Data and Population
We analyzed the 2019 and 2020 National Health Interview Survey (NHIS), conducted annually by the National Center for Health Statistics (NCHS). The NHIS is a cross-sectional, nationally representative, household-based survey of the civilian, non-institutionalized population, typically conducted face-to-face in participants’ homes and by telephone. For each household surveyed, basic demographic data are gathered about all individuals and then one “sample adult” is selected at random and asked a more extensive list of questions. NHIS uses a multistage sampling approach by selecting households in nested, geographically defined strata and clusters.20
The 2019 sample adult response rate was 59.1%.21 During 2020, the COVID-19 pandemic necessitated a shift from in-person to telephone-based interviewing and response rates dropped. To account for the decreased response rates seen in 2020, NHIS re-contacted a group of survey respondents from 2019 and created a longitudinal 2019–2020 sample to bolster the original 2020 “partial sample.”20 Following NHIS recommendations, we excluded the 2020 longitudinal sample to analyze 2019–2020 as a single combined national data set with no repeated interviews.20
Our study population included female “sample adults” ages 18 to 49 years of age. Of note, our primary exposure (giving birth in the last year), discussed below, was only ascertained by the NHIS among individuals in this subgroup; i.e., it excluded older adults and those who did not self-report female gender, precluding inclusion of postpartum individuals of other genders in our study. For this paper, we use the term “women,” as utilized in the NHIS survey; however, we want to acknowledge that not all individuals who birth identify as women. Additionally, our data addressed live births only.
Study Outcomes
The primary exposure of interest was whether our study subjects gave birth in the past year, ascertained with the question: “During the past 12 months, did you have a pregnancy that ended in a live birth?”
We had two outcomes of interest: (1) problems with medical debt, and (2) inability to pay medical debt. The first was ascertained with the question, “In the past 12 months did you / anyone in the family have problems paying or were unable to pay any medical bills?” The second was ascertained with the question, “Do you / does anyone in your family currently have any medical bills that you are unable to pay at all?” The second question was only asked of those who had problems with medical debt (or who did not answer that question), although we constructed our outcome using the full study population denominator.
Analysis Plan
We first tabulated the characteristics of the study population and compared baseline characteristics stratified by the exposure of birth status (gave birth in last year or not).
Next, we tabulated the proportion of individuals having each outcome stratified by birth status. We calculated unadjusted odds ratio examining the association between birth status and each debt outcome using univariate logistic regressions. We then performed multivariable logistic regression with adjustment for the following: age (ages 18–24; 25–34; 35–49), region (Northeast, Midwest, South, West), self-reported health status (good/very good health; fair/poor health), education (< high school, high school/GED, some college, BA, > BA), family income ($0 to $34,999; $35,000 to $49,999; $50,000 to $74,999; $75,000 to $99,999; $100,000 or greater), and marital status (married vs. unmarried [includes widowed, divorced, separated, never married, living with a partner but not married]). We repeated these analyses restricted to the subgroup of women with private health insurance, which might offer greater protection against healthcare cost burdens.
Next, within the subgroup of women who had a live birth in the past year, we examined correlates between three sociodemographic characteristics (income, race/ethnicity, and insurance) and three chronic diseases common among pregnant women (asthma, hypertension, and gestational diabetes)22,23 with each medical debt outcome. Multivariable models included adjustment for the covariates used in our aforementioned multivariable models in addition to health insurance (private; Medicaid and other public; other coverage; or uninsured) and one chronic disease indicator (however, all three chronic indicators were included in models examining the association between sociodemographic variables and debt outcomes). Additionally, for a supplementary analysis, to examine whether insurance status or chronic diseases modified the effect of live birth on debt outcomes, we examined the full study cohort and interacted insurance status (or one of the chronic disease indicators) with the live birth indicator; these models included covariates used in the other multivariable models as well as main effects.
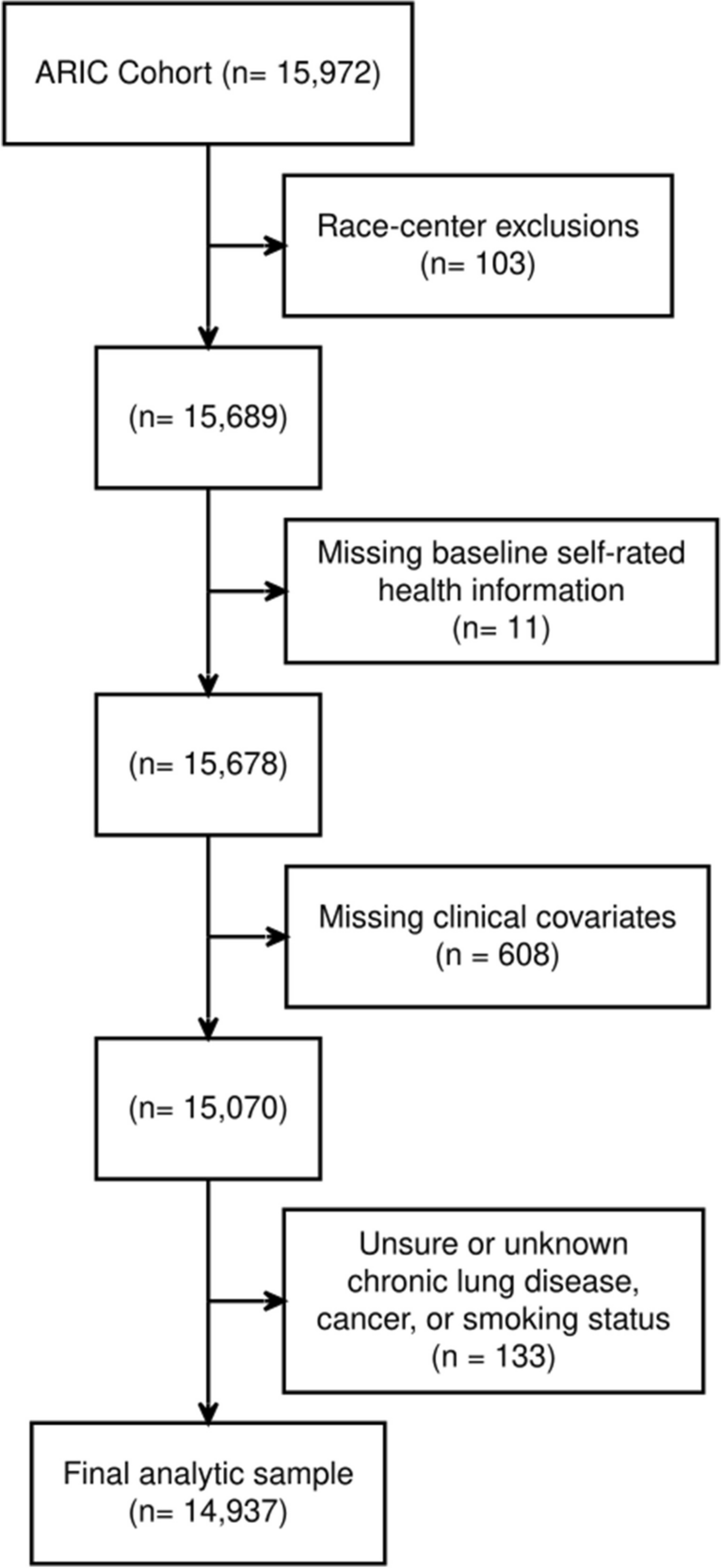
Of our total study population of n = 12,163, 2.6% (n = 321) had missing data on one or more covariate, and were excluded from complete case adjusted analyses (Appendix Fig. 1).
We used Stata/SE 16.1 (StataCorp LLC) for all analyses. Using the Stata svy procedure and NCHS weights, primary sampling units, and strata, we calculated nationally representative estimates that accounted for the NHIS’s complex design. We used Stata’s margins commands after models including interaction terms to calculate predicted probabilities and statistical significance of potential effect modification. Our study was deemed exempt from review by the Cambridge Health Alliance Institutional Review Board.





留言 (0)