
記住我

Advancement in technology in the last decade and the pursuit of patient comfort and acceptability have resulted in an abundance of commercially available devices to measure blood pressure (BP) without the need of a pneumatic cuff [1,2]. Cuffless wearable BP devices have the potential to provide thousands of BP readings over weeks and months, without significant user awareness and disturbance. The potential of cuffless devices seems superior to conventional out-of-office methods, such as ambulatory (ABPM) and home BP monitoring (HBPM), in their ability to provide a more complete BP profile. Furthermore, for users they are generally more comfortable to wear than cuff-based monitors, making them far more acceptable [3].
Cuffless devices therefore have the potential to supersede conventional BP monitoring methods, but only once their accuracy has been established [4]. Accuracy of BP measuring devices is usually determined through a careful validation process. However, the established validation procedure for cuff BP devices is not suitable for cuffless devices [4]. We refer here to the Association for the Advancement of Medical Instrumentation/ European Society of Hypertension/ International Organization for Standardization (AAMI/ESH/ISO) Universal Standard (ISO 81060-2:2018) [5], which does not include a procedure to track BP changes as this is not an issue with cuff BP devices. For cuffless BP devices, pressure is estimated from a surrogate measure, which is usually calibrated at rest with no guarantee the calibration would be valid at other levels of blood pressure. When commercial entities thus employ this standard to validate cuffless devices, it will lead to misleading conclusions [6]. In a recent statement by the ESH Working Group on Blood Pressure Monitoring and Cardiovascular Variability on cuffless BP measuring devices, it is highlighted that the validation of cuffless devices should focus on very specific aspects, such as their ability to track BP changes [4]. In this study, we therefore evaluated the performance of the commercially available wrist-worn Aktiia cuffless wearable device (Switzerland) in tracking BP changes in a day-to-day setting. We determined whether the Aktiia tracks 24-h systolic and diastolic BP (SBP, DBP) compared to conventional ABPM; and antihypertensive medication-induced BP changes when compared to cuff-based HBPM.
METHODSWe recruited outpatients attending the Hypertension Center STRIDE-7 (Athens, Greece) and the Dobney Hypertension Centre (Perth, Australia) from November 2021 to April 2022. Inclusion criteria were male or female, age 18–80 years, BP in the normotensive or hypertensive range (treated and untreated), and absence of co-morbidities. Those with a history of arrhythmias, average office BP ≥180/110 mmHg, inter-arm BP difference of >10 mmHg, and shift workers or habitual siesta takers were excluded from the study. For the study investigating the detection of circadian BP with cuffless BP monitoring as compared to classic ABPM, we recruited untreated individuals or treated individuals on stable BP treatment. For the study investigating the detection of medication-induced changes in BP with cuffless BP monitoring as compared to HBPM, we recruited outpatients who required uptitration of antihypertensive therapy. The study protocol was approved by the Human Research Ethics Committee from each of the institutions involved in this study and written consent was obtained from all participants.
Study protocolParticipants underwent a physical examination and a brief medical history was undertaken. After 5 min of seated rest, attended automated office BP was taken with a validated oscillometric device (WatchBP Office; Microlife, Widnau, Switzerland) on both arms, simultaneously, in triplicate at one-minute intervals. The mean of the second and third measurements was used as the final BP reading. The arm with higher BP was selected for future office BP measurements. Participants were fitted with the cuffless wearable BP device (Aktiia Bracelet G1; Aktiia SA, Neuchatel, Switzerland) on their dominant wrist. Initialization (calibration) of the Aktiia was then performed according to manufacturer instructions through Bluetooth connection using the Aktiia App installed onto a mobile phone of the centers. During this process, the wrist-worn device was calibrated with brachial cuff BP measured on the nondominant arm using the manufacturer-supplied automated, oscillometric BP monitor (Aktiia Init I1, Aktiia SA).
Protocol for tracking 24-h BP changesParticipants were instructed to wear the Aktiia continuously, except in the shower or bath, for 6–12 days. Classic ABPM (WatchBP O3; MicroLife) was performed on the first and last 24 h of cuffless BP monitoring at 20-min intervals throughout both day and night. ABPM was repeated in order to increase sensitivity due to challenges in ABPM reproducibility [7]. The ABPM cuff was fitted on the nondominant arm. Participants were required to visit the clinic for both ABPM device fitting and removal. The Aktiia was removed on the last study visit and BP readings were synchronized with the online Aktiia secure server via the Aktiia App.
Protocol for tracking medication-induced BP changesParticipants were instructed to wear the Aktiia continuously for three weeks, except in the shower or bath. Calibration with the upper-arm cuff was performed once at the beginning of the study during the first study visit. Participants also performed HBPM every day for three weeks (Omron HEM-7121; Omron Healthcare Co. Ltd, Kyoto, Japan). They recorded home BP twice in the morning before medications and in the evening, after five minutes of seated rest and with one-minute interval between each BP measurement, using a diary sheet. Participants remained on their original antihypertensive therapy for the first week of the study. BP medication was uptitrated at the start of the second week, and participants were instructed to continue wearing the Aktiia and perform HBPM during the second and third week.
Cuffless blood pressure monitoringThe Aktiia is a CE-marked Class IIa medical device which is available on the market and uses an optical signal (photoplethysmography) measured on the back of the wrist to estimate BP. Measurement is automatically triggered, yet measurements are taken only when the device detects that the user is still. The measured optical signals are stored in the Aktiia device until synchronized with the Aktiia server through the Aktiia App. A proprietary pulse wave analysis algorithm is used to retrospectively process the optical data and produce estimates of BP.
Statistical analysisAll statistical analyses were performed in R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria). A P value of <0.05 was considered statistically significant. Data are presented as mean ± standard deviation (SD) unless otherwise specified.
Tracking 24-h BP changesTo compare 24-h BP monitoring, we calculated daily time-weighted (average of hourly mean values) 24-h, daytime, and night-time BP values and averaged these across the total study days for cuffless BP (ranging from 6 to 12 days) and across the two 24-h periods for ambulatory BP during which ABPM was performed. For both cuffless BP and ambulatory BP, daytime and night-time BP were determined based on self-reported sleep and awake times in the participants’ activity diaries. Comparisons of 24-h, daytime, and night-time BP between cuffless BP and ambulatory BP were made using paired Student's t-tests. We also created Bland-Altman plots [8] to compare averaged BP on days when both Aktiia and ABPM readings were available. McNemar's chi-squared test was used to compare the proportion of night-time BP dippers (defined as night-time decline in both SBP and DBP >10% relative to daytime BP) as classified by Aktiia or ABPM. The reproducibility of ABPM in this study was further assessed using Bland-Altman analysis and standard deviation of the mean differences (SDD) between the two visits.
Tracking medication-induced BP changesThe data for only three participants were available, hence individual participant data are presented. We used the daytime average BP (0700 to 2259 h) as measured by the Aktiia for comparison with HBPM. The daily cuff-based home BP readings were averaged across the two to four measurements recorded by the participants.
RESULTS Tracking 24-h BP changesA total of 60 outpatients were recruited across the two hypertension centers. After exclusions (Figure S1, Supplemental Digital Content, https://links.lww.com/HJH/C175), a total of 41 participants (age 58 ± 14 years, 32% females, 80% hypertension) were included in the final data analysis (Table 1). Five participants did not have a repeat ABPM, but exclusion of these participants did not affect the overall results (data not shown).
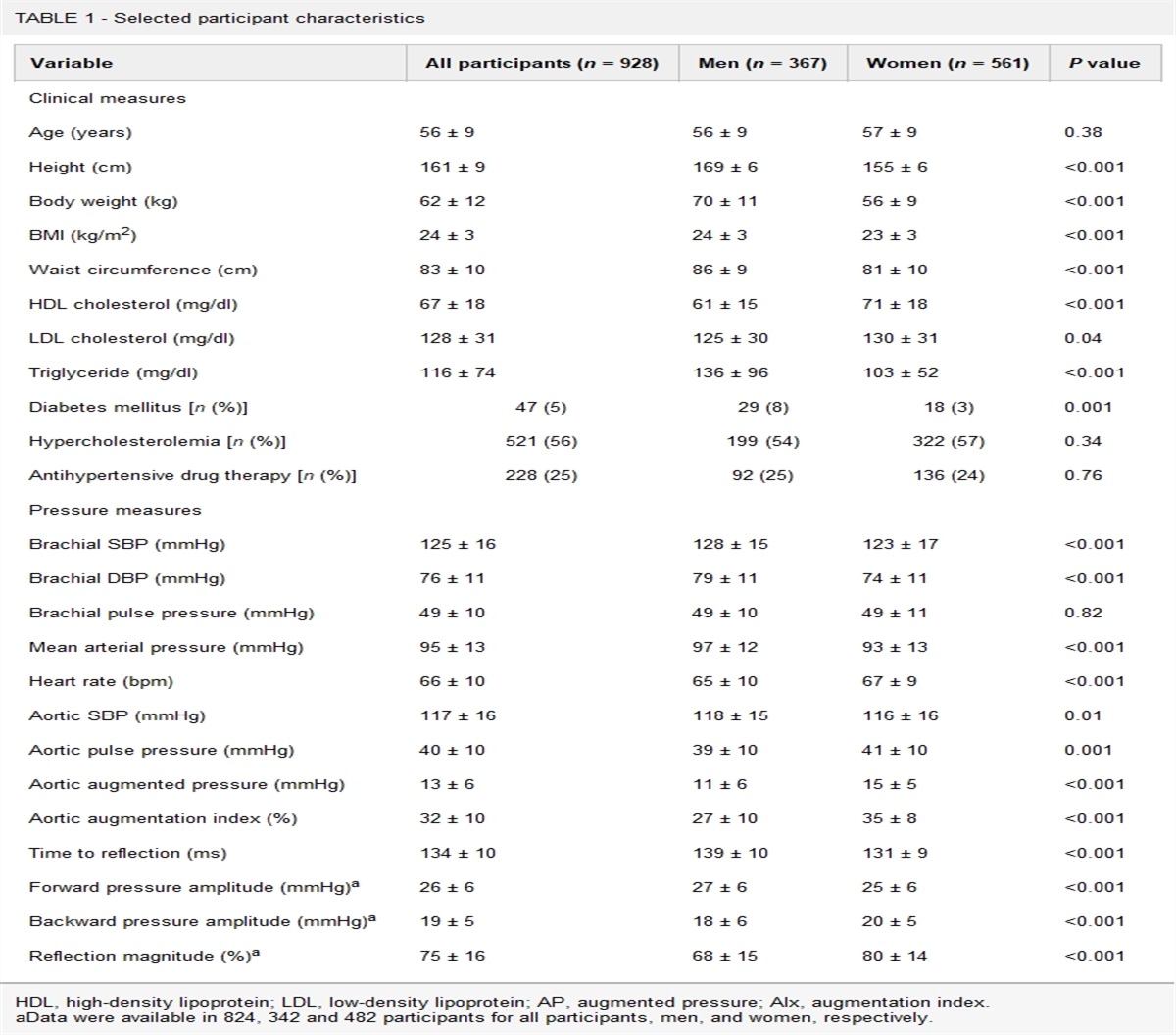
TABLE 1 - Participants included in the 24-h BP tracking study (N = 41) Mean ± SD Baseline characteristics Age, years 58 ± 14 Females, N (%) 13 (32) Height, cm 173 ± 8 Weight, kg 83.7 ± 15.0 Body mass index, kg/m2 27.9 ± 4.1 Clinic systolic blood pressure, mmHg 130 ± 13 Clinic diastolic blood pressure, mmHg 79 ± 9 Clinic heart rate, bpm 71 ± 13 Medical history Hypertension, N (%) 33 (80) Hypercholesterolemia, N (%) 25 (61) Smoking history, N (%) 14 (34) Medication Angiotensin receptor blockers, N (%) 34 (83) Diuretics, N (%) 10 (24) Calcium channel blockers, N (%) 25 (61) Other antihypertensives, N (%) 9 (22) Statins, N (%) 27 (66)Participants had an average 24-h BP of 121 ± 10/73 ± 7 mmHg, daytime BP of 127 ± 11/78 ± 8 mmHg, and night-time BP of 108 ± 10/63 ± 6 mmHg as measured by classic ABPM. The average night-time dip was −19.7 ± 7.4 mmHg (−14.6 ± 6.3%) for SBP and −14.4 ± 5.6 mmHg (−17.9 ± 7.5%) for DBP (Table 2). When comparing the average 24-h, daytime and night-time SBP and DBP differences between the Aktiia and classic ABPM (Table 2, Table S1, Supplemental Digital Content, https://links.lww.com/HJH/C175), the Aktiia showed higher 24-h and night-time BP (all P ≤ 0.002), but similar daytime SBP (P = 0.48) and DBP (P = 0.13) (Fig. 1a). Aktiia reported reduced night-time dip for SBP and DBP (both P < 0.001) as compared to ABPM. Seven out of 41 (17.1%) participants were classified as nondippers by ABPM, and 40 out of 41 (97.6%) participants were classified as nondippers by Aktiia (P < 0.001).
TABLE 2 - Weighted mean 24-h, daytime, and night-time BP as obtained by cuffless BP monitoring and classic ABPM (N = 41) Aktiia ABPM Difference [95% CI] P Cuffless monitoring (6–12 days) vs. ABPM (2 days) Systolic blood pressure (mmHg) 24-h 126 ± 13 121 ± 9 4.9 [1.9, 7.9] 0.002 Daytime 128 ± 13 127 ± 11 1.0 [−1.8, 3.8] 0.48 Night-time 124 ± 14 108 ± 9 15.5 [11.8, 19.1] <0.001 Night-time dip −4.8 ± 4.1 −19.7 ± 7.4 14.2 [12.1, 16.3] <0.001 Night-time dip (%) −3.8 ± 3.3 −14.7 ± 5.4 11.0 [9.4, 12.5] <0.001 Diastolic blood pressure (mmHg) 24-h 77 ± 9 73 ± 7 4.2 [2.3, 6.0] <0.001 Daytime 79 ± 9 78 ± 8 1.4 [−0.4, 3.2] 0.13 Night-time 75 ± 9 63 ± 6 11.8 [9.5, 14.1] <0.001 Night-time dip −4.1 ± 2.7 −14.4 ± 5.6 10.2[8.6, 11.9] < 0.001 Night-time dip (%) −5.3 ± 3.5 −18.2 ± 6.5 12.9 [11.0, 14.8] <0.001 Cuffless monitoring vs. ABPM (devices worn simultaneously) Systolic blood pressure (mmHg) 24-h 126 ± 14 121 ± 10 5.3 [2.2, 8.5] 0.002 Daytime 128 ± 13 127 ± 11 1.1 [−1.8, 4.0] 0.45 Night-time 123 ± 15 108 ± 10 15.3 [11.4, 19.2] <0.001 Night-time dip −4.9 ± 5.2 −18.8 ± 8.7 14.2 [12.1, 16.2] <0.001 Night-time dip (%) −3.9 ± 4.2 −14.6 ± 6.3 10.9 [9.3, 12.4] <0.001 Diastolic blood pressure (mmHg) 24-h 77 ± 9 73 ± 7 4.7 [2.8, 6.6] <0.001 Daytime 79 ± 9 78 ± 8 1.8 [0.0, 3.7] 0.05 Night-time 75 ± 10 63 ± 7 11.9 [9.6, 14.3] <0.001 Night-time dip −4.2 ± 3.4 −14.1 ± 6.4 10.1 [8.5, 11.7] <0.001 Night-time dip (%) −5.4 ± 4.4 −17.9 ± 7.5 12.8 [11.0, 14.5] <0.001Bold denotes statistical significance, P < 0.05.ABPM, ambulatory blood pressure monitoring.
 FIGURE 1:
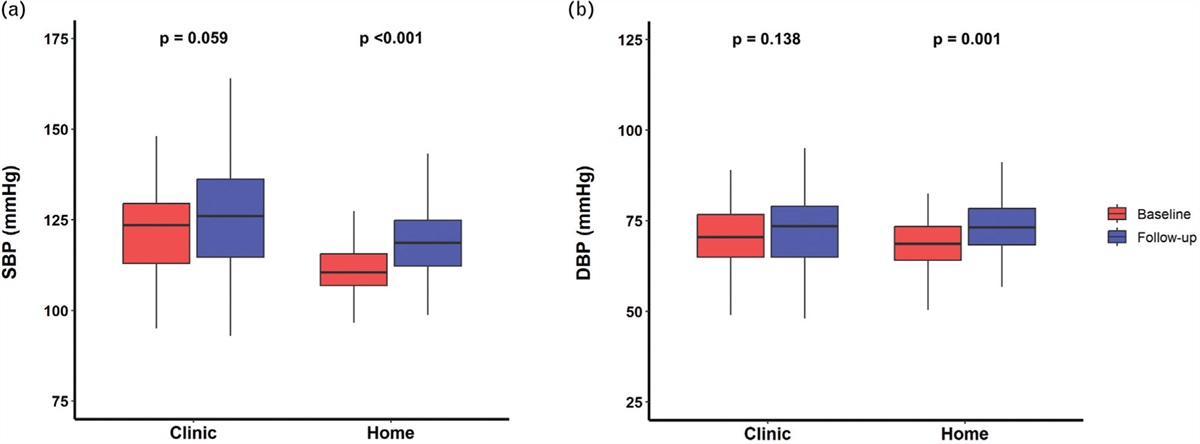
FIGURE 1: Comparison of BP tracking across 24-h with classic ABPM (open circles) vs. cuffless Aktiia (black dots) (n = 41). (a) The weighted average 24-h, daytime and night-time BP with ABPM (2 days) vs. Aktiia (6–12 days). (b) The 24-h profile comparison per hour (bars represent 95% CI).
The 24-h BP profiles as obtained by Aktiia and ABPM showed concordant BP values between 0700 to 1900 h, from which point the two started to diverge until approximately 0300 h before converging again (Fig. 1b). When comparing the 24-h BP profiles based on hours before/after sleep onset, discordance between Aktiia BP and ABPM BP was observed a few hours before sleep onset (Figure S3, Supplemental Digital Content, https://links.lww.com/HJH/C175). This pattern was consistently observed regardless of whether we compared BP across 6–12 days with cuffless vs. 2 days with ABPM (Table 2, Fig. 1b), or only on days when devices were worn simultaneously (Table 2, Figure S2B, Supplemental Digital Content, https://links.lww.com/HJH/C175). The range of total number of Aktiia BP readings for each participant over the period of device wear is shown in Figure S4, Supplemental Digital Content, https://links.lww.com/HJH/C175, and the total number of Aktiia BP and ABPM readings is shown in Table S2, Supplemental Digital Content, https://links.lww.com/HJH/C175.
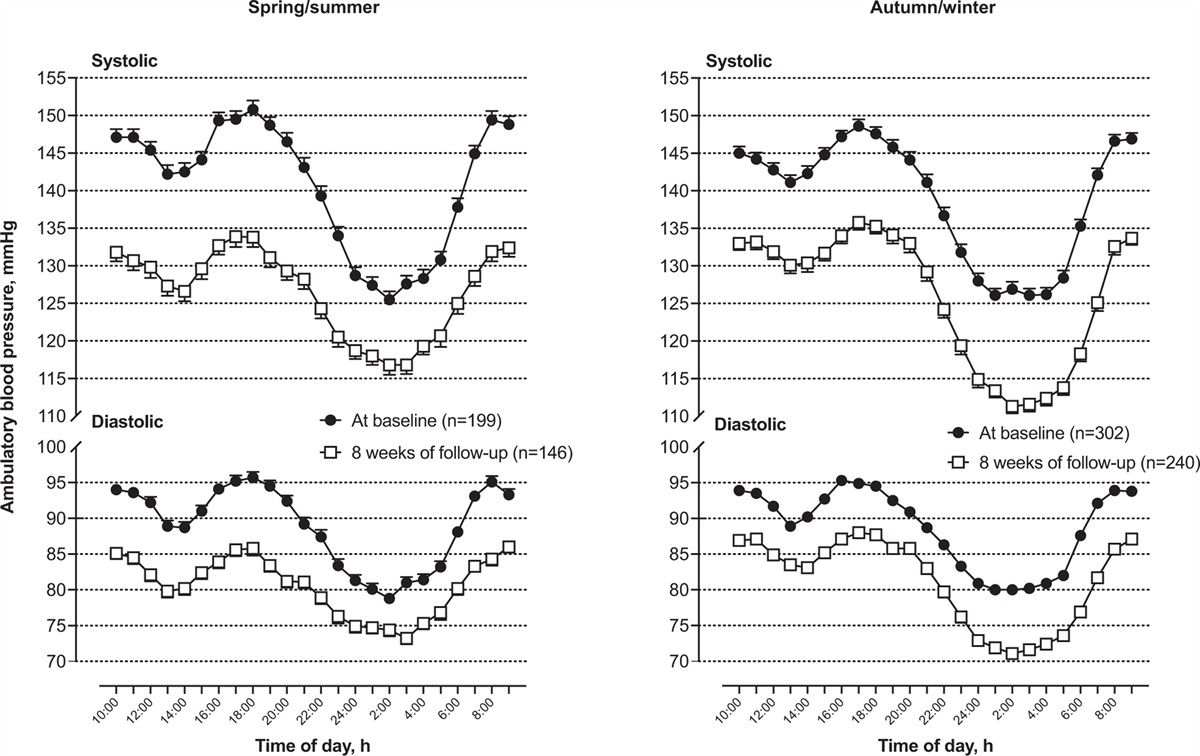
We determined bias and 95% limits of agreement with Bland-Altman plots between Aktiia and ABPM readings for average 24-h, daytime, and night-time BP on days when Aktiia and ABPM devices were worn simultaneously (Fig. 2). The mean bias and limits of agreement for 24-h SBP was 5.3 [–14.4; 25.0] mmHg, for daytime SBP 1.1 [–17.0; 19.2] mmHg, and for night-time SBP +15.3 [–8.7, 39.3] mmHg. For DBP, the pattern was similar, with the mean bias and limits of agreement of 24-h DBP being 4.7 [–7.2; 16.6] mmHg, daytime DBP 1.8 [–9.5; 13.2] mmHg and night-time DBP 11.9 [–2.6; 26.5] mmHg. We also performed the same analysis on the hourly averaged BP readings for hours where both Aktiia and ABPM readings were available, with similar results (Figure S5, Supplemental Digital Content, https://links.lww.com/HJH/C175).
 FIGURE 2:
FIGURE 2: Bland–Altman plots comparing the average 24-h, daytime and night-time BP between classic cuff ABPM and Aktiia cuffless BP (n = 41).
Reproducibility of SBP/DBP between the two ABPM performed (N = 37) was 6.8/5.0 mmHg (SDD) for 24-h, 7.1/4.9 mmHg for daytime, and 7.2/5.0 mmHg for night-time. The limits of agreement between the two ABPM were [−13.3; +13.2] mmHg for 24-h SBP and [−9.7; +9.8] mmHg for 24-h DBP; [−14.4; +13.5] mmHg for daytime SBP and [−9.5; +9.8] for daytime DBP; [−11.4; 16.9] mmHg for night-time SBP and [−9.3; +10.7] mmHg for night-time DBP.
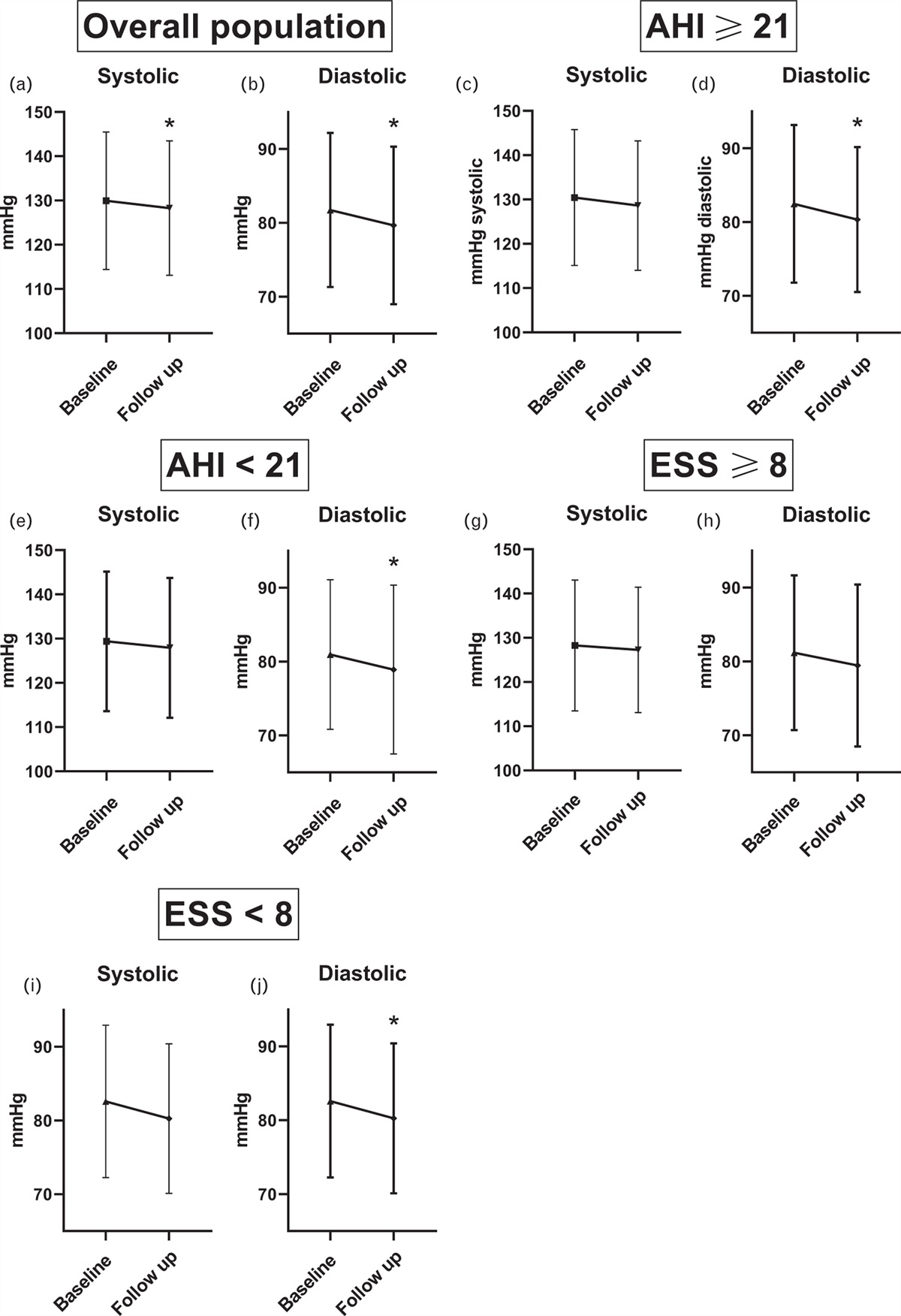
Tracking medication-induced BP changesWe recruited eight participants requiring antihypertensive medication uptitration from the Dobney Hypertension Centre (Perth, Australia). Two participants did not complete the study due to irritation with the wrist device (n = 1) or without reason (n = 1), and three participants had no Aktiia readings recorded, resulting in three participants (age 60 ± 8 years, 1 female) with complete study data. Due to the small sample size, individual results are presented in Fig. 3. We noted consistent results across participants, with a downward trend in home BP readings across the 21 days, compared to Aktiia daytime BP readings that remained unchanged throughout the same time period, and without additional cuff calibration after initial setup. Table S3, Supplemental Digital Content, https://links.lww.com/HJH/C175 shows the weekly average BP at baseline (first week of measurement, prior to medication uptitration) and over the two weeks post medication uptitration. The average medication-induced lowering in SBP and DBP for the three participants from week 1 to 3 for the Aktiia was −1.0/−0.8 mmHg vs. −19.7/−11.5 mmHg with classic HBPM (P < 0.03 for SBP difference and P = 0.04 for DBP difference).
 FIGURE 3:
FIGURE 3: Tracking BP medication-induced changes in systolic and diastolic BP in three participants with cuffless Aktiia (black dots) vs. classic home BP monitoring (HBPM). Dashed line indicates medication uptitration.
DISCUSSIONThis study evaluated the ability of the wrist-wearable cuffless BP device, Aktiia, to track BP changes against conventional out-of-office cuff BP measurement methods. We showed that despite comparable daytime BP, the cuffless method did not adequately track the BP decline during night-time sleep when compared to conventional cuff-based ABPM. Our study results also suggested that the cuffless device did not adequately track antihypertensive medication-induced BP lowering when compared with cuff-based HBPM. Previous studies by the developers of Aktiia [9–12] report accuracy when validating the device after cuff BP calibration in the sitting position according to an adapted ISO81060-2 protocol for cuff devices [10], accuracy in the most common body positions [9], and accurate tracking of BP changes in a case study when taking antihypertensive medication [12], – concluding that the Aktiia can be recommended for BP measurement in the adult population [10]. Yet, recently they also reported that conventional ABPM demonstrated a 3.4 times larger night-time dipping than the Aktiia device [11], which align with our findings. The question thus is, can the Aktiia device be recommended for BP measurement in adults?
There is now a plethora of cuffless BP devices available on the market. In the online marketplace in Australia, the number of wrist wearables (N = 532) exceed that of cuff devices (N = 440) for sale – despite a lack of evidence of validation for accuracy of wearable devices [13]. An increasing number of papers claim to be ‘validation studies’ despite the fact that, to date, none have followed the recommended guidelines from Institute of Electrical and Electronic Engineers (IEEE) standard for wearable, cuffless measuring BP devices [6]. An ISO 81060-3 standard is currently under development [4] – yet, due to the heterogenous technologies used by cuffless manufacturers, there are major challenges. From the perspective of technological companies, this poses a frustrating situation on how to prove unequivocally that a new device is indeed accurate. Due to this challenge, we therefore focused on clinical utility in this study as the ability of a cuffless device to accurately track BP changes over time is essential for clinical decision making.
Tracking 24-h BP changesIn our sample of 41 adults, we demonstrated a significant deviation in the ability to track night-time SBP and DBP dipping of the Aktiia device, reporting a mean difference of 15.5/11.8 mmHg compared to cuff-based ABPM. Based on results from the Aktiia, the majority of participants (97% vs. 17%) were incorrectly categorized as nondippers. For daytime BP, however, the mean SBP and DBP values showed acceptable clinical agreement between the methods (+1.1 mmHg). Bland–Altman plots comparing Aktiia and ABPM daytime BP (Aktiia and ABPM worn simultaneously) indicated wide limits of agreement [–17.0; +19.2] mmHg for SBP and [–9.5; +12.2] mmHg for DBP, which are aligned with findings from a meta-analysis on short-term reproducibility of repeat ABPMs in 35 studies ([–16.7; +18.4] mmHg for daytime SBP and [–10.4; +12.3] mmHg for daytime DBP) [7], but slightly wider than the reproducibility of the repeat ABPM in this study ([−14.4; +13.5] mmHg for daytime SBP and [–9.5; +9.1] mmHg for daytime DBP). The limits of agreement for 24-h and night-time BP would have been narrower between the Aktiia and ABPM, were it not for the significant difference in night-time BP tracking. The inability to track BP changes over 24 h is not unique to the Aktiia device, but may be a limitation shared by other cuffless wearable devices that have also been shown to have greater discrepancies at night-time than daytime when compared against ABPM [14,15]. This study was not designed to provide clarity on the discrepancy between daytime and night-time BP, but it would be critical for developers to understand and establish the underlying factors that preclude tracking of night-time BP. It is unclear whether the more comparable daytime BP estimation is due a heavy reliance on the input of cuff-based BP calibration. For this reason, we also evaluated daytime BP changes in response to uptitration of antihypertensive treatment.
Tracking medication-induced BP changesDespite including only three participants, these pilot observations were consistent with the results from tracking 24-h BP changes, with the Aktiia device being unable to adequately detect BP changes induced by dosage increase of antihypertensive medication. Despite potential anxiety due to cuff inflation [16], HBPM showed a consistent lowering in BP across the two weeks of observation from time of medication uptitration, albeit with varying degrees of BP reduction across the three individuals. On the contrary, the Aktiia BP readings showed little to no change over the two weeks in each individual (overall change in SBP/DBP of Aktiia vs. HBPM –1.0/–0.8 vs. –19.7/–11.5 mmHg). It is acknowledged that reporting bias from participants may exist from handwritten diaries of home BP measurements and thus electronic data capture from the device would have been ideal. However, participants were not instructed to install the manufacturer's accompanying app for data syncing purposes, and the monitor could only store 30 measurements, thus it was not possible to obtain the electronic data from the devices.
Tracking BP changes using cuffless methodsAs previously mentioned, the apparent inability to track BP changes over time is not a limitation of the Aktiia device alone but may be a limitation shared amongst other currently available cuffless BP devices. One plausible explanation is the reliance of cuffless BP devices on an initial calibration that is often only performed at resting BP using a conventional cuff-based BP device. Subsequent BP measurements are thus relative to the preceding cuff-based measurement value [6], which may be within acceptable limits for smaller changes in BP (e.g. during normal daytime variations) but not over large changes in BP (e.g. with normal night-time decline, exercise, or antihypertensive medication). However, it is beyond the scope of the present study to investigate the possible technological or physiological factors that contribute to a cuffless device's ability (or inability) to track BP changes.
In conclusion, cuffless wearable devices have considerable potential to improve hypertension management, but only once accuracy and clinical usefulness have been demonstrated. The commercially available wrist-worn Aktiia cuffless wearable device lacked the key function required for clinical management, namely the ability to track changes in brachial BP during sleep or with drug treatment in a similar fashion as conventional cuff-based methods. While awaiting a new ISO standard which is specific for validating cuffless devices, studies are encouraged to evaluate the ability of wearable devices to track changes in BP, as opposed to just validating the devices at resting or calibration BP.
ACKNOWLEDGEMENTSThe authors thank the participants and technical staff for taking part in this investigation.
Previous presentations: Results from this paper were previously presented at the following scientific meetings: 2022 American Heart Association Hypertension meeting; 2022 International Society of Hypertension meeting
Funding sources: The study was funded through a Program Grant of the National Health and Medical Research Council (NHMRC) of Australia.
Conflicts of interestAktiia SA (Switzerland) provided the devices at no cost for the purpose of this study but had no input in the design or conduct of this investigation. A.E.S. received speaker honoraria from Aktiia and Omron. G.S.S. has received consulting fees by Aktiia and Microlife and lecture fees by Aktiia. IT was previously employed by AtCor Medical Pty. Ltd, a subsidiary of CardieX Ltd, developer of blood pressure monitoring devices and health wearables.
REFERENCES 1. Schutte AE, Kollias A, Stergiou GS. Blood pressure and its variability: classic and novel measurement techniques. Nat Rev Cardiol 2022; 19:643–654. 2. Schutte AE. The promise and pitfalls of novel cuffless blood pressure devices. Eur Heart J 2022; 43:4222–4223. 3. Gnanenthiran SR, Liu H, Tan I, Chan J, Schlaich MP, Schutte AE. Cuffless blood pressure devices: the gap between patient acceptability and need for validation. J Hypertens 2022; 40:2317–2319. 4. Stergiou GS, Mukkamala R, Avolio A, Kyriakoulis KG, Mieke S, Murray A, et al. Cuffless blood pressure measuring devices: review and statement by the European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability. J Hypertens 2022; 40:1449–1460. 5. Stergiou GS, Alpert B, Mieke S, Asmar R, Atkins N, Eckert S, et al. A universal standard for the validation of blood pressure measuring devices: Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) collaboration statement. Hypertension 2018; 71:368–374. 6. Mukkamala R, Yavarimanesh M, Natarajan K, Hahn JO, Kyriakoulis KG, Avolio AP, et al. Evaluation of the accuracy of cuffless blood pressure measurement devices: challenges and proposals. Hypertension 2021; 78:1161–1167. 7. Bo Y, Kwok KO, Chung VC, Yu CP, Tsoi KK, Wong SY, et al. Short-term reproducibility of ambulatory blood pressure measurements: a systematic review and meta-analysis of 35 observational studies. J Hypertens 2020; 38:2095–2109. 8. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1:307–310. 9. Sola J, Vybornova A, Fallet S, Polychronopoulou E, Wurzner-Ghajarzadeh A, Wuerzner G. Validation of the optical Aktiia bracelet in different body positions for the persistent monitoring of blood pressure. Sci Rep 2021; 11:20644. 10. Vybornova A, Polychronopoulou E, Wurzner-Ghajarzadeh A, Fallet S, Sola J, Wuerzner G. Blood pressure from the optical Aktiia Bracelet: a 1-month validation study using an extended ISO81060-2 protocol adapted for a cuffless wrist device. Blood Press Monit 2021; 26:305–311. 11. Sola J, Cortes M, Perruchoud D, De Marco B, Lobo MD, Pellaton C, et al. Guidance for the interpretation of continual cuffless blood pressure data for the diagnosis and management of hypertension. Front Med Technol 2022; 4:899143. 12. Sola J, Sibylle F, Gregoire W. Monitoring the personalised effects of antihypertensive drugs using the Aktiia optical device: a 4-month follow-up. Cardiovasc Med 2021; 24:w10054. 13. Picone DS, Deshpande RA, Schultz MG, Fonseca R, Campbell NRC, Delles C, et al. Nonvalidated home blood pressure devices dominate the online marketplace in Australia: major implications for cardiovascular risk management. Hypertension 2020; 75:1593–1599. 14. Nyvad J, Christensen KL, Buus NH, Reinhard M. The cuffless SOMNOtouch NIBP device shows poor agreement with a validated oscillometric device during 24-h ambulatory blood pressure monitoring. J Clin Hypertens (Greenwich) 2021; 23:61–70. 15. Miranda Hurtado M, Reyes Vasquez J, Rodriguez-Fernandez M. Comparison of a tonometric with an oscillometric blood pressure monitoring device over 24 h of ambulatory use. Blood Press Monit 2021; 26:149–155. 16. Xie F, Wu Y, Liu H, Yu Z, Xu J, Su H. Anxiety is associated with higher blood pressure rise induced by cuff inflation. Blood Press Monit 2022; 27:168–172.
留言 (0)