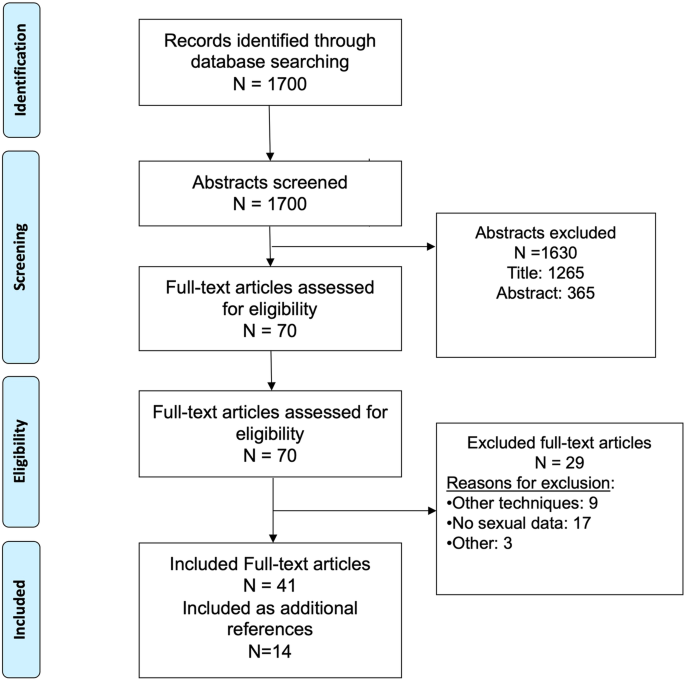
The search generated 657 citations between the dates of January 1, 2007 to May 30, 2022. 102 duplicates were removed. The remaining 555 were imported into Covidence for title and abstract screening. 482 studies were excluded, leaving 73 studies for full text screening. Database alerts, collected between May 31, 2022 and August 5, 2022, generated three further guidelines for inclusion, bringing the total for full text screening to 76. After applying the PCC inclusion criteria to the full text screening, 23 guidelines and consensus statements from 16 different groups or organisations remained (Fig. 1).
Research questions
A narrative summary, addressing each of the research questions in turn, accompanies the genetic testing strategies from each of the 23 included guidelines and consensus statements. Guidelines and consensus statements included in Table 3 were genetic testing guidelines or consensus statements from major organisations, recognised as authorities on the subject (n = 13). Major guidelines are thus defined as guidelines or consensus statements based on a clearly articulated process involving research evidence to support recommendations with consensus from a panel of experts from recognised medical organisations (national, or regional). The 10 remaining guidelines or consensus statements, are referred to as adapted guidelines, based on reviews of the major guidelines and consensus statements with country-specific, or other considered modifications based on specific stages of cancer, implementation, or practical clinical application. All adapted guidelines are also based on a rigorous methodology and consensus from a panel of experts. A summary table of these adapted guidelines is in Appendix III.
a. What genetic testing guidelines and consensus statements for prostate cancer currently exist?
Of the 13 major guidelines included in this review, six guidelines and two consensus statements were from organisations in the US, comprising the NCCN (n = 3) [21, 30, 31], a conglomerate of specialist prostate cancer clinician organisations (AUA; American Society for Radiotherapy and Oncology (ASTRO); Society of Urologic Oncology (SUO)) (n = 3) [32,33,34] and the Philadelphia Prostate Cancer Consensus Conference (n = 2) [16, 35]. Two guidelines and two consensus statements were from European organisations: ESMO; [23] a conglomerate of organisations comprising specialist prostate cancer clinicians (European Association of Urology (EAU), European Association of Nuclear Medicine (EANM), European Society for Radiotherapy and Oncology (ESTRO), European Society of Urogenital Radiology (ESUR), International Society of Geriatric Oncology (SIOG)) [22]; and the Advanced Prostate Cancer Society (APCCC) (n = 2) [36, 37]. One major guideline, eviQ, was from the Cancer Institute of NSW, Australia [38].
The ten remaining adapted guidelines comprised seven guidelines, two consensus statements and one position paper from various organisations in nine countries including Italy (Italian Scientific Societies) [39], France (Cancer Committee of the French Association of Urology (CCFAU)) [40], Spain (Spanish Society of Medical Oncology (SEOM) and Spanish Oncology Genitourinary Group (SOGUG)) [41], Canada (n = 2) (i. Canadian Consensus Forum [42] and ii. Canadian Expert Multidisciplinary Working Group in Genetic Testing for Metastatic Prostate Cancer [43]), Switzerland (Swiss Group for Clinical Cancer Research (SAKK) Network for Cancer Predisposition Testing and Counselling (CPTC)) [44], US (Large Urology Group Practice Association (LUGPA)) [45], Sweden (n = 2)(Swedish National Prostate Cancer Guidelines Group) [46, 47] and China (Hong Kong Urological Association and Hong Kong Society of Uro-Oncology) [48].
b. What are the recommendations for genetic testing of prostate cancer?
Genetic testing strategies from each of the major guidelines are summarised in Table 3. Genetic testing strategies from adapted guidelines are summarised in Appendix III.
c. Who should be considered for genetic testing?
All guidelines and consensus statements recommend genetic testing (germline and/or somatic) for men with metastatic prostate cancer. The NCCN guidelines offer the most detailed guidance across the three prostate cancer relevant guidelines included (Prostate Cancer; Genetic/Familial High-Risk Assessment: Breast, Ovarian and Pancreatic Cancer; and Colon Cancer). Essentially, germline testing is recommended for men with high- or very high-risk prostate cancer, regional or metastatic prostate cancer, regardless of family history. Germline testing is also recommended for men with a personal history of breast cancer or a positive family history of early onset breast, colorectal or endometrial cancer (age ≤50 years); ovarian, exocrine or pancreatic cancer (any age); prostate cancer ≤60 years or prostate cancer death; Lynch-syndrome related cancer, especially if diagnosed <50 years; or Ashkenazi Jewish ancestry.
Somatic testing is recommended for men with hormone sensitive metastatic prostate cancer or castrate resistant metastatic prostate cancer. While many of the major guidelines offer less specific and/or less comprehensive criteria for genetic testing than NCCN, all recommend germline and somatic testing for men with metastatic prostate cancer, particularly for men with personal or family history or Ashkenazi Jewish ancestry and early onset disease.
For men with early stage or localised prostate cancer, germline genetic testing is recommended only where it is likely to impact treatment, clinical trial options, risk management of other cancers and/or potential risk for family members. Testing criteria tend to focus on personal history of metastatic or high-risk prostate cancer, particularly early onset, and family history of prostate cancer, breast, ovarian, pancreatic, colorectal or endometrial cancer and Ashkenazi Jewish ancestry. Some guidelines [23, 38] recommend germline testing for men who have confirmed DNA MMR deficiency or a pathogenic variant in a listed gene after tumour testing. For this population, one guideline makes no recommendations [34], while others suggest genetic testing be considered only for men with personal or family history of high-risk germline mutations and/or early onset prostate cancer [44, 46, 48].
For men without prostate cancer, many guidelines make no mention of genetic testing [23, 34, 40] or make recommendations to consider germline testing for reasons of family history or ancestry [22, 38, 48], rather than recommending it. Germline testing is recommended for men without prostate cancer in the guidelines of only three organisations. NCCN recommend germline testing for men with a family history suggestive of hereditary prostate cancer or hereditary breast and ovarian cancer or colon cancer syndromes [21, 30, 31]. The Italian Scientific Societies recommend germline BRCA testing for men with a family history of hereditary breast or ovarian cancer or paternal family with breast or ovarian cancer [39]. The Spanish Society of Medical Oncology recommends germline testing for men with a family history of cancer predisposition [41].
d. Which genes should be tested for?
Men with prostate cancer may have germline mutations in a number of genes. Those genes with moderate to high risk hereditary cancer susceptibility include homologous recombination repair genes BRCA2, BRCA1, CHEK2, ATM, PALB2, RAD51D; mismatch repair genes MLH1, MSH2, MSH6, PMS2; and pathogenic variant HOXB13. These genes are implicated in a range of cancer types, with the exception of HOXB13 which, to date, seems to be prostate cancer specific [12]. The NCCN provides the most comprehensive recommendations, recommending different genes for genetic testing based on the purpose of testing (Table 4) [21].
Table 4 Purpose of genetic testing and choice of genes.Other guidelines base their recommendations on disease stage [22, 32,33,34,35] or a combination of both purpose and stage. While there is some consensus regarding which genes to test, recommendations across guidelines vary. For example, for metastatic castrate resistant prostate cancer, recommendations range from the type of test (germline and/or somatic) with no specific genes nominated [42, 47] or testing for one gene only (BRCA2) [47] compared to the more comprehensive list recommended by NCCN in Table 4 above. For those with high-risk or metastatic prostate cancer, one guideline recommends germline testing only after somatic testing or after a validated prediction tool (e.g., CanRisk) confirms a ≥ 10% probability of detecting BRCA1/2 pathogenic variant [38], whereas many guidelines and consensus statements recommend germline testing across a range of genes for all men diagnosed with metastatic prostate cancer [16, 21,22,23, 30,31,32,33,34,35,36,37, 41, 43, 45, 48].
e. Which testing methods are used and where are samples drawn from?
Few guidelines or consensus statements provide further specificity than germline and/or somatic testing in relation to testing methods or where samples are drawn from. Recommendations tend to range from targeted gene tests for one or two genes (BRCA1/2) to a prespecified gene panel (e.g. HRR and/or MMR genes) [16, 21, 30, 31, 35, 45], or large panel testing for advanced prostate cancer [36, 37]. Whole exome or whole genome sequencing was not mentioned in any of the included guidelines or consensus statements. Typically, germline testing samples blood or saliva and somatic testing samples the tumour or metastatic tissue. No guideline or consensus statement mentioned sampling plasma or testing for circulating tumour DNA. Putative mutations or variants of unknown significance (VUS) were mentioned only in relation to post-test counselling [16, 21, 30, 31, 35,36,37].
f. What evidence supports the recommendations?
All guidelines and consensus statements involved a review of the literature as an evidence base. While guidelines and consensus statements often employed different methods to rate the level of evidence or strength of recommendation to support their recommendations, in general, evidence was reported as lower level. For example, all included NCCN recommendations were rated 2a, meaning the guideline statement is based upon lower-level evidence, however, NCCN consensus is that the intervention is appropriate. Expert opinion, which comprised reviews of the literature and consensus panels, was cited as strength of recommendation in 10 guidelines [16, 32,33,34,35,36,37,38,39, 42,43,44,45,46,47]. Other guidelines and consensus statements used modified GRADE evidence ratings [22, 40, 48] had their own strength of evidence ratings [32,33,34] or grades of recommendation [23] or adopted other systems from previous clinical guidelines [41] to rate the strength of their recommendations.

留言 (0)