
記住我




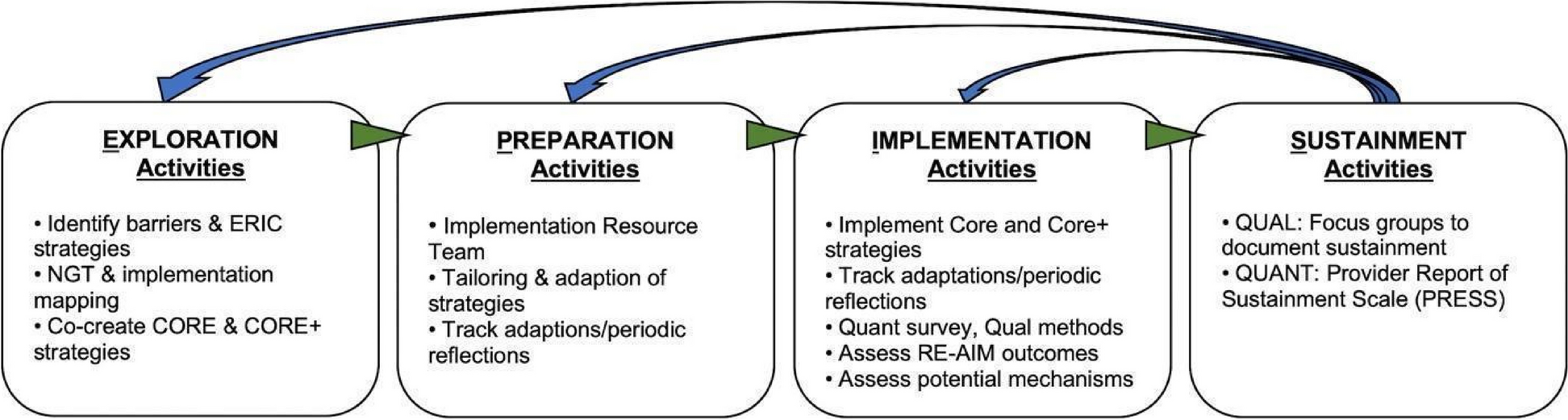

This study occurs in multiple phases [a pre-implementation (UG3), implementation (UH3), and post-implementation], applies several implementation science frameworks, and uses a stepped wedge cluster randomized trial (CRT) study design. Figure 1 overviews the two implementation science frameworks — the integrated Promoting Action on Research Implementation in Health Services (i-PARiHS) [26] and the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) [27] — used in the pre- and post-implementation phases. Below, we provide details on each phase.
Fig. 1
Overview of i-PARiHS and RE-AIM
The pre-implementation phase used the i-PARiHS in inquiring about the existing health system and PHC context to inform the development of a context-specific PF strategy. We assessed barriers and facilitators of integrating TASSH into PHCs for hypertension management through structured facility assessments and in-depth interviews with stakeholders within the PHCs and primary health system in Akwa Ibom. A pilot study was conducted during the pre-implementation phase wherein the feasibility of TASSH plus PF intervention was assessed in two PHCs. The facilities included in the pilot are not participating in the implementation phase.
In the implementation phase, we are using a SW-CRT design to introduce PF at the PHCs. The 30 PHCs were randomly allocated into five cohorts of six PHCs, and all begin in the TASSH only condition, which serves as the usual care control. Figure 2 overviews the stepped wedge design for this study. Given the SW-CRT, the length of time in TASSH alone (without PF) will vary, with a minimum duration of 3 months for the first cohort. Three months prior to the TASSH plus PF experimental condition starting, each cohort will have a training period. During this period, nurses and other staff at the PHCs receive training (or retraining) in delivering TASSH. Once the 3-month training period is completed, the PHCs will participate in a 12-month implementation period during which PF will occur.
Fig. 2
Stepped wedge study design
Nurses at these PHCs will implement all aspects of TASSH in their clinical care for PLWH with uncontrolled hypertension. PFs will support nurses during the 12-month period by helping with hypertension treatment issues and addressing barriers to TASSH implementation. The RE-AIM framework defines measures to evaluate the effect of PF on TASSH adoption after 12 months of PF compared to TASSH adoption without PF (primary outcome). RE-AIM facilitates evaluation of the effect of PF on BP control (secondary outcome) and the level of TASSH implementation fidelity (secondary outcome).
Following each cohort’s 12-month implementation phase, each PHC transitions to the post-implementation phase (follow-up period). Nurses will continue to implement TASSH. However, PF will end. Six months into this post-implementation period (18 months following the start of PF), we will evaluate the sustainability of TASSH within the PHCs (secondary outcome). Figure 3 provides an overview of the study design including the pre-implementation, implementation, and post-implementation phases.
Fig. 3
Pre-implementation (UG3), implementation (UH3), and post-implementation phases
Ethical approvalsThis study is approved by the Institutional Review Boards (IRBs) at the University of Abuja (Abuja, Nigeria), Ibom Multi-Specialty Hospital (Uyo, Akwa Ibom), and New York University (NYU) Grossman School of Medicine. The study is registered at Clinicaltrials.gov (NCT05031819).
Rationale for the study designIn a pragmatic study design which stems from the fields of service delivery and policy evaluation, the SW-CRT allows for robust evaluation while factoring in logistical (i.e., rolling out of facilities) or political (i.e., relating to the policymakers and service managers) constraints common with a standard parallel randomized controlled trial (RCT) design [28]. In this study, the sequential crossover of PHCs from TASSH-only to TASSH-plus PF permits rigorous evaluation of the implementation strategy effects while enabling all study facilities and participants the benefit of TASSH with PF training.
Along with the robust nature of the stepped wedge design, we will evaluate the PF experimental condition using the RE-AIM framework. Widely used in both health research and health intervention programming and evaluation, RE-AIM offers a systematic guide for collecting and analyzing data to examine all aspects of planning, implementation, and potential sustainability [29]. For this study, RE-AIM is most appropriate to evaluate and identify the program elements critical for implementation and sustainability.
Study setting and populationThirty-two PHCs from a network of 59 PHCs across Akwa Ibom were recruited into the study — 2 for the pre-implementation phase and 30 for the implementation phase. These PHCs support a sizeable number of PLWH. Adoption will be measured on all eligible persons to be screened for hypertension. Eligible patients are identified from the roster of PLWH during routine visits and through linkages from community screening and proximal HIV clinics. In the 30 implementation study sites, we will recruit and enroll an average of 28–32 patients, for a maximum of 960 PLWH participants with uncontrolled hypertension to be followed longitudinally for BP outcomes. Eligibility criteria include the following: (1) HIV-positive persons aged 18 years or older; (2) either currently enrolled in HIV treatment services at one of the 30 study PHCs, receiving hypertension treatment services at one of the 30 study PHCs, or can be enrolled at one of the 30 study PHCs to receive hypertension services for the entire study duration; (3) (for those being followed for BP control) have elevated BP between 140–179 mm Hg systolic and/or 90–109 mm Hg diastolic, as determined by the average of the latter two of three separate BP readings during one clinic visit; and (4) be able to provide consent. The inclusion criteria are based on WHO’s CVD treatment guidelines [30,31,32].
Those who refuse, who are unable to provide informed consent, or with any of the following criteria at baseline will be ineligible for inclusion in the longitudinal BP cohort: (1) BP of ≥ 180/110 mm Hg; (2) known history of kidney disease, heart disease, diabetes mellitus, transient ischemic attacks, stroke, or heart failure; and (3) are pregnant or breastfeeding at the time of enrollment.
Description of TASSH and the PF implementation strategyAs previously noted, our Lagos study [16] provides thorough details of TASSH and the approach for developing the PF implementation strategy. Here, we briefly describe both and specify any potential differences for this study.
TASSH uses a four-step approach for identifying, counseling, treating, and referring (ICTR) and the 5As counseling strategy (ask, assess, advice, assist, & arrange). The four steps are defined as follows: (1) identifying PLWH patients with uncontrolled hypertension (BP > 140/90); (2) initiating counseling by giving clear advice on how PLWH patients can modify their behaviors; (3) treating PLWH with uncontrolled hypertension by prescribing medication treatment according to the Nigerian Simplified Hypertension Protocol; and (4) referring patients with severely elevated BP and/or a chronic comorbid condition, including established CVD, to physicians for further care. The 5 As have been implemented in previous TASSH studies [11, 16, 17, 25] and applied to other health outcomes [33, 34].
As described, we will test the effect of PF on the adoption of TASSH and systolic BP reduction. We used a context-specific approach to develop and guide the PF implementation strategy based on three main components: (1) formation of an advisory board to guide the PF intervention, (2) development of the PF strategy, and (3) training of community nurses on TASSH protocol implementation.
The advisory board constitutes members from the National Agency for the Control of AIDS (NACA), the Federal Ministry of Health (FMOH), the Directorate of Nursing, Akwa Ibom State Ministry of Health, Akwa Ibom State Agency for Control of AIDS (AKSACA), two physicians, two community nurses, and three patient advocates. Development of the PF strategy included the following: (1) training the practice facilitators using a train-the-trainer model [35] guided by the study-developed three Es, i.e., engaging, enhancing, and evaluating the nurses on performing their TASSH duties and delivering the hypertension protocol, (2) identifying site champions and coordinators, (3) building consensus for quality improvement targets, (4) implementing practice changes to support TASSH implementation, and (5) peer-to-peer collaboration. Additional details on the training approach for TASSH and the PF implementation strategy are detailed in prior work [16].
PF justification and approachPF is designed to stimulate specific, actionable steps that PHCs can use to build a robust and context-appropriate foundation for integrating TASSH components. Senior or retired healthcare nurses are trained as coaches and help develop the skills needed in order to adopt evidence-based interventions. The PF strategy combines one-on-one onsite facilitation with shared learning opportunities across practices via peer-to-peer phone calls and text messaging. Practice facilitators are expected as follows: (i) coordinate meetings with PHC nurses, (ii) assist PHC nurses in setting performance goals, (iii) strategize on how to best implement TASSH, and (iv) test workflow changes within PHCs.
During the implementation phase, practice facilitators will support PHCs and nurses implementing TASSH. Facilitators will coordinate monthly telephone calls and onsite meetings (twice during the first month and monthly thereafter). Key tasks for the onsite meetings include reviewing baseline data and assisting nurses to set targets for their weekly workload at the first meeting and troubleshooting workflow issues in subsequent visits. Monthly check-in phone calls will provide opportunities for nurses to raise challenges that may arise with implementing TASSH.
Enrollment, randomization, and allocationIn the pilot phase, two PHCs were recruited to refine and understand data collection strategies, instruments, training timing and methods, and study recruitment methods. For the SW-CRT, 30 PHCs are randomized in five cohorts of six PHCs. Within each PHC, we anticipate enrolling approximately 28–32 PLWH on average. The enrollment targets for each PHC are based on its smaller, mid-sized, or large caseload. We do not anticipate any attrition in study sites. In the event that a site does drop out for any reason, we have adequate numbers of sites with similar characteristics to recruit from PHCs that the Agency oversees.
Study biostatisticians developed the randomization sequence to allocate each PHC to a stepped wedge cohorts. These allocations are kept in a secure electronic format inaccessible to study sites, in accordance with CONSORT guidelines. Study coordinators will be informed of which PHCs are allocated to each cohort just before each training period begins. Because of the nature of the intervention, it is impossible to mask individuals, nurses, practice facilitators, and study coordinators to the group assignment when implementation begins. One study biostatistician will remain blinded to treatment assignment until all data have been collected and the database is locked.
Recruitment and retentionPrimary healthcare centers (PHCs)Throughout Akwa Ibom, the majority of PHCs provide HIV treatment services. Building on the pre-implementation phase findings, we worked closely with the Akwa Ibom State Ministry of Health and the Agency to select two pilot PHC sites and the 30 PHCs for the SW-CRT. Selection of eligible PHCs was based on geographical areas distinct from one another to allow for an equal mix of urban and rural PHCs. PHCs agreed to participate, signed memorandum of understanding (MOU) agreements, and identified at least two nurses to be trained to deliver TASSH and collect study data. Leveraging our experience from our other trials [17, 25, 36] and best practices from the literature on PF [21, 37, 38], we will use several strategies to retain PHCs enrolled in the study. These include the following: signed MOUs, identifying a champion or facility case manager as a liaison, providing monetary incentives for nurses, and maintaining open communication through phone calls, emails, etc.
PatientsAll PLWH treated at the PHCs will receive TASSH, as it is aligned with the Nigerian Hypertension Treatment Protocol, the current standard of care. Working closely with study trained nurses at the 30 PHCs and based on the data from the facility assessment, research coordinators will develop a recruitment strategy tailored to each study site for the BP longitudinal cohort. After study trained nurses identify an eligible PLWH with uncontrolled hypertension meeting the inclusion criteria, he or she will describe the study and refer the patient to a research coordinator to obtain informed consent if the patient is willing to participate. Each PHC will recruit an average 28–32 PLWH with uncontrolled hypertension who meet the eligibility criteria for the BP longitudinal cohort.
Practice facilitatorsSenior nurses with extensive clinical and managerial experience working in PHCs as trainers were recruited as practice facilitators to support clinic nurses implementing TASSH. Working with the Akwa Ibom State Directorate of Nursing which oversees the training, planning, and evaluation of capacity building programs, we recruited and hired six senior nurses as practice facilitators. Each practice facilitator will work with six study sites for the study duration. The decision to recruit and hire senior nurses as practice facilitators is due to the hierarchical nursing structure in Nigeria wherein senior nurses are responsible for providing oversight and support of nurses within PHCs. Working within the current nursing structure enhances the sustainability and adoption of TASSH beyond the study period.
Primary outcomeAdoption (i.e., uptake) is the utilization of components of TASSH. TASSH adoption will be defined as nurses showing utilization of all of the following components: (1) identifying PLWH with uncontrolled hypertension, (2) measuring PLWH’s anthropometrics and BP with a valid automated device following standard procedures, (3) initiating lifestyle counseling and medication treatment every 1–3 months, and (4) referring PLWH with severely elevated BP and complicated hypertension to physicians for further care. Adoption will be measured at the clinic level, in aggregate, each month from the baseline period of the first cohort through the end of follow-up, for all those PLWH with BP screens by case managers or those previously diagnosed with hypertension at a prior visit by the nurses. Table 1 expands on the specific measures of adoption.
Table 1 Measurement of adoptionSecondary outcomesSecondary outcomes include BP control, implementation fidelity, and TASSH sustainability. BP control is defined as a BP less than 140/90 mm Hg. For those consented and enrolled, at baseline visit, three BP readings will be taken by nurses using an automated BP monitor with the participant seated comfortably for 5 min prior to the measurements, following standard guidelines. The average of the latter two BP readings will be used as the measure for each visit. The same procedure will be followed for each participant visit, including the 12-month visit. Uncontrolled BP is defined by an average clinic systolic BP ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg following the guidelines set forth by WHO for CVD treatment [31, 32] and in accordance with the Nigeria Hypertension Treatment Protocol.
Fidelity to TASSH will be measured throughout the study and defined by five dimensions: (1) adherence to the program protocol, (2) dose of the program delivered, (3) quality of program delivery, (4) participant responsiveness, and (5) program differentiation. Tools to assess fidelity were developed for this study and adapted from the current literature [39,40,41]. Fidelity measures will evaluate adherence from the perspective of the PF, nurses, and the participants.
Sustainability is defined as the maintenance of TASSH adoption at HIV clinics at 18 months (6 months after the end of each cohort’s TASSH + PF phase). Sustainability will be assessed similarly to adoption (as defined above) and qualitatively, based on interviews with nurses and clinic leadership at 18 months. The research coordinator will conduct the interviews with two nurses and one key leadership personnel at each clinic. The interviews will be guided by i-PARiHS and inquire about attitudes regarding TASSH implementation, barriers, facilitators, and implications for scalability. All interviews will be recorded, transcribed, and analyzed with NVivo Version 11.
留言 (0)