Vestibular evoked myogenic potential (VEMP) is an objective method for assessing the otolithic apparatus and vestibular nerve conduction pathways in the vestibular system, such as the utricle and saccule, and is a myogenic potential recorded after stimulation of the otolithic apparatus by high-intensity acoustic signals [1]. Depending on the placement of the recording electrodes, VEMP examinations can be divided into cervical vestibular evoked myogenic potentials (cVEMPs) and ocular vestibular evoked myogenic potentials (oVEMPs). The oVEMP reflects the function of the superior vestibular pathway of the utricle and the cVEMP reflects the function of the inferior vestibular pathway of the saccule.
Diabetes mellitus is a metabolic disorder of multiple etiologies, characterized by chronic hyperglycemia and long-term complications [2]. In China, the proportion of people over 20 years of age with diabetes is reported to be 9.7% (about 92.4 million people), and the incidence of abnormal glucose tolerance is 15.5% (148.2 million people) [3]. The growing prevalence of diabetes and its complications has become a major health problem for Chinese nationals, placing a severe economic burden on society. Diabetes can cause a variety of clinical symptoms, among which balance dysfunction (dizziness, falls, etc.) is one of the symptoms commonly complained about by patients with this illness. Although the exact mechanism has not been sufficiently elucidated, Agrawal et al. [4] have indicated that the rate of vestibular dysfunction is 70% higher in diabetic patients than in healthy individuals. The risk of falls is markedly increased in DM and diabetic peripheral neuropathy (DPN), the role of DPN may promote vestibular impairments in these patients [5]. Meng Y et al. [6] performed vestibular function examination on 62 pre-diabetic patients and found that the incidence of vestibular impairment in diabetic patients was 71%. Vestibular impairment may be a major factor in the development of balance disorders in diabetics.
The detection of vestibular function in diabetics has received attention due to the increasing recognition of the impact of vestibular impairment on imbalance and falls in diabetics. Diabetic patients may develop vestibular dysfunction in the absence of significant vestibular symptoms [7]. Many researchers have identified various vestibular symptoms and vestibular test abnormalities in people with type 2 diabetes. While vestibular tests may be abnormal, these changes may be present in the absence of vestibular symptoms. In such cases, vestibular lesions can be identified by objective vestibular diagnostic testing tools, despite the absence of vestibular symptoms in patients with DM. Previous studies have used electronystagmography instruments to evaluate changes in vestibular function using spontaneous nystagmus tests, position tests, head shake tests, neck turn tests, temperature tests, and visual oculomotor system examinations (gaze test, sweep test, smooth tracking test) [8], but there are limitations due to the examination technique and patient cooperation. At present, VEMP testing constitutes an important part of the vestibular test battery and provides either diagnostic or assistive contributions in the clinical evaluation of common vestibular diseases such as Meniere’s disease (MD), vestibular neuritis (VN) and superior canal dehiscence syndrome (SCDS) [9]. In 2001, Perez et al. [6] assessed vestibular evoked potentials in experimentally induced type 2 diabetic animals, showing vestibular damage in the inner ear. However, the research literature on VEMP response in diabetics remains limited. The present study aimed to compare cVEMP and oVEMP in diabetes, subclinical diabetic peripheral neuropathy, DPN and healthy controls, and to assess the lesions of peripheral vestibular end organs by changes in parameters such as wave latency and amplitude, and to illustrate the impact of DPN on vestibular function in patients with DM.
Materials and methods
This study was conducted at the Second Hospital of Fujian Medical University (Fujian, China), in accordance with the guidelines of the Declaration of Helsinki, and was approved by the Ethics Committee of the Second Hospital of Fujian Medical University [Ethics Approval No.: Lun Audit (Research) No. 213 of 2021].
Participants
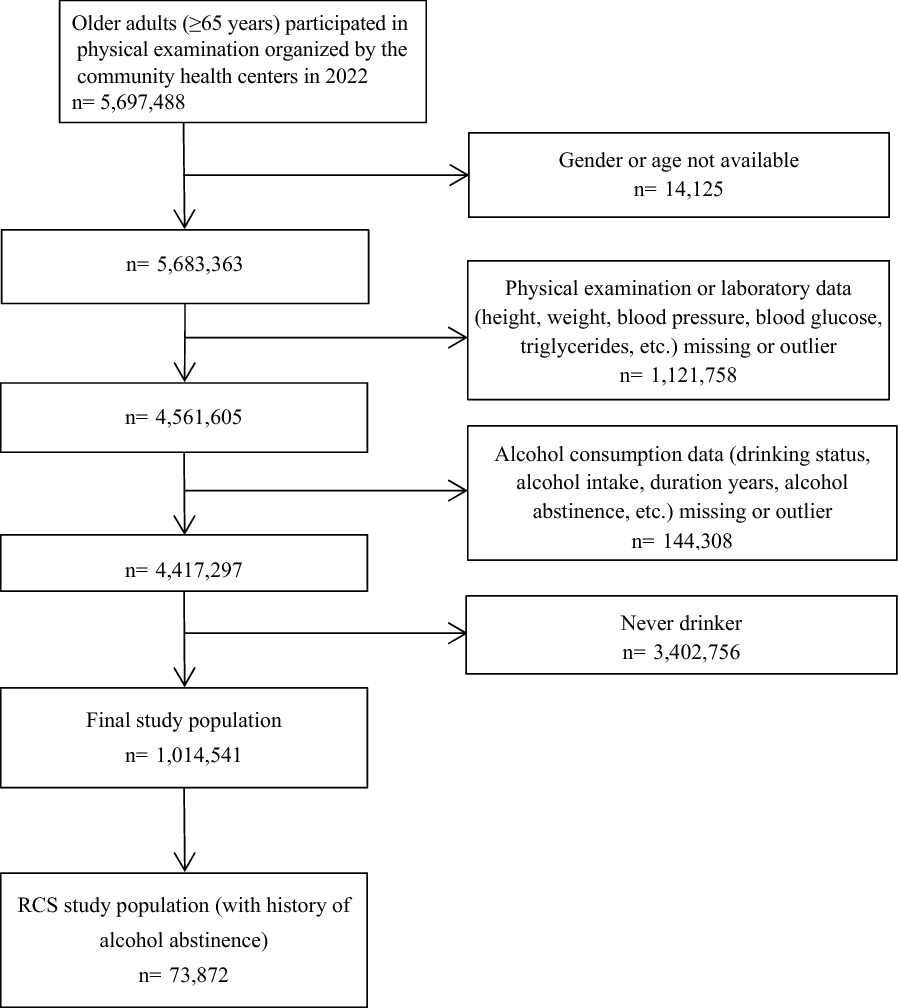
89 patients with type 2 diabetes who visited the Second Hospital of Fujian Medical University from April 2021 to November 2021 were enrolled in this study, including 57 males and 32 females with a mean age of (53.0 ± 11.9 years). There were 42 cases in the healthy control group, including 23 males and 19 females, with a mean age of (52.3 ± 5.6) years. (for details, see Table 1).The diagnosis of diabetes was based on the American Diabetes Association (ADA) (2021) diabetes diagnosis criteria [10]. The subjects had no existing/historical records of any otological disorders, nor any historical or existing vestibular complaints (such as dizziness, vertigo, nausea). Patients present with a history of head-and-neck injury, limited neck mobility, history of head and neck surgery, central nervous system disorders; those who present with diseases involving external or middle ear, those who present with a history of usage of drugs such as ototoxic drugs, antiepileptics, muscle relaxants; those who were unable to cooperate were excluded from the study. The patients gave permission for all of the procedures involving clinical tests and data collection, with approval by the ethical committee of the Second Hospital of Fujian Medical University, China. General information including gender, age, body mass index, duration of diabetes, glycated hemoglobin (HbA1c), fasting blood glucose(FBG), blood pressure, smoking history, triglycerides, total cholesterol, low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) were recorded for all participants.
Test used
All subjects were examined using an electromyographic evocator (Keypoint 9033A07, Focus), including nerve conduction velocity measurement, cVEMP test, and oVEMP test. All subjects were tested in a quiet environment.
Nerve conduction velocity examination
All enrolled patients were examined by a neurologist specializing in nerve conduction velocity. Diabetic peripheral neuropathy was diagnosed using the diagnostic criteria of the Expert consensus on the diagnosis and management of diabetic neuropathy (2021 Edition) [11]. Diagnosis of distal symmetric polyneuropathy or multiple peripheral neuropathies by nerve conduction velocity examination. 89 patients with Type 2 Diabetes in the present study consisted of three groups: 29 patients with no peripheral neuropathy (NDPN group), 26 patients with asymptomatic neuropathy (SDPN group), 34 patients with symptomatic neuropathy (DPN group).
The diagnostic criteria for diabetic peripheral neuropathy include the following three points: (1) definite presence of diabetes; (2) presence of clinical and/or electrophysiological evidence of peripheral neuropathy; and (3) exclusion of other causes of peripheral neuropathy [11]. The clinical manifestations are symmetrical pain and paresthesia, with paresthesia in the early stage and sensory loss in the late stage. The symptoms of lower limbs are more common than those of upper limbs. Electromyography can confirm peripheral neuropathy and assist in determining its type as well as its severity. In asymptomatic diabetic patients, electrophysiological examination can help detect subclinical peripheral neuropathy.
VEMP test
VEMP test was executed using a Keypoint (9033A07, Focus) with the following settings and equipment: 2 channels; The velocity is 10 ms/D; sensitivity 0.2 mV/D; Filters range from 5 Hz to 5 kHz; click sound (300–500 stimuli for 0.1 ms at 5 Hz each); single-channel calibrated stereo headphones and surface electrodes. Consecutive runs were performed to confirm the reproducibility of biphasic waveform for cVEMP and oVEMP. Conversely, cVEMP and oVEMP responses were absent when reproducibility was lacking. The presence of a VEMP reaction was evaluated, and the parameters included latencies (ms) and amplitudes (mV). (1) cVEMP test: The patient was placed in the supine position. Two active electrodes were placed on the upper two thirds of the bilateral sternocleidomastoid (SCM) muscles with the reference electrode on the sternoclavicular joint. Subjects were instructed to lift the head from the pillow so that the sternocleidomastoid muscle contracted and maintained a muscle tension greater than 50 uV. Thereafter, the examiner adjusted the headset stimulus to 135 dB SPL for an average of approximately 300–500 repetitions until a steady waveform was obtained and labeled p13, n23 [[12][13]]. The presence of cVEMP was confirmed when reproducible short-latency biphasic waveforms appeared at certain latencies. The latencies of p13 and n23 were measured. Typical cVEMP waveforms were bidirectional, with the positive wave latency near 13 ms, labeled p13, and the negative wave appearing near 23 ms, labeled n23. The recorded EMG activity was corrected, which reflects the reflected potential originating from the saccule. (2) oVEMP test: The recording electrode was located just below the lower lid margin of each eye in line with the pupil. Subjects were asked to gaze maximally upward by looking at the target point located 60–70 cm from the eyes with a visual angle of 25°, and oVEMPs were recorded from the contralateral extraocular muscles [14]. The n10-p15 composite waveform was recorded as negative followed by positive, and the trough with an upward trend is marked as n10 about 10 ms after the sound is given, and the peak with a downward trend after n10 is marked as p15. The recorded waveform with good reproducibility after 3 repeated utterances of the same intensity was considered as the oVEMP response waveform [12].

留言 (0)