
記住我





Artificial intelligence (AI) is defined as the use of computers to perform tasks that normally require human intelligence and over the past few years has emerged as a potential clinical tool in nephrology.1 Specifically, AI has begun to demonstrate potential clinical utility, including risk prediction, AKI identification/notification, AKI phenotypes, and imaging transcriptomics.2–5 These new AI tools need to be thoroughly evaluated to determine utility in clinical care, including but not limited to controlled clinical trials. We will discuss the current literature, limitations, and potential future directions for using AI in the setting of clinical AKI.
AKI Risk Prediction and DetectionThe AI-AKI literature has focused on risk prediction and detection of AKI.3,4,6 Unsurprisingly, AI and advanced learning techniques can identify trends in large-scale clinical data that are subsequently associated with changes in serum creatinine and urine output. In isolation, AI-AKI risk scores remain imperfect; even when they have been validated in multiple independent cohorts3 or demonstrated to outperform other AKI biomarkers,6 they should be used in concert with physician assessment. These tools need to undergo intense examination through clinical trials to determine their ability to meaningfully improve outcomes.
Skepticism may exist to implement AI-AKI risk prediction tools; however, it is clear that in the current paradigm, patients with established AKI are not receiving guideline-based care.7 Nevertheless, if these tools are operationalized, they may obviate the need to implement current guideline-based care, by preventing serum creatinine or urine output–defined AKI. These AI risk scores have been shown to detect AKI risk 36–48 hours before there are significant changes in serum creatinine.3,6 Data on the implementation of these AI-AKI scores and their impact on outcomes are lacking. Despite excellent specificity and negative predictive value, these scores uniformly suffer from lower than optimal positive predictive values (PPVs) (20%–50%), which has limited their wide-scale implementation. There are significant costs to clinically implementing any risk score, and enthusiasm may be dampened because they are much better at ruling out impending AKI rather than ruling it in.
Existing data demonstrate AKI alerts at the time of serum creatinine increases and urine output decreases paired with clinical care plans/recommendations can have mixed results; some studies have shown improved outcomes such as shorter lengths of stay and improved compliance with nephrology guideline–based care8,9; whereas others have demonstrated a signal for harm.4 These trials used AI sniffers to detect AKI and did not implement their interventions until after AKI had been clinically established. It is unknown how much of these results were due to “horses that had already left their respective barns”; future trials should implement guideline-based care bundles using AI risk algorithms that alert a patient's high-risk AKI status before presence of clinical AKI. These trials could consider combining other risk assessment tools, which may improve the aforementioned mediocre PPVs (severity of illness scores, biomarkers of AKI) to further enhance AKI risk prediction. If these combined-tool trials are successful in improving outcomes (development/severity of AKI, length of stay, postdischarge outcomes), it may reshape our definitions of clinical AKI and diminish our outdated reliance on serum creatinine and urine output.
Phenotypes of AKIIn addition to detecting early AKI risk, AI and advanced learning techniques have been used to detect phenotypes of AKI. All AKI is defined by changes in two generic functional biomarkers of the kidney and does not discriminate the underlying source of injury nor provide insights into specific injury pathways (ischemia, inflammation, nephrotoxins) or potential treatment strategies. Functional biomarkers alone (serum creatinine and urine output) do not accurately identify patients who are at high risk for the most severe forms of AKI (e.g., requiring dialysis). Not all patients with stage 3 AKI go on to require dialysis or have AKI that persists for several days. Nephrology needs new tools to identify those at risk for these adverse outcomes.
A recent study of electronic health record data (vital signs, laboratory test results, demographics, and comorbidities) from 4001 intensive care unit patients in a tertiary care hospital was able to detect three distinct phenotypes within sepsis-associated AKI.5 Despite all having AKI in the setting of sepsis in the same intensive care unit, these phenotypes had different tendencies in their preadmission comorbidities and different risks regarding inpatient mortality or the need for dialysis. These phenotypes need to be validated in prospective data and then investigated to determine whether these phenotypes will preferentially respond differently to the same therapies.
Separately, in a post hoc analysis using latent class analysis and a cohort of 1219 patients with sepsis-associated AKI from the Vasopressin in Septic Shock Trial, investigators identified two distinct AKI phenotypes with different risks for renal nonrecovery and 28-day mortality. These two novel sepsis-associated AKI phenotypes also demonstrated unique responses to vasopressin therapy.10 One of the phenotypes had improved 90-day mortality when randomized to receive vasopressin (27% versus 46%).10 Separate from this improved mortality, the addition of biochemical biomarker to these phenotypes further modified AKI risk. Adding angiopoietin 1 and 2 and IL-8 concentrations with genotyping data around single nucleotide polymorphism near the angiopoietin-2 gene identified patients at decreased risk of AKI. Each T-allele present was associated with lower serum angiopoiten-2 levels and a lower risk of developing sepsis-associated AKI.11 Thus, advanced learning techniques are able to identify unique cohorts of patients who are not clinically apparent on first glance. Identifying which patients are more likely to benefit from certain therapeutic interventions and/or more likely to progress to certain outcomes is a crucial next step in AKI research.
Future AI-AKI investigations may determine certain treatments or guidelines are more beneficial in certain clinical settings. Phenotyping tools need to be independently validated and then prospectively investigated to determine whether real-time implementation improves patient outcomes. A multimodal risk assessment that could include combining AI risk tools with biochemical biomarkers (e.g., serum creatinine, angiopoiten-2) and genetic biomarkers may work to change the prognosis of sepsis-associated AKI.
Kidney Precision Medicine ProjectThe Kidney Precision Medicine Project (KPMP) seeks to redefine AKI by integrating molecular phenotypes with clinical characteristics, digital pathology, and patient outcomes.2 The KPMP will obtain kidney biopsies from patients with AKI and create a kidney atlas, characterize AKI phenotypes on the basis of molecular mechanisms, and identify critical cells/pathways and potentially develop novel therapeutics. This work, while still in its infancy, will help implement precision medicine for patients with AKI (and other forms of kidney disease). AKI biopsy samples will be processed using multiple molecular interrogations (in addition to traditional histologic evaluations) including kidney tissue span imaging, transcriptomics, proteomics, and spatial metabolomics.2 Given the sheer volume of data that will be generated from these samples, several AI and augmented learning techniques will be implemented. The long-term goal of this project is to develop new methods of molecular analysis, digital pathology, imaging techniques, and bioinformatics to reshape the diagnostic process of AKI.2 However, as of the last quarter of 2022, this project is actively enrolling its first 200 participants (for AKI and CKD) to evaluate safety and feasibility issues. Our sincere expectation is that the KPMP and its use of AI, augmented learning, and omics technology will change the way we perform, collect, and interpret kidney biopsies and potentially improve the implementation of care post-AKI biopsy.
Future of AI in AKIAI and advanced learning techniques are currently being evaluated in several aspects of AKI. Are they guaranteed to be a success? No, they are not. Care must be taken to ensure that these new tools are being developed under scientific rigor but also that they are being developed justly and free of bias. As nephrologists, we have lived through the missteps of including factors such as race into CKD assessment, and these new AKI tools are no different. As these AKI tools are being developed and preliminarily validated, we must minimize any bias, construct, and implement them based on multicenter data, ensuring that randomized trials are performed to determine the impact of these tools on clinical care and patient outcomes. Given the nature of these novel AKI tools and the evolving world of clinical trials and implementation science, newer trial designs can be used including pragmatic, cluster-randomized, and platform trials.
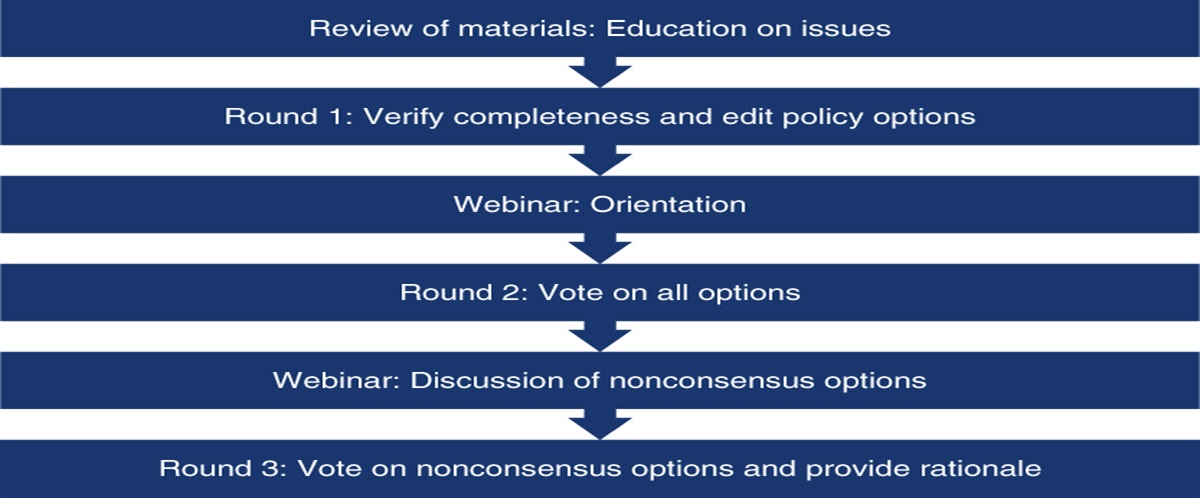
We stand at an inflection point in AKI research, where AI and augmented learning may help identify which patients are most likely to benefit from specific AKI interventions. These AI-AKI tools may allow us to revisit prior interventions that were trialed in lower risk patients, based solely on changes in serum creatinine and urine output. These tools need to be thoroughly validated and investigated and paired with clinically meaningful interventions. The trials used to study these tools need to be controlled, free of bias, appropriately powered, and relatively easy to conduct and replicate. Figure 1 depicts the timeline/process of validating, implementing, and studying an AI tool. As nephrologists, there is great reason for cautious optimism around the power of these AI tools to reshape when, how, and to whom we deliver AKI care. Perhaps, these AI-AKI tools can help end the subtle nihilism that exists on hospital rounds around treating those with AKI.
 Figure 1:
Figure 1: Flow chart for an AI-AKI tool. An AI-AKI tool is developed and validated to ensure it accomplishes its designated task (risk assessment, phenotyping, and treatment targets). Then, the tool needs to be rigorously investigated to determine that it permits a beneficial intervention within an actionable time frame. Then, investigators should be able to measure a variety of clinically meaningful AKI outcomes. If the model is successful, it should be clinically implemented and can be recalibrated and monitored over time to ensure it continues to improve outcomes, and if the model is unsuccessful, then it will undergo critical re-examination and redevelopment. AI, artificial intelligence.
DisclosuresT. Bajaj reports ownership interest in CDTX, DIDI, KO, MRK, PCOR, and TLRY. J.L. Koyner reports consultancy agreements with Astute Medical/Biomerieux Baxter, Biomerieux, Guard Therapeutics, Mallinckrodt, Novartis, and SeaStar; research funding from Astute Medical, Biomerieux, Bioporto, Fresenius Medical, NIH, and NxStage Medical; honoraria from Acute Disease Quality Initiative (ADQI), American Society of Nephrology, CSCTR, and ISICEM; a patent for Pi GST to detect severe AKI after cardiac surgery—with Argutus Medical; serves on the Editorial Boards of American Journal of Nephrology, CJASN, and Kidney360; serves advisory or leadership roles for Scientific Ad Board for the Guard Therapeutics, NKF of Illinois, and Novartis; and serves on speakers bureau for NxStage Medical.
FundingJ.L. Koyner is funded by NIH (R01DK126933).
AcknowledgmentsThis article is part of the Artificial Intelligence and Machine Learning in Nephrology series, led by series editor Girish N. Nadkarni.
The content of this article reflects the personal experience and views of the author(s) and should not be considered medical advice or recommendation. The content does not reflect the views or opinions of the American Society of Nephrology (ASN) or CJASN. Responsibility for the information and views expressed herein lies entirely with the author(s).
Author ContributionsAll authors conceptualized and wrote the original draft and reviewed and edited the manuscript.
References 1. Soranno DE, Bihorac A, Goldstein SL, et al. Artificial intelligence for AKI!Now: let's not await plato's utopian republic. Kidney360. 2022;3(2):376–381. doi:10.34067/KID.0003472021 2. de Boer IH, Alpers CE, Azeloglu EU, et al. Rationale and design of the kidney precision medicine project. Kidney Int. 2021;99(3):498–510. doi:10.1016/j.kint.2020.08.039 3. Churpek MM, Carey KA, Edelson DP, et al. Internal and external validation of a machine learning risk score for acute kidney injury. JAMA Netw Open. 2020;3(8):e2012892. doi:10.1001/jamanetworkopen.2020.12892 4. Wilson FP, Martin M, Yamamoto Y, et al. Electronic health record alerts for acute kidney injury: multicenter, randomized clinical trial. BMJ. 2021;372:m4786. doi:10.1136/bmj.m4786 5. Chaudhary K, Vaid A, Duffy Á, et al. Utilization of deep learning for subphenotype identification in sepsis-associated acute kidney injury. Clin J Am Soc Nephrol. 2020;15(11):1557–1565. doi:10.2215/CJN.09330819 6. Flechet M, Falini S, Bonetti C, et al. Machine learning versus physicians' prediction of acute kidney injury in critically ill adults: a prospective evaluation of the AKIpredictor. Crit Care. 2019;23(1):282. doi:10.1186/s13054-019-2563-x 7. Moledina DG, Belliveau O, Yamamoto Y, et al. Variation in best practice measures in patients with severe hospital-acquired acute kidney injury: a multicenter study. Am J Kidney Dis. 2021;77(4):547–549. doi:10.1053/j.ajkd.2020.08.013 8. Hodgson LE, Roderick PJ, Venn RM, Yao GL, Dimitrov BD, Forni LG. The ICE-AKI study: impact analysis of a Clinical prediction rule and Electronic AKI alert in general medical patients. PLoS One. 2018;13(8):e0200584. doi:10.1371/journal.pone.0200584 9. Selby NM, Casula A, Lamming L, et al. An organizational-level program of intervention for AKI: a pragmatic stepped wedge cluster randomized trial. J Am Soc Nephrol. 2019;30(3):505–515. doi:10.1681/ASN.2018090886 10. Bhatraju PK, Zelnick LR, Herting J, et al. Identification of acute kidney injury subphenotypes with differing molecular signatures and responses to vasopressin therapy. Am J Respir Crit Care Med. 2019;199(7):863–872. doi:10.1164/rccm.201807-1346OC 11. Bhatraju PK, Cohen M, Nagao RJ, et al. Genetic variation implicates plasma angiopoietin-2 in the development of acute kidney injury sub-phenotypes. BMC Nephrol. 2020;21(1):284. doi:10.1186/s12882-020-01935-1
留言 (0)