
記住我


The inclusion and exclusion criteria led to the inclusion of 639 CKD patients with CAD from MIMIC-IV in the research (Fig. 1). The median TyG index was 9.1 (8.6, 9.5). Of the 639 CKD patients with CAD who were hospitalized, 102 (15.5%) passed away while 557 others survived. The variations in baseline characteristics are summarized in Table 1 and Additional file 2: Table S1. Serum glucose and TyG index values were greater in patients who passed away while receiving hospital care, and they also had increased risks for liver disease and dialysis (P < 0.001). A total of 128 (19.4%) of the 639 CKD patients with CAD died during the follow-up period (Additional file 2: Table S2).
Fig. 1
Flowchart illustrating the selection of patients from the MIMIC-IV database. MIMIC Medical Information Mart for Intensive Care
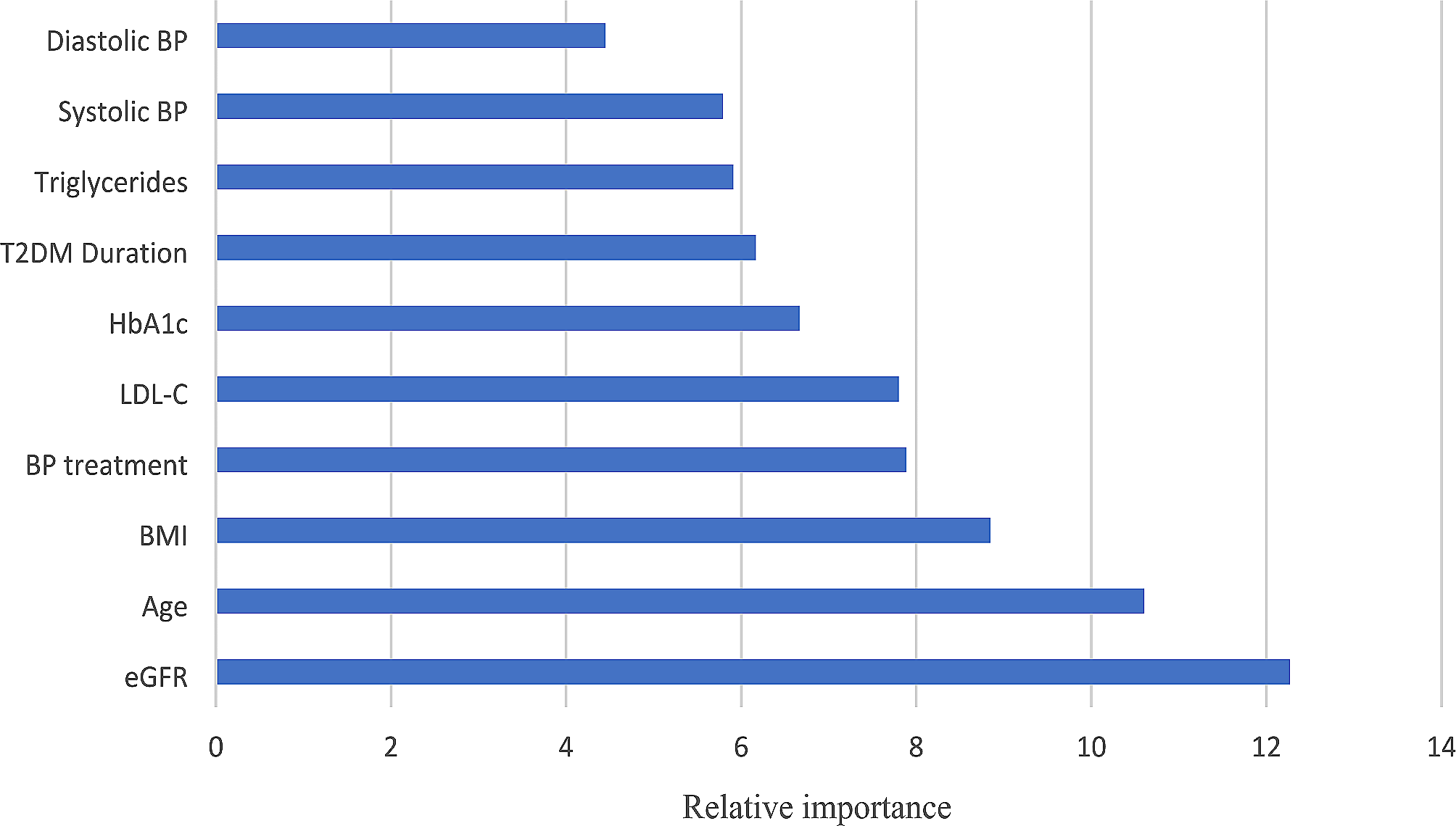
Table 1 The main baseline characteristic for patients included in the study divided by in-hospital situationFeature selectionThirty-two and 34 variables that were the most associated with in-hospital and one-year mortality, respectively, were confirmed using the Boruta method, (Fig. 2, Additional file 1: Fig. S1, and Additional file 2: Tables S3, S4). Although several important characteristics, such as ACS, dialysis, diabetes and hypertension and medication situation, such as aspirin and statin use, were disregarded due to the low Z-value in comparison to the shadow feature, they were nonetheless included in the analysis based on prior research and clinical experience. Factors were chosen for the final complete adjustment model when in the Boruta analysis, their Z-scores were higher than the shadow features or when added to the model, they had the largest matched effect (odds ratio or hazard ratio) among a group of biomarkers (max, mean and min) or they were based on previous findings and clinical constraints.
Fig. 2
Feature selection for the relationship between various TyG indices and in-hospital mortality analyzed by the Boruta algorithm. The horizontal axis shows the name of each variable, while the vertical axis represents the Z-value of each variable. The box plot depicts the Z-value of each variable in the model calculation, with green boxes representing important variables, yellow representing tentative attributes, and red representing unimportant variables. scr serum creatinine, eGFR estimated glomerular filtration rate, ACS acute coronary syndrome, HT, hypertension; max, maximum; min, minimum, WBC white blood cell; RBC, red blood cell, ALT alanine aminotransferase, INR International Normalized Ratio, PT prothrombin time, SOFA sequential organ failure assessment, HR heart rate, SpO2 oxyhemoglobin saturation
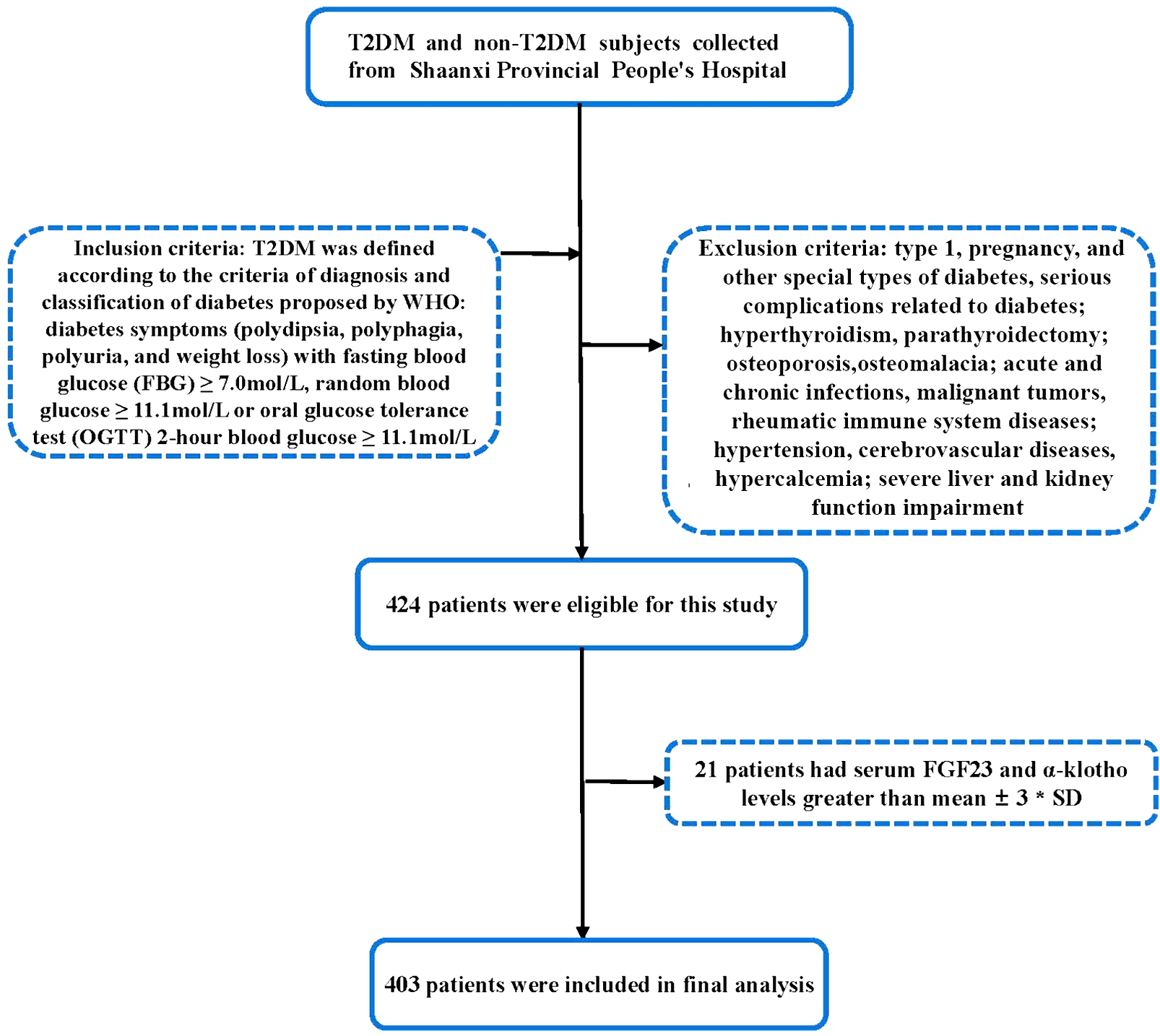
TyG index and in-hospital mortality relationshipAccording to the database, there were 102 in-hospital deaths out of 639 patients (16.0%). The TyG index was found to have a nonlinear relationship with the probability of dying in the hospital according to the multivariable RCS model. When the TyG index was between 8.869 and 9.373, a plateau phase was noticed, and the hazard ratio (HR) value of the TyG index was near 1. The risk of in-hospital death increased with the TyG index, whether it was less than 8.869 or larger than 9.373 (Fig. 3A). The risk of in-hospital mortality and the TyG index were not yet significantly associated in this range.
Fig. 3
Multivariable RCS regression showed the nonlinear association between the TyG index and in-hospital (A) and one-year (B) mortality after full adjustment. The cutoff values in the plot of in-hospital death risk were 8.869 and 9.373, while the cutoff values for one-year mortality were 8.716, 9.037, and 9.664. TyG, triglyceride glucose; RCS, restricted cubic spline
We defined three categories of patients based on the TyG index: Q1 (TyG ≤ 8.869), Q2 (8.869 < TyG ≤ 9.373), and Q3 (TyG > 9.373). The results of multivariable logistic regression (Table 2, Model 3) showed that the TyG index increased the probability of dying in the hospital (OR 1.678, 95% confidence interval [CI] 1.113–2.531) after adjusting for all impact factors identified by Boruta analysis and clinical experience. Compared to the lowest TyG index in Q1 (Table 2, P for trend 0.026), the OR for the incidence of in-hospital death decreased in Q2 (OR 0.968, 95% CI 0.487–1.925); however, it climbed in Q3 (OR 2.165, 95% CI 1.122–4.179).
Table 2 The association between various TyG index groups and in-hospital mortalityOne-year mortality and the TyG index correlationA total of 128 of 639 (20.0%) participants died during the one-year follow-up period. The TyG index was nonlinearly related to the risk of in-hospital death according to the multivariable RCS model. When the TyG index was less than 8.716 or more than 9.664, the 1-year risk of death was positively correlated with the value of the TyG index. The HR value was near 1 when the TyG index ranged from 8.716 to 9.664 with a cutoff value of 9.037 (Fig. 3B).
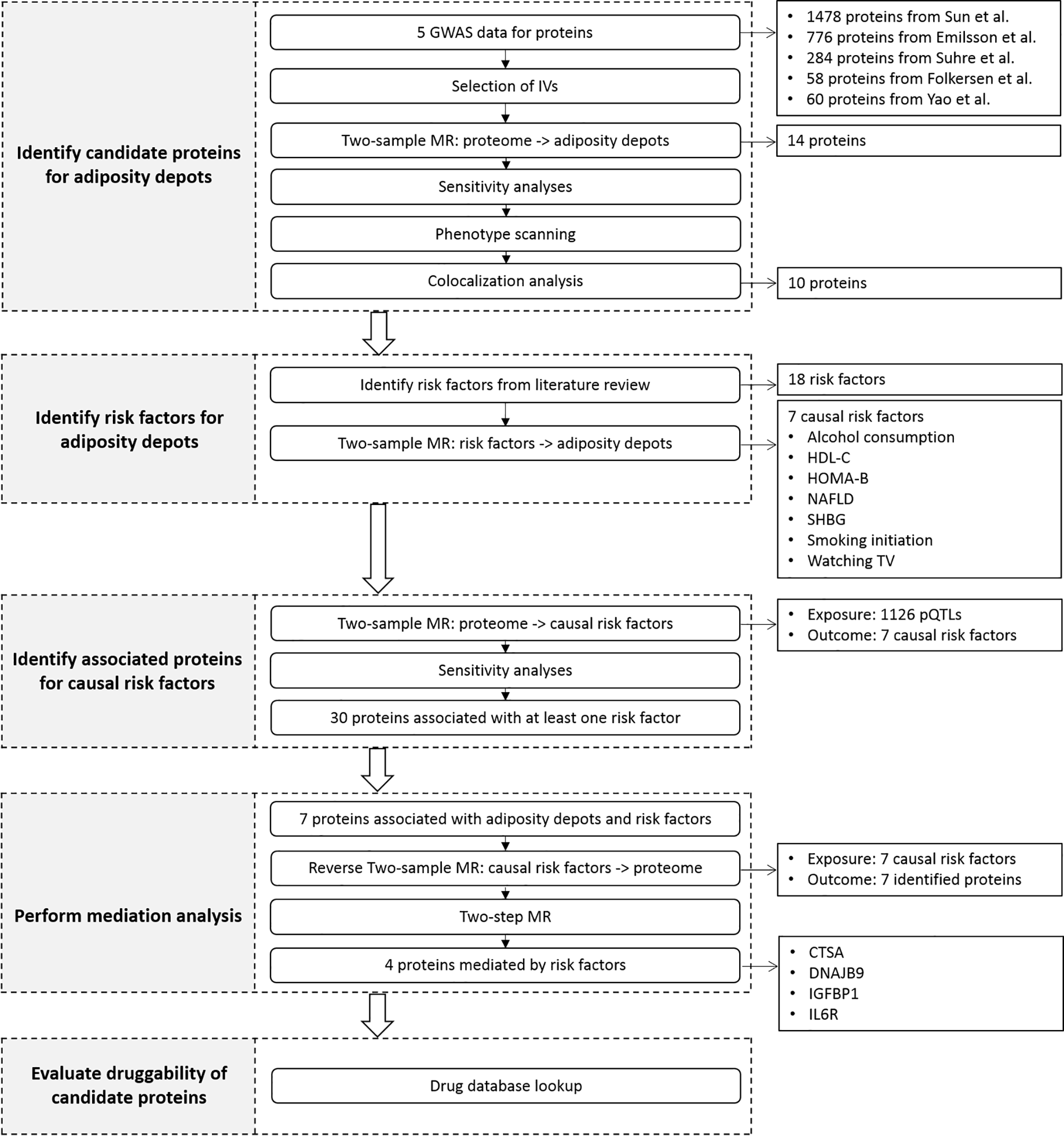
As a result, the participants were divided into four groups based on various TyG indices: T1 (TyG ≤ 8.716), T2 (8.716 < TyG ≤ 9.037), T3 (9.037 < TyG ≤ 9.664), and T4 (TyG > 9.664). The Kaplan–Meier analysis plot showed a significant difference among various TyG index groups (Fig. 4).
Fig. 4
Kaplan–Meier analysis results illustrated the cumulative incidence of one-year mortality in patients with both CKD and CAD in various TyG index groups. TyG triglyceride glucose, CKD chronic kidney disease, CAD coronary artery disease
Overall, multivariable Cox regression analysis revealed an association between the TyG index score and an elevated risk of one-year mortality (HR 1.343, 95% CI 1.020–1.769, P < 0.05). While the HRs of T2 and T3 were reduced (HR 0.750, 95% CI 0.423–1.331, and HR 0.929, 95% CI 0.568–1.520, respectively), the HR of T4 was increased compared to that of T1 (HR 1.627, 95% CI 1.058–2.766). The trend from T1 to T4 was statistically significant but not very pronounced (Table 3, P for trend 0.049).
Table 3 The association between various TyG index groups and one-year mortalitySubgroup analysisTo confirm the relationship between the TyG index and in-hospital mortality as well as one-year mortality stratified by age, sex, kidney function and health status, subgroup analyses were carried out. Age and eGFR level were found to interact with the relationship between the TyG index and in-hospital deaths, whereas sex interacted with the TyG index and one-year mortality. Elderly patients (≥ 75 years), males, those with higher eGFR levels, non-ACS and non-dialysis participants continued to show a similar association between the TyG index and in-hospital risk. The link between TyG and 1-year mortality risk was the same among male and non-ACS patients (Table 4 and Additional file 2: Table S5).
Table 4 The subgroup analysis results of the multivariable-adjusted ORs for the association between the TyG index and hospital mortality
留言 (0)