonferroni corrected level of 0.0125, there was some indication that the moderating effect of BDEFS-ER was considerably less for mothers than fathers (β = 1.49; p = 0.016). Similarly, parents’ ER abilities also moderated the effect of children’s adaptive functioning abilities on parents’ caregiver strain (β = 1.22; p = 0.011), such that parents with higher ER abilities experienced lower levels of caregiver strain in response to their children’s lower adaptive functioning abilities. See Figures 1, 2 and Table 4 for more information.
Table 3. Results of main effects only linear mixed effect models evaluating the effect of child characteristics on the four parent outcomes.
Figure 1. ER moderating the effect of RRBs on CGSQ.
Figure 2. ER moderating the effect of VABS on CGSQ.
Table 4. Results of mixed effect models evaluating the moderating effect of parents’ ER on the association between child characteristics and caregiver strain.
For the models of parents’ depression, anxiety and wellbeing, RBS-R was a significant predictor (Table 3), with increases in RRBs associated with higher anxiety (β = 0.92; p = 0.001) and depression (β = 0.97; p = 0.002), and lower wellbeing (β = −0.13; p = 0.005), although these results did not remain significant upon the inclusion of BDEFS-ER in the models. Additionally, these relationships did not differ significantly between mothers and fathers (Supplementary Table 1).
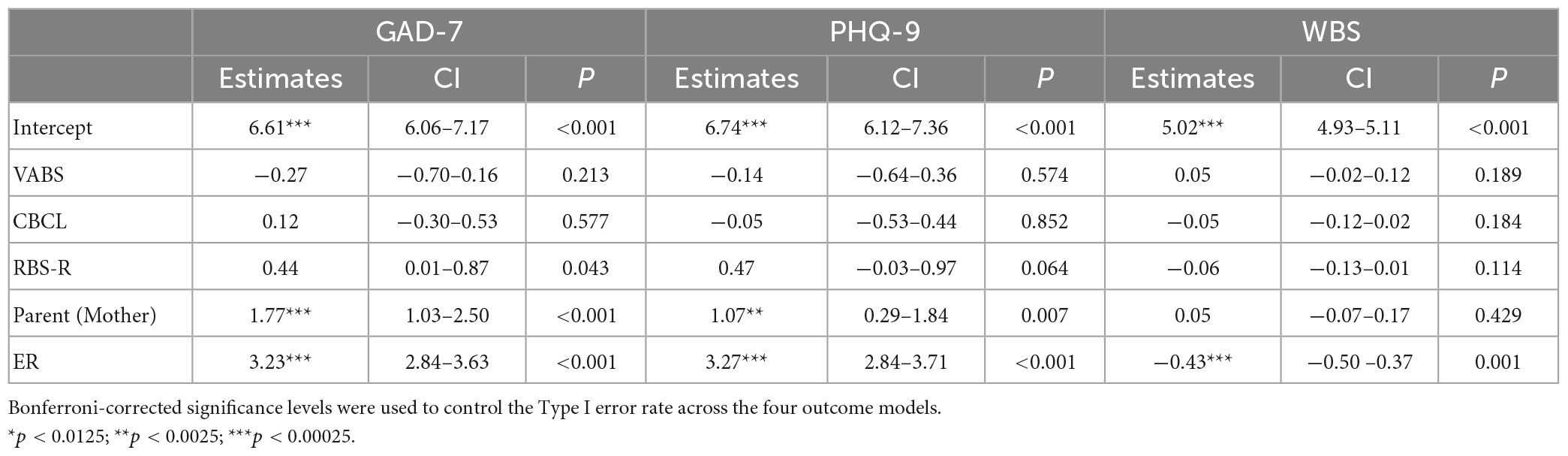
Parents’ ER abilities significantly predicted parents’ depression (β = 3.23; p < 0.001) and anxiety (β = 3.27; p < 0.001), such that parents with higher ER abilities had fewer symptoms of depression and anxiety. Additionally, a significant effect for parents’ ER was seen for parents’ wellbeing (β = −0.13; p = 0.005), with higher ER predicting higher wellbeing. See Table 5 for details. There was no evidence of different effects of ER on depression, anxiety and wellbeing between mothers and fathers (Supplementary Table 2).
Table 5. Results of main effects only linear mixed effect models evaluating the effect of parents’ ER and child characteristics on parent mental health outcomes.
Lastly, a significant main parent effect was detected, such that mothers reported experiencing higher caregiver strain (β = 2.06; p < 0.001) and anxiety (β = 1.66; p < 0.001) than fathers. See Table 3 for further details on all models.
DiscussionThe current study examined contributors to, and potential mitigators of, strain, wellbeing, and mental health outcomes in parents of autistic children. Consistent with previous findings in the literature, parent self-reported caregiving strain was associated with children’s adaptive functioning abilities and restricted and repetitive behaviors (RRB) (Bishop et al., 2007). In previous studies, increased rates of RRBs have been associated with higher levels of caregiving strain and difficulty managing RRBs in parents of autistic children (Gabriels et al., 2005; Lecavalier et al., 2006; Bishop et al., 2007; Nikmat et al., 2008). Similarly, challenges with adaptive functioning skills can greatly impact a child’s level of independence (Harrop et al., 2016) which, in turn, places greater caregiving burden on parents. One study reported that increased caregiving strain was associated with lower levels of child adaptive functioning, specifically in the domain of daily living skills (Postorino et al., 2019). While the current study did not examine the individual subscale scores for the RBS-R and VABS-3 due to methodological concerns (see methods for details), future research is needed to better understand how specific aspects of RRBs and adaptive functioning abilities uniquely contribute to parents’ mental health and wellbeing. Altogether, our findings are consistent with the extant literature regarding the relationship between children’s RRBs, adaptive functioning abilities and caregiving strain.
The current study did not find a significant association between children’s behaviors and caregiving strain. Initially, this lack of association appears at odds with previous studies that have shown that children’s behaviors and autism symptomatology are associated with caregiving strain in parents of autistic children (Davis and Carter., 2008; Lecavalier et al., 2006). However, the current study differs from previous studies by analyzing children’s RRBs alongside children’s behaviors as a predictor of caregiving strain. It is possible that the inclusion of children’s RRBs accounted for variance accounted for by children’s behaviors in previous studies. Therefore, there is a need to better understand the ways different categories of behaviors may influence caregiver strain and, specifically, how autistic children’s RRBs may be perceived as behavioral concerns by caregivers. The use of parent-report measures of child factors in this study may have also contributed to differences in associations between children’s behaviors and parents’ caregiver strain. Future studies would benefit from the inclusion of observational measures of children’s behaviors, alongside caregiver report measures, to offer multiple vantages of children’s behaviors. Such an approach would allow for a more detailed understanding of the specific behaviors which appear to impact caregiver strain. Additionally, physiological measures of stress (such as heart rate variability), have been found to provide a more objective method for studying individual differences and underlying biological influences in stress reactivity and ER (Factor et al., 2017). This would inform possible supports to help families address these challenges.
In the current study, child factors were significantly associated with parents’ caregiver strain, even after the inclusion of parents’ ER in the model. This finding is consistent with previous studies in which child-related factors have been consistently associated with caregiver strain in parents of autistic children (Gabriels et al., 2005; Lecavalier et al., 2006; Bishop et al., 2007; Falk et al., 2014). Child factors, specifically children’s RRBs, were also associated with parents’ anxiety, depression and wellbeing, but these findings were no longer significant upon the inclusion of parents’ ER in the models. Although the present findings differ from previous studies that found a positive relationship between child factors and parents’ mental health and wellbeing (Hastings et al., 2005; Ozturk et al., 2014; Foody et al., 2015; Cohrs and Leslie, 2017; Li et al., 2022) they are consistent with other studies findings that parent-related factors (e.g., increased social support, parent cognition, parents’ internal locus of control) have been largely associated with positive mental health in parents of autistic children (Bishop et al., 2007; Falk et al., 2014; Bitsika and Sharpley, 2016). This difference may be in part due to the distinction between caregiving strain and mental health. Caregiving strain, as measured by the CGSQ-SF, refers to “the demands, responsibilities, difficulties” (Brannan et al., 1997) of caregiving for an autistic child. As such, this measure reflects the amount of daily strain experienced by parents, which may be more related to child-level factors such as adaptive functioning and behavioral concerns. In contrast, parents’ mental health refers to a more global experience of psychological distress, such as the experience of symptoms of anxiety and depression, which may be more related to parent-related factors such as parental cognition. Altogether, our findings underscore the need to consider both child- and parent- level factors in examining contributors to mental health and wellbeing in parents of autistic children.
The ability to regulate emotions also emerged as a significant factor in determining parents’ reports of caregiving strain and mental health. In fact, parents’ ability to regulate emotions was the only factor to predict all the parental outcomes - caregiver strain, depression, anxiety, and wellbeing. Additionally, parents’ ER abilities moderated the impact of children’s RRBs and adaptive functioning challenges on caregiving strain. Although the role of ER has not been specifically studied in parents of autistic children, it has been indirectly addressed in the literature within the related construct of parents’ coping skills (i.e., the behavioral and cognitive efforts employed to reduce distress; Lazarus and Folkman, 1984). From a theoretical perspective, ER and coping strategies both refer to processes aimed at fostering positive emotional states and regulating negative ones (Gross, 2002, 2015). The findings of the current study corroborate previous studies emphasizing the importance of positive coping strategies that address emotion dysregulation, such as cognitive reappraisal or reframing, for reducing stress and psychological distress in parents of autistic children (Hastings et al., 2005; Zablotsky et al., 2013; Shepherd et al., 2018). Conversely, certain coping strategies, such as avoidance or escape behaviors, have been associated with higher levels of stress (Dunn et al., 2001; Hastings et al., 2005). Our findings contribute to the extant literature by examining parents’ overall ability to regulate emotions, as opposed to the utility of specific coping strategies, in relation to the experience of caregiver strain and mental health and wellbeing. Our findings highlight the impact of ER abilities on the experience of caregiver strain and mental health in parents of autistic children and identify parents’ ER abilities as a possible intervention target. The importance of parent ER underscored in the present study also suggests that more environmental supports for parents of autistic children may be critical to providing space and time for parents to regulate complex emotions.
Lastly, a significant difference was seen in the experience of caregiving strain and anxiety reported by mothers and fathers, such that mothers reported higher levels of caregiving strain and anxiety than did fathers. These findings are consistent with previous studies reporting significantly higher levels of caregiver strain and anxiety for mother than fathers (Hastings, 2003; Dabrowska and Pisula, 2010; Foody et al., 2015; Vitale et al., 2022). One possible explanation for this discrepancy is that mothers tend to be more involved in the day-to-day management of family life (Konstantareas and Homaditis, 1992; Benson et al., 2008). In our sample, almost half of mothers identifying as stay-at-home caretakers in comparison to less than 5 percent of fathers. Research has found that greater involvement in managing children’s day-to-day activities is associated with higher levels of caregiver strain (Tehee et al., 2009), which may explain the higher incidence of caregiver strain in mothers. Differences have also been reported in the sources of caregiving strain for parents of autistic children, with mothers’ caregiver strain being predicted by daily living skills (e.g., sleeping, eating) and dysregulation, whereas externalizing behaviors have been found to predict fathers’ caregiver strain (Davis and Carter., 2008). These differences may have contributed to the sex differences seen for caregiving strain and anxiety. In sum, these findings contribute to the extant literature by replicating previous findings in a large sample. Further examination is needed to better understand the child and parent factors that contribute to different experiences of caregiver strain and anxiety in mothers and fathers of autistic children.
Future directions and limitationsThe current study presents findings from a large, national sample of autistic children and their biological parents. These findings are the first to shed light on the importance of ER on the experience of caregiver strain and adverse mental health in parents of autistic children. Despite the considerable strengths of this study, some limitations should be addressed. First, the sample included in this study was majority married, White, with a high SES, which affects the generalizability of the findings. Similarly, parents in this study were in heterosexual relationships, with almost half of mothers identifying as full-time care providers, which affects the generalizability of these findings to other family structures. Additionally, findings are based solely on parent-reports of their own caregiver strain, mental health, and ER, as well as their children’s autism symptomatology, adaptive functioning, and behaviors. Future research should consider other methods of measurement (e.g., direct observation, clinical assessment) when assessing the associations between these constructs. For example, studies examining the association between caregiver strain and children’s RRBs could benefit from the use of observational measures such as the ADOS-2 (Lord et al., 1999), the gold standard for autism diagnosis. Further, future research would benefit from the inclusion of a measure of social communication abilities in autistic children, to further parse the contribution of each core feature of autism. Lastly, while this study begins to examine the ways that ER abilities impact caregiver strain and mental health in parents of autistic children, this area of study is new and further examination is warranted.
ConclusionThis study is the first to examine how parents’ ER abilities moderate the association between children’s behaviors and parents’ experience of caregiving strain and mental health. Our findings suggest that parents may benefit from supports to improve their ER abilities and environmental supports to provide parents time and space for emotion management, which could improve their ability to cope with day-to-day stressors associated with caregiving for an autistic child.
Data availability statementThe original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statementThe studies involving human participants were reviewed and approved by the UCLA IRB Board. The patients/participants provided their written informed consent to participate in this study.
Author contributionsAD, RF, AS, LV, AW, LA, and AG conceptualized the study. ST and MP conducted the data analysis. AD and RF wrote the manuscript. All authors read and provided feedback on the final manuscript.
FundingThis work was supported through grants from SFARI (390314, AG) and the National Institutes of Health, National Center for Advancing Translational Sciences (UL1 TR001860).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnbeh.2023.1102516/full#supplementary-material
Footnotes ReferencesAbbeduto, L., Seltzer, M. M., Shattuck, P., Krauss, M. W., Orsmond, G., and Murphy, M. M. (2004). Psychological well-being and coping in mothers of youths with autism, down syndrome, orfragile X syndrome. Am. J. Ment. Retard. 109, 237–254. doi: 10.1352/0895-8017(2004)109<237:PWACIM>2.0.CO;2
CrossRef Full Text | Google Scholar
Achenbach, T. M., and Rescorla, L. A. (2001). Manual for ASEBA school-age forms & profiles. Burlington, VT: University of Vermont.
Anuradha, K. (2004). Empowering families with mentally Ill members: A strengths perspective. Int. J. Adv. Couns. 26, 383–391. doi: 10.1007/s10447-004-0174-x
CrossRef Full Text | Google Scholar
Baker, J. K., Messinger, D. S., Lyons, K. K., and Grantz, C. J. (2010). A pilot study of maternal sensitivity in the context of emergent autism. J. Autism Dev. Disord. 40, 988–999. doi: 10.1007/s10803-010-0948-4
PubMed Abstract | CrossRef Full Text | Google Scholar
Barakat, L. P., and Linney, J. A. (1992). Children with physical handicaps and their mothers: The interrelation of social support, maternal adjustment, and child adjustment. J. Pediatr. Psychol. 17, 725–739. doi: 10.1093/jpepsy/17.6.725
PubMed Abstract | CrossRef Full Text | Google Scholar
Barkley, R. A. (2011b). Barkley Deficits in Executive Functioning Scale (BDEFS for adults). New York, NY: Guilford Press. doi: 10.1037/t37378-000
CrossRef Full Text | Google Scholar
Bayley, N. (2006). Bayley scales of infant and toddler development. San Antonio, TX: Harcourt Assessment.
Bendixen, R. M., Elder, J. H., Donaldson, S., Kairalla, J. A., Valcante, G., and Ferdig, R. E. (2011). Effects of a father-based in-home intervention on perceived stress and family dynamics in parents of children with autism. Am. J. Occup. Ther. 65, 679–687. doi: 10.5014/ajot.2011.001271
PubMed Abstract | CrossRef Full Text | Google Scholar
Benson, P. R., and Karlof, K. L. (2009). Anger, stress proliferation, and depressed mood among parents of children with ASD: A longitudinal replication. J. Autism Dev. Disord. 39, 350–362. doi: 10.1007/s10803-008-0632-0
PubMed Abstract | CrossRef Full Text | Google Scholar
Benson, P., Karlof, K. L., and Siperstein, G. N. (2008). Maternal involvement in the education of young children with autism spectrum disorders. Autism 12, 47–63. doi: 10.1177/1362361307085269
PubMed Abstract | CrossRef Full Text | Google Scholar
Bishop, S. L., Richler, J., Cain, A. C., and Lord, C. (2007). Predictors of perceived negative impact in mothers of children with autism spectrum disorder. Am. J. Ment. Retard. 112, 450–461. doi: 10.1352/0895-8017(2007)112[450:POPNII]2.0.CO;2
CrossRef Full Text | Google Scholar
Bitsika, V., and Sharpley, C. F. (2016). Which aspects of challenging behaviour are associated with anxiety across two age groups of young males with an autism spectrum disorder? J. Dev. Phys. Disabil. 28, 685–701. doi: 10.1007/s10882-016-9502-4
CrossRef Full Text | Google Scholar
Bodfish, J. W., Symons, F. J., and Lewis, M. H. (1999). The Repetitive Behavior Scales (RBS). Research Reports. Chapel Hill, NC: Western Carolina Center.
Brannan, A. M., Athay, M. M., and de Andrade, A. R. V. (2012). Measurement quality of the caregiver strain questionnaire-short form 7 (CGSQ-SF7). Adm. Policy Ment. Health Ment. Health Serv. Res. 39, 51–59. doi: 10.1007/s10488-012-0412-1
PubMed Abstract | CrossRef Full Text | Google Scholar
Brannan, A. M., Heflinger, C. A., and Bickman, L. (1997). The caregiver strain questionnaire: Measuring the impact on the family of living with a child with serious emotional disturbance. J. Emot. Behav. Disord. 5, 212–222. doi: 10.1177/106342669700500404
CrossRef Full Text | Google Scholar
Bristol, M., Gallagher, J., and Schopler, E. (1988). Mothers and fathers of young developmentally disabled and nondisabled boys: Adaptation and spousal support. Dev. Psychol. 24, 441–451. doi: 10.1037/0012-1649.24.3.441
CrossRef Full Text | Google Scholar
Bury, S. M., Jellett, R., Spoor, J. R., and Hedley, D. (2020). “It defines who I am” or “It’s something I have”: What language do [autistic] Australian adults [on the autism spectrum] prefer? J. Autism Dev. Disord. 53, 677–687. doi: 10.1007/s10803-020-04425-3
PubMed Abstract | CrossRef Full Text | Google Scholar
Clarke, P. J., Marshall, V. W., Ryff, C. D., and Wheaton, B. (2001). Measuring psychological well-being in the Canadian study of health and aging. Int. Psychogeriatr. 13, 79–90. doi: 10.1017/S1041610202008013
PubMed Abstract | CrossRef Full Text | Google Scholar
Cohrs, A. C., and Leslie, D. L. (2017). Depression in parents of children diagnosed with autism spectrum disorder: A claims-based analysis. J. Autism Dev. Disord. 47, 1416–1422. doi: 10.1007/s10803-017-3063-y
PubMed Abstract | CrossRef Full Text | Google Scholar
Dabrowska, A., and Pisula, E. (2010). Parenting stress and coping styles in mothers and fathers of pre-school children with autism and Down syndrome. J. Intell. Disabil. Res. 54, 266–280. doi: 10.1111/j.1365-2788.2010.01258.x
PubMed Abstract | CrossRef Full Text | Google Scholar
Davis, N. O., and Carter, A. S. (2008). Parenting stress in mothers and fathers of toddlers with aut
留言 (0)