Study design and patients
Patients (aged ≥18 years) had locally advanced or metastatic solid tumors resistant to standard therapy, or for which no standard therapy had been available, as well as a baseline Eastern Cooperative Oncology Group performance status (ECOG PS) of 0 or 1. To be included, all patients were required to have adequate bone marrow, renal, and liver function. Additional inclusion and exclusion criteria are listed in Supplementary Table 1.
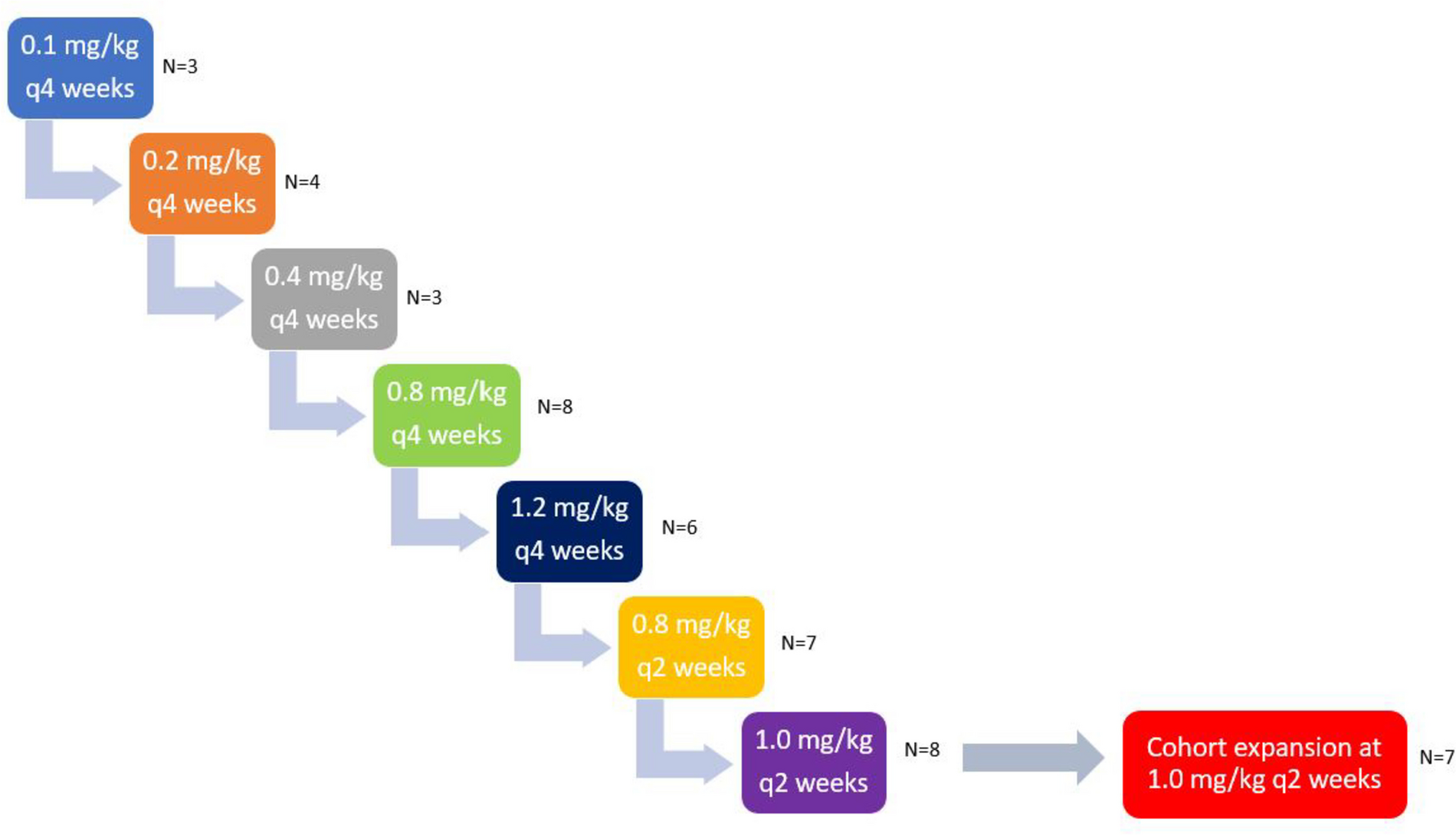
Prior clinical studies have demonstrated the maximum tolerated dose of talazoparib monotherapy to be 1 mg QD in Western and Japanese patients [11, 16]. Based on the established safety profile and approval of talazoparib monotherapy administered at 1 mg QD by the US Food and Drug Administration, European Medicines Agency, and other global health authorities [9, 10], a 3+3 study design was not required.
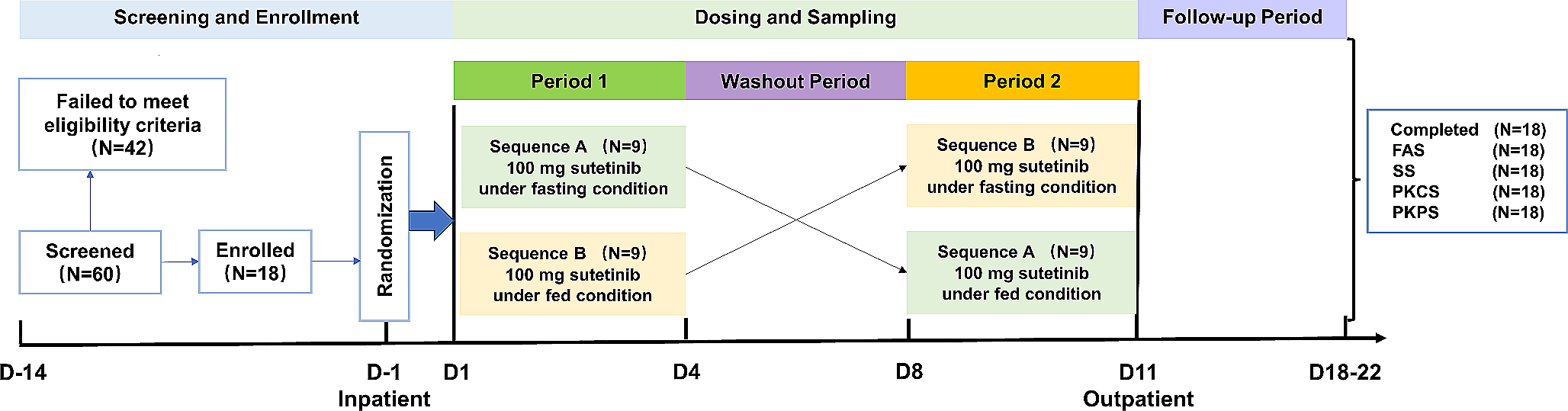
A single dose of talazoparib 1 mg was administered orally on Day –9. From Cycle 1 Day 1, patients received talazoparib 1 mg QD orally on a continuous basis at approximately the same time each day (preferably in the morning) until disease progression, death, unacceptable toxicity, or withdrawal of consent. Dose interruptions or reductions were not required unless toxicity persisted at grade 2 for ≥7 days. Daily dosing was paused for grade ≥3 hematologic toxicities. Supportive care including blood products was allowed as appropriate per local guidance. To minimize any drug-drug interaction effects relating to talazoparib exposure and potential alteration to efficacy, co-medication with P-glycoprotein (P-gp) inhibitors and inducers was prohibited for Cycle 1 when intensive PK assessments were scheduled after both single-dose and multiple-dose talazoparib administrations. After Cycle 1, only potent P-gp inhibitors were prohibited to accommodate more co-medication options.
The final protocol and any amendments were reviewed and approved by the independent ethics committees at each of the investigational centers participating in the study. This study was conducted in compliance with the ethical principles originating in or derived from the Declaration of Helsinki and in compliance with all International Council for Harmonization Guidelines for Good Clinical Practice. Informed consent was obtained from all individual patients included in the study.
Sample size consideration
To support registration of patients with metastatic castration-resistant prostate cancer (mCRPC) and other future potential indications in China, it was determined that 12 evaluable patients were needed to characterize the Chinese PK profile. This number was based on available global talazoparib PK data and with the intention to satisfy regulatory requirements by the China National Medical Products Administration for PK evaluation in a Chinese population. Considering there will be non-evaluable patients, it was estimated that approximately 15 patients were needed to be enrolled.
Endpoints
The primary endpoint was to characterize the single-dose and steady-state PK of talazoparib. Key secondary endpoints included evaluation of the incidence and severity of AEs and efficacy, as evaluated by unconfirmed objective response rate and duration of response.
Pharmacokinetic assessments
To assess the single-dose PK profile, patients took talazoparib on Day –9 of a 9-day (216 h) lead-in period; blood samples were collected at pre-dose and at 0.5, 1, 2, 4, 8, 24, 48, 96, 168, and 216 h post-dose. For the steady-state PK profile, serial samples after multiple doses of talazoparib were collected on Day 22 of the first cycle at pre-dose and at 0.5, 1, 2, 4, 8, and 24 h post-dose. Prior to serial PK sampling (Cycle 1 Day –9, Cycle 1 Day 22), patients were required to fast for at least 8 h before dosing and they had to continue fasting for 2 h after dosing to control the variability due to food effect on Cmax. For the other PK sampling points, talazoparib could have been taken with or without food. On clinic visit days, talazoparib was administered after completion of a pre-dose blood sampling for PK and assessments. Blood samples of approximately 3 mL, to provide a minimum of 1.5 mL plasma, for measurement of talazoparib concentrations were collected.
Safety assessments
AE reporting included data up to 28 days after last dose of study drug or to start of new anticancer drug therapy Day -1 (whichever came first). For AEs, Medical Dictionary for Regulatory Activities (MedDRA), version 24.0, coding was applied.
Efficacy assessments
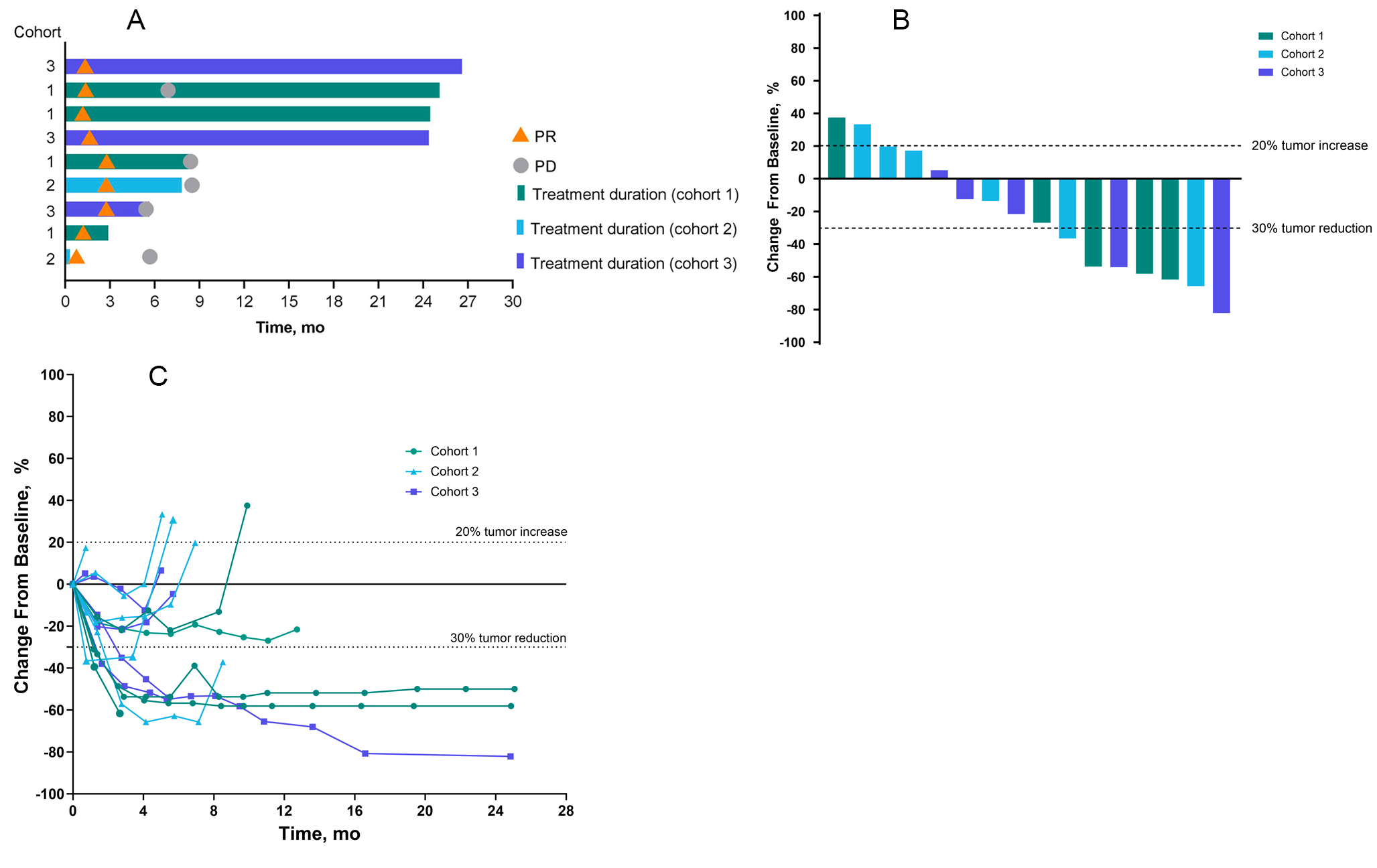
Tumor assessments were performed on Day 29 and every 8 weeks thereafter for the initial 12 cycles, regardless of any dose interruptions or dose delays, and then performed per local standard practice after completion of Cycle 12. Tumor assessments were repeated at the end of study visit if more than 6 weeks had passed since the last evaluation. Unconfirmed objective response by investigator assessment was defined as a complete (disappearance of all target lesions) or partial (at least 30% decrease in the sum of diameters of target lesions) response recorded from Cycle 1 Day 1 until disease progression, start of subsequent anticancer therapy, or death due to any cause. Given the exploratory nature of the efficacy endpoint, confirmation of response was not required. Duration of response, calculated as the time from first documentation of complete response or partial response to date of first documentation of objective progression or death, was only calculated for the subgroup of patients with an unconfirmed objective response.
Statistical analyses
All patients who had received at least 1 dose of talazoparib were included in the safety and efficacy analysis sets. All treated patients with at least 1 PK concentration in the single-dose and/or multiple-dose PK part were included in the PK concentration analysis set, and all treated patients with at least 1 of the PK parameters of primary interest in the single-dose and/or multiple-dose PK part were included in the PK parameter analysis set. All patients in the PK parameter analysis set who completed both the single-dose PK and multiple-dose PK parts without major protocol deviations were included in the PK evaluable analysis set.
Talazoparib PK parameters were calculated for each patient and each treatment, as applicable, using non-compartmental analysis of concentration-time data. Summary statistics were calculated by setting concentration values below the lower limit of quantification to zero.

留言 (0)