
記住我
A 16-year-old female patient, born and living in Colón, Esmeraldas, Ecuador. Family history: grandfather with high blood pressure (HBP), maternal grandmother with HBP, diabetes, breast cancer and sister with pleural effusion of unknown aetiology. Surgical history of umbilical herniorrhaphy 15 years ago. The patient took an unspecified medication to treat a diagnosed urinary tract infection two weeks before this hospitalisation (first week of November 2021).
On 23 November 2021, the patient was admitted to the emergency department complaining of a moderately pressing headache, mild oppressive retrosternal pain and dyspnoea at rest for 24 h. There was also an unquantified temperature increase, hyporexia and asthenia for two weeks.
On physical examination, blood pressure was 109/63 mmHg, heart rate 126 bpm, respiratory rate 28 min, temperature 35.9 °C, oxygen saturation 90% with 0.5 L O2 via nasal cannula. Weight 49 kg and height 1.62 m with a body mass index of 18.7 kg/m2. Conscious, oriented, dehydrated, diaphoretic patient. Dry oral mucosa, dry lower lip with thrush. Persistent chest expansion, tachypnoeic. Lung auscultation showed absent breath sounds in the left lung base and decreased air entry in the right lung base with fine crackles. Abdomen increased air-fluid sounds.
Based on the clinical findings, chest tomography, complete blood count, C-reactive protein, procalcitonin, erythrocyte sedimentation rate, lactate dehydrogenase (LDH), d-dimer, ferritin, serum iron, liver profile, blood biochemistry, electrolytes, coagulation, hormones, and lipid profile were requested (Table 1). Tests for human immunodeficiency virus infection were negative on two separate tests. Thoracic tomography (Fig. 1A) showed a pleural effusion in the left hemithorax, an approximate volume of 485 mL, and a maximum density of 38 hu.
Table 1 Lab results of the caseFig. 1
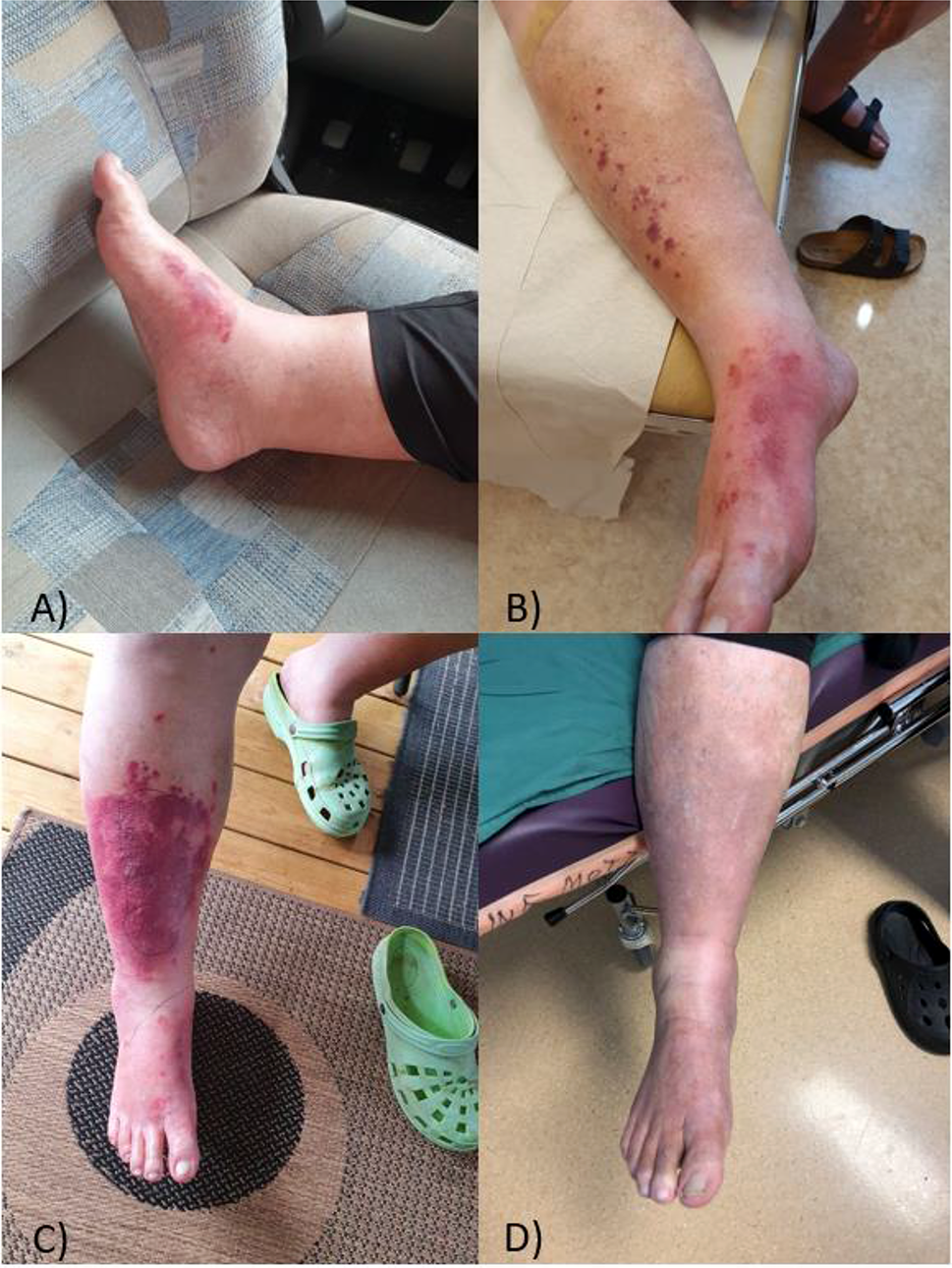
Relevant radiological and microbiological findings of the case. A Thoracic tomography shows pleural effusion in the left hemithorax, approximate volume 485 mL, maximum density 38 hu, parietal and visceral pleura thickening, and mediastinal calcifications. Left anterior apical calcified granuloma, subpleural laminar and segmental atelectasis left basal consolidation with aerial bronchogram. Pre-aortic and subcarinal reactive nodules. Small right pericardial effusion. B Female helminth of A. lumbricoides obtained from the patient's vomit. C Mycobacterium tuberculosis isolated from lung biopsy on Lowenstein Jensen agar. D Culture of a lung biopsy on Sabouraud agar with chloramphenicol showing filamentous growth of Curvularia hawaiiensis. E Microscopic view of C. hawaiiensis ha colony with ellipsoid conidia, rounded at the ends, pale brown, medium reddish brown to dark brown, three septa
On 24 November 2021, it was decided to perform a pleural puncture, during which 120 mL of yellow-green fluid was obtained. Examination of the pleural fluid (Table 1) revealed the presence of leukocytes with 97% monocytes, erythrocytes and LDH 735. In addition, Ziehl–Neelsen staining was negative for mycobacteria, adenosine deaminase was negative, and amplification of nucleic acids by GeneXpert MTB/RIF detected Mycobacterium tuberculosis. Based on these results, an administrative procedure was initiated with the Ecuadorian Ministry of Health to obtain antituberculous therapy. On the same day, the patient experienced spontaneous vomiting at night, and according to the laboratory report, a female Ascaris lumbricoides was detected (Fig. 1B).
On 25 November 2021, antibiotic therapy was started with ampicillin plus sulbactam 3 grammes intravenously every 6 h daily for seven days. In addition, albendazole 400 mg orally was introduced for one dose.
On 25 November 2021, fever and chest pain persisted despite intravenous antipyretic medication at therapeutic doses. Therefore, cardiothoracic surgery performed thoracoscopy, complete lung decortication, parietal pleurectomy and wedge-shaped lung resection. Lung and pleural biopsy showed growth of M. tuberculosis in a culture that responded to first-line antituberculosis drugs (Fig. 1C). In addition, Curvularia hawaiiensis (Fig. 1D, E), was isolated from a fungal culture of lung tissue and identified by sequencing the internal transcribed spacer and D1/D2 regions of the rDNA (7 December 2021).
On 26 November 2021, oral antituberculosis therapy was started with isoniazid (245 mg), pyrazinamide (1225 mg), ethambutol (735 mg) and rifampicin (490 mg) for two months. And 6 months were completed with rifampicin and isoniazid.
The patient was treated with itraconazole 200 mg twice daily for 16 weeks. Monthly follow-ups were done for the first three months, and the patient showed no progression of her infections. One year ago, there were no relapses or new hospitalisations at the follow-up.
留言 (0)