
記住我

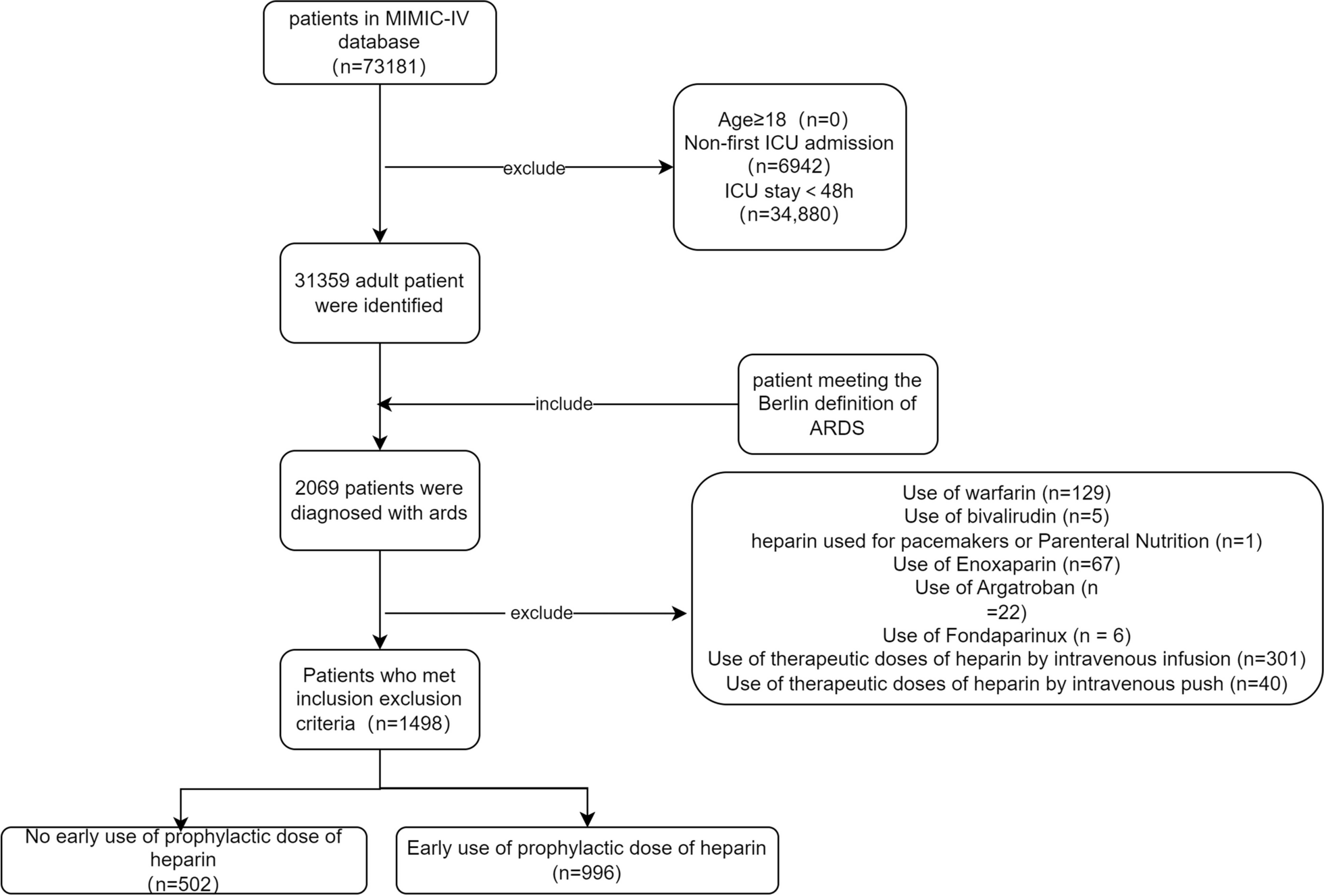
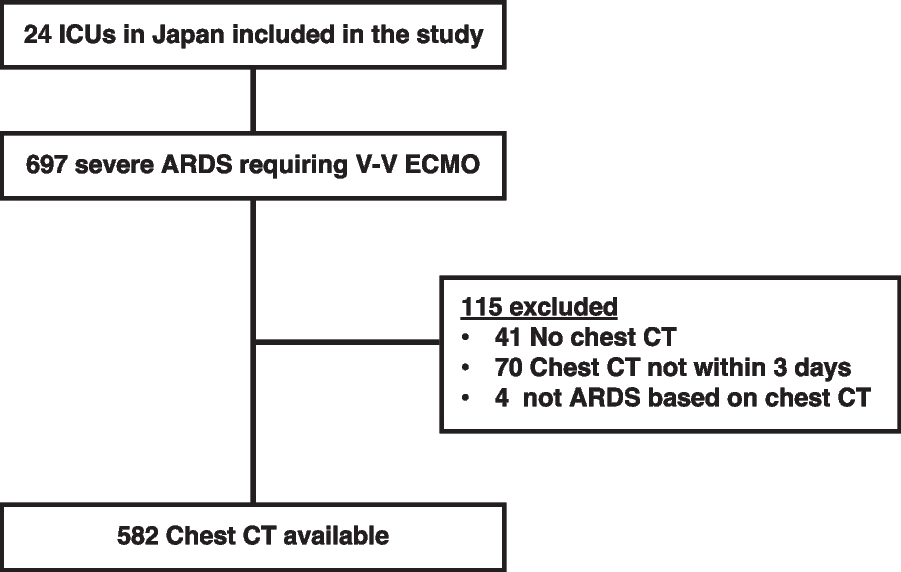
Enrolled in this study were 253 of the 435 consecutive adult patients (≥ 20 years old) who underwent cardiovascular surgery at the Wakayama Medical University Hospital between January 1st 2020 and December 31st 2021. Owing to the need for emergent surgery, 162 patients were excluded, and 20 patients were excluded because they were admitted to a department outside of ICU, such as to a cardiac care unit or general ward (Fig. 1).
Fig. 1 Ethical statement
Ethical statementThis single-center retrospective cohort study was approved by Wakayama Medical University Institutional Review Board (approval number 3532) and was registered in the UMIN Clinical Trial Registry on 23rd June, 2022 (registration no. UMIN000048142). The need for informed consent was waived because of the retrospective and observational nature of this study, but the study was conducted in accordance with the principles of the Declaration of Helsinki.
InterventionWe introduced a nurse-led preoperative orientation program as a preventative measure against delirium during postoperative ICU stays (Fig. 2). In this program, nurses specializing in ICU care visit the patients on the day before surgery. Initially, they introduce themselves and their work to the patients. Patients then receive orientation about the ICU environment which includes, for example, how to wake up from anesthesia in the ICU bed, the kinds of noises such as alarm sounds that they will hear in ICU, and about the medical staff members such as nurses and physicians that will be working around them during their stay there. The nurses then explain the procedures that patients will undergo (e.g. mechanical ventilation, central venous catheter, atrial catheter, chest drainage tube, etc.). The patient is informed that she/he cannot initially speak because of the use of tracheal tube, but they may communicate with nurses and physicians by gesture or writing. Patients are informed that they may be physically restrained. Finally, patients receive information about postoperative delirium (e.g. “what is delirium”, “what symptoms of delirium might patients have?”, or “what is the treatment for delirium?”) During this orientation visit, which takes approximately 30 min, nurses use a pamphlet including pictures and explanatory text. Wherever possible, nurses who will be responsible for providing care of the patient during their ICU stay participate in the preoperative orientation. This intervention, named ‘preoperative visit’, was transitionally introduced in October 2020 and then routinely performed from January 2021 (Fig. 3). The same preoperative orientations were used in the transitional period and post-intervention period.
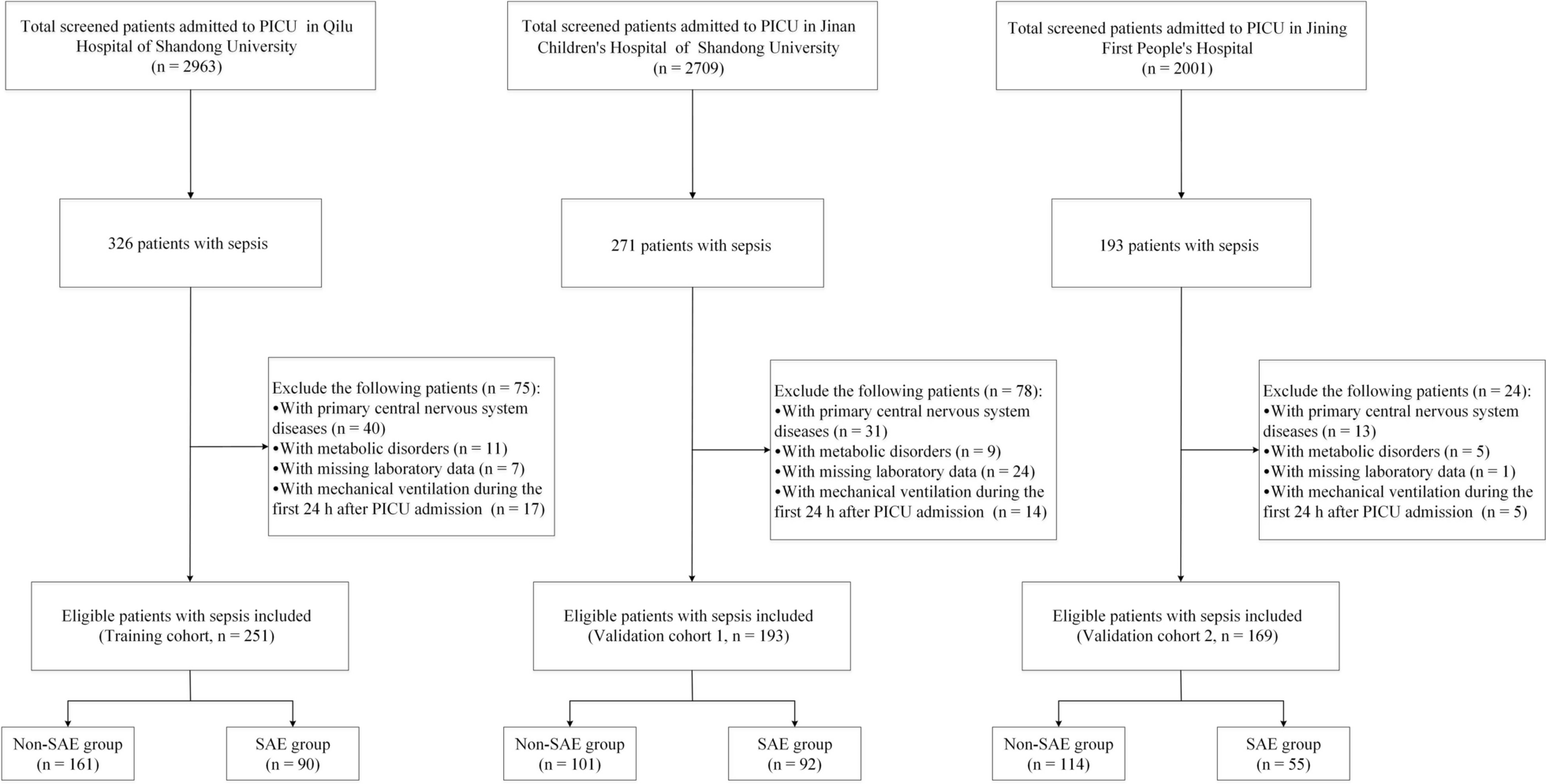
Fig. 2
Example of orientation with figure used in the nurse-led orientation program. ECG: electrocardiogram; SpO2: peripheral saturation of oxygen; CV: central venous
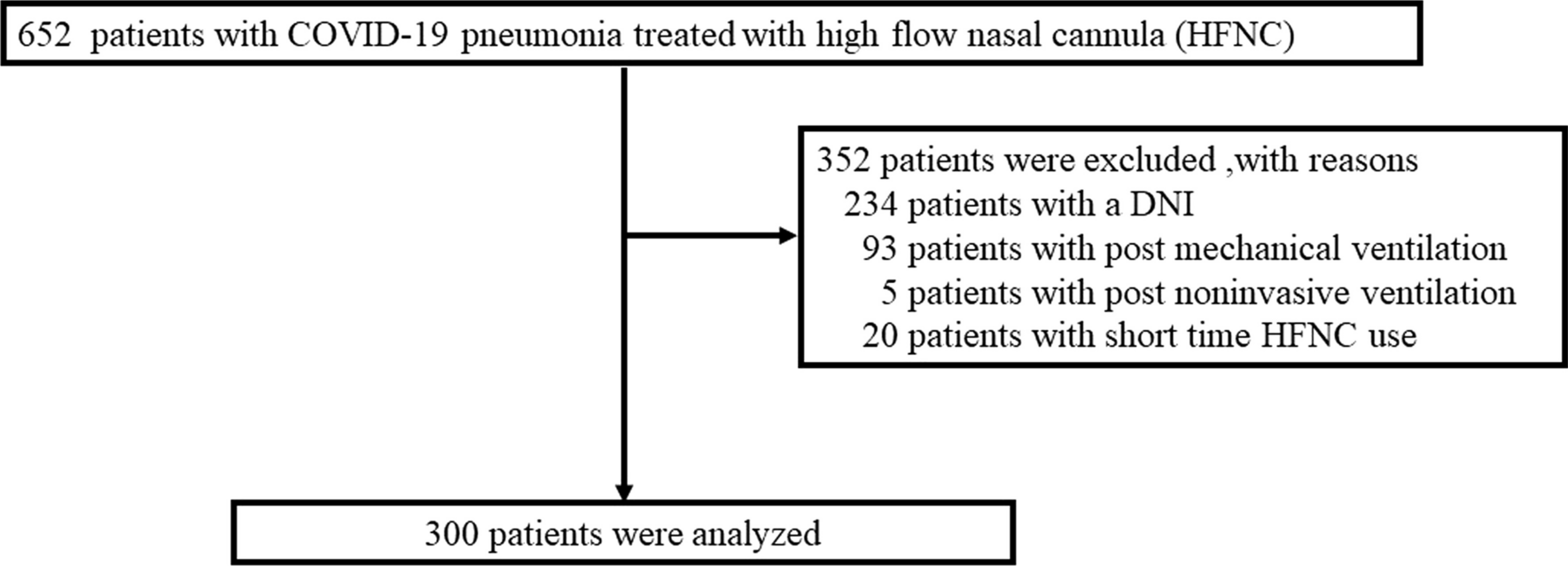
Fig. 3
Intervention period. A nurse-led preoperative educational program (preoperative visit) was gradually introduced from October 2020, and used routinely from January 2021
In some cases, the preoperative visit was not conducted during the transitional or the post-intervention period because the patients were not available at the time of orientation visit for other preoperative examinations, etc. The patients’ selection of the intervention was not based on their preoperative factors.
OutcomesThe primary outcome of this study was the occurrence of delirium, which was defined as at least one positive result on the Confusion Assessment Method for the ICU (CAM-ICU) during their ICU stay [12]. CAM-ICU was assessed daily by trained nurses during the daytime when patients were not under deep sedation, and there was also assessment of whether there was change in patients' mental status. Secondary outcomes included the length of ICU and hospital stay, hospital discharge to home, and medical costs during hospitalization.
Procedures during surgery and ICUIn the operating room, general anesthesia was performed with propofol, remifentanil, sevoflurane, or rocuronium at the discretion of the anesthesiologist at the time. Additional epidural anesthesia by levobupivacaine or fentanyl was used for patients who received thoracoabdominal incision. INVOS system (Covidien, Minneapolis, MN) was routinely used to measure the regional cerebral oxygen saturation (rScO2) at the left and right forehead during the operation to monitor the appropriate cerebral perfusion. The value used was the mean rScO2 of the left and right forehead.
In our ICU, we performed the standard preventive measure for delirium known as the ABCDEF bundle [13]. Analgosedation was performed using fentanyl, propofol, and/or dexmedetomidine for patients receiving mechanical ventilation. Dexmedetomidine was used at the discretion of the physician responsible for sedation during mechanical ventilation and prevention of postoperative delirium. All patients were routinely evaluated for pain using the numeric rating scale or behavioral pain scale, as appropriate. Fentanyl and intravenous acetaminophen were mainly used to alleviate pain towards the goal of behavioral pain scale < 5 or numeric rating scale < 4. All patients receiving mechanical ventilation routinely underwent daily spontaneous awakening trials and spontaneous breathing trials as a means of weaning them from mechanical ventilation when it was considered to be appropriate. Sedation depth was evaluated using the Richmond Agitation Sedation Scale every 1–3 h. The goal of sedation in patients during the spontaneous awakening trial was set to Richmond Agitation Sedation Scale of 0 or − 1 (calm) during the day and − 2 or − 3 (lightly sedated) during the night. We avoided using benzodiazepines, a known cause of delirium, and we evaluated the occurrence of delirium with CAM-ICU, mentioned in the outcome subsection below. We routinely performed early mobilization and rehabilitation after the surgery. Before the COVID-19 pandemic, family visitation was allowed in accordance with the requests of patients and their families.
Statistical analysisContinuous variables are presented as median and interquartile range (IQR) or average and standard deviation. Categorical variables are presented as numbers and percentages. To compare two groups, Student’s t test or Wilcoxon rank sum test were used for continuous variables, and Pearson’s chi-square test or Fisher’s exact test were used for categorical variables, as appropriate. Univariate and multivariate logistic regression models were used to assess the association between the preoperative orientation visits and delirium. The multivariate logistic model used predefined adjusters that were selected because previous literature and clinical judgement suggested they would be risk factors of postoperative delirium [1, 14]. These adjusters included age (≥ 75 years, median), history of cerebrovascular and mental illness (at least one of cerebrovascular disease, mental illness, history of delirium during previous hospitalization, and dementia), use of cardiopulmonary bypass (CPB), operation time, intubation time after surgery (≥ 14 h, median), and perioperative platelet cell transfusion received. As sensitivity analysis for primary results and as exploratory analysis to examine risk factors on postoperative delirium, we separately constructed univariate and multivariate logistic regression models using variables from baseline characteristics (age, gender, body mass index [BMI], left ventricular ejection fraction, chronic kidney disease (estimated glomerular filtration rate < 60 ml/min/1.73 m2), respiratory disorder (forced expiratory volume 1.0% < 70% and/or % vital capacity < 80% defined by spirometry), diabetes mellitus, history of smoking and any cerebrovascular or mental illness), the European System for Cardiac Operative Risk Evaluation II (EuroSCORE II), and characteristics during operation (type of surgery, operation time, CPB use, rScO2, any transfusion received, and highest plasma lactate level). The multivariate model used variables that were P value < 0.05 in the univariate model. Additionally, we conducted the abovementioned analyses but with exclusion of the transitional period for the purpose of more clearly understanding sensitivity, because this period had a mixture of patients that received preoperative visits and patients that did not.
JMP Pro software (version 16; SAS Institute, Cary, NC) was used in all analyses. A two-sided P value < 0.05 was considered to be statistically significant.
留言 (0)