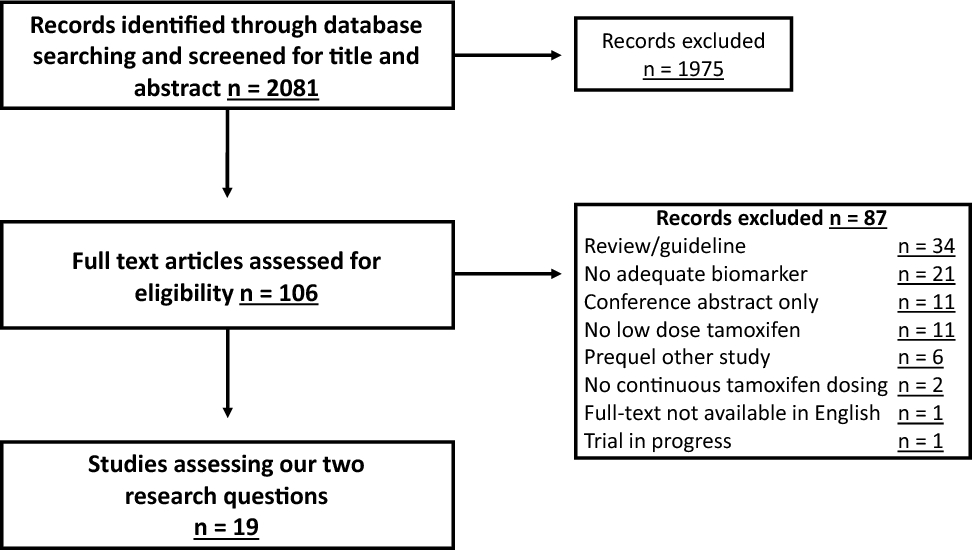
In this paper, we have mapped the landscape of expanded access publications from January 1, 2000 to January 1, 2022. To the best of our knowledge, this is the first literature review of expanded access publications to assess drugs, diseases, patient numbers, and research methods. We have identified 1632 original investigations of expanded access, of which 1231 focus on pharmacological therapeutics, and the number of publications increases significantly over time. The increase in publications reflects a general increase in attention for expanded access, as reported by regulators, industry, and through other scholars. Our work provides the first annotated dataset that yields insights into how many patients contributed to the peer-reviewed scientific literature through expanded access programs, across diseases, geographies, and drugs.
The geographic distribution of expanded access publications highlights the disparity in the availability of investigational medicine. High-income countries produce more publications compared with low-income countries, which may be partly explained by excluding non-English literature, but may also be attributed to manufacturer and scientific willingness to provide expanded access and facilitate subsequent research. Our findings reflect the limited access to medicine in developing countries in general, but to investigational medicine in particular—an issue worth exploring in future research.
The differences between countries within the EU may be due to differences in regulatory preferences. Italy, with the highest number of publications per capita, is more liberal in allowing data collection compared with countries such as Sweden and Finland [3]. The variance in allowing expanded access programs to generate evidence among European regulators has created a maze of national pathways for manufacturers to navigate [7]. Such complexity may provoke reluctance from drug manufacturers to provide expanded access in the first place, which may impede rather than facilitate equity in patient access.
The largest share of expanded access research is devoted to oncology and (malignant) hematology, accounting for 53.5% publications. This is driven in part by the large unmet medical need of cancer patients, as well as the abundance of trials in these areas. Furthermore, regulators offer specific guidance for expanded access to oncology (for example, through the FDA’s Project Facilitate) [25], educating oncologists and expediting access to anticancer drugs.
Our findings seem to support the position that, indeed, expanded access programs can be used to collect data that can further the knowledge on an investigational medicine. The stance of some regulators (e.g., Sweden, Finland, Canada) that data collection within an EAP is prohibited (or discouraged), in part over fears of data quality or companies attempting to bypass trial regulations [3, 26, 27], seems to be at odds with the numbers of publications from those countries (n = 13, n = 5, n = 56, respectively). The number of expanded access publications show that the treatment of patients with investigational medicine is, in itself, being used as a means to support (ongoing) investigations.
Nonetheless, the analyses of expanded access data should be interpreted with caution. Expanded access data are nonblinded, nonrandomized data, and as such may be inherently confounded. These “real-world” data may harbor serious data quality issues. Furthermore, expanded access data may suffer even more quality loss, as 50.9 % of the reports in our sample collected data retrospectively. This may severely impact data quality, although main parameters (such as survival) should be straightforward to gather. In our analysis of endpoints used in EAPs for COVID-19, we found that data is collected beyond mandatory safety reporting. Endpoints included various clinical improvement ratings/scales, respiratory or oxygen support status, duration of hospitalization, viral load, and patient-reported outcomes, among others. The heterogeneity of research methods and endpoints makes it difficult to compare studies.
Ideally, an EAP should include a prespecified, prospective data collection to ensure highest data quality that is fit for purpose. Although the inclusion of expanded access data (and other sources of real-world data) in regulatory decision-making is increasing [8, 28, 29], the lack of oversight could contribute to suboptimal data quality and hesitance of regulatory bodies to include said data in decision-making processes. To expand the application of expanded access data beyond peer-reviewed publications, it is important to develop minimal data quality standards for expanded access studies in the future [30].
Harmonization on publications may be an area of potential development. Some expanded access programs harbor “salami tactics,” i.e., there are different publications per center, then per region, then per country, and subsequently, a synthesized international publication [16,17,18,19,20]. Additionally, the basis of a new publication may not be a different geographic location, but rather a different (sub)topic, publishing separately on safety [21], efficacy, and/or quality-of-life [22]. Although we acknowledge that the lack of observational research harmonization across countries impedes international collaboration, we question the incremental added value of each of these single publications as opposed to several large, overarching, international publications. As local investigators may not be aware of all scientific endeavors worldwide, drug manufacturers should better coordinate local efforts by connecting researchers across regions.
The impact of COVID-19 on the expanded access landscape is remarkable. Early in the pandemic, various authors cautioned against the widespread use of medication outside of clinical trials as randomized trials would be “the only way to find effective and safe treatments for COVID-19” [26]. Indeed, the results from the large-scale expanded access program of convalescent plasma in the USA later failed to replicate in various randomized trials [31,32,33,34]. Although we agree that the place for expanded access is in addition to clinical trials rather than instead of, there is a place for expanded access in facilitating serendipitous findings, especially in the field of rare diseases. Evidence of expanded access can be used in addition to clinical trials to explore the safety and effectiveness of medicines used in different populations, or in (slightly) different indications (for example, in the case of cancer therapies targeting the same genetic aberration in a different histology). The drawback of expanded access data collection does not imply that these data are worthless or that no data ought to be collected; we, together with other scholars [4, 6], believe that the treatment of a patient with investigational medicine should always be used to further the understanding of the potential benefits and risks of investigational medicine [30].

留言 (0)