PNETs account for less than 5% of all pancreatic tumors, and although resection is the treatment of choice in principle, PNETs are known to recur frequently after surgery. Dong et al. reported that 154 (15.1%) of 1,020 postoperative patients with PNET experienced recurrence, with the liver (n = 76, 49.4%) and pancreas (n = 35, 22.7%) being the primary sites of recurrence [3]. In the same paper, it was reported that about half the recurrences occurred within 2 years after surgery but could also occur even after almost 10 years. Similarly, Kim et al. also reported cases of liver metastases recurrence more than 10 years after surgery, suggesting the need for long-term postoperative follow-up [4]. In the present case, liver metastasis was suspected 6 months after surgery, but there were no malignant findings. After continuous follow-up, an increasing trend toward recurrence was observed 12 years later. A lesion that was initially found 6 months post-surgery was later found to be an enlarging neoplasm after 10 years. To date, this has never been reported; this, however, suggests that slow-growing tumors may exist in PNETs even after malignancy has been ruled out.
Careful follow-up is important to avoid missing the optimal timing of resection. Tumor markers should be measured every 3 months, and imaging studies should be performed every 6 months during the first 2 years, and then every year thereafter [5]. It has been reported that follow-up is necessary for at least 10 years because recurrence may occur after a long period [5]. In the present case, recurrence happened more than 10 years after primary resection, and radical resection was still possible with the diagnosis of recurrence. While many cases recur soon after surgery, some recur after a longer timeframe, and careful long-term follow-up should be done to avoid missing the opportunity for resection, especially if recurrence is suspected on the postoperative follow-up examination.
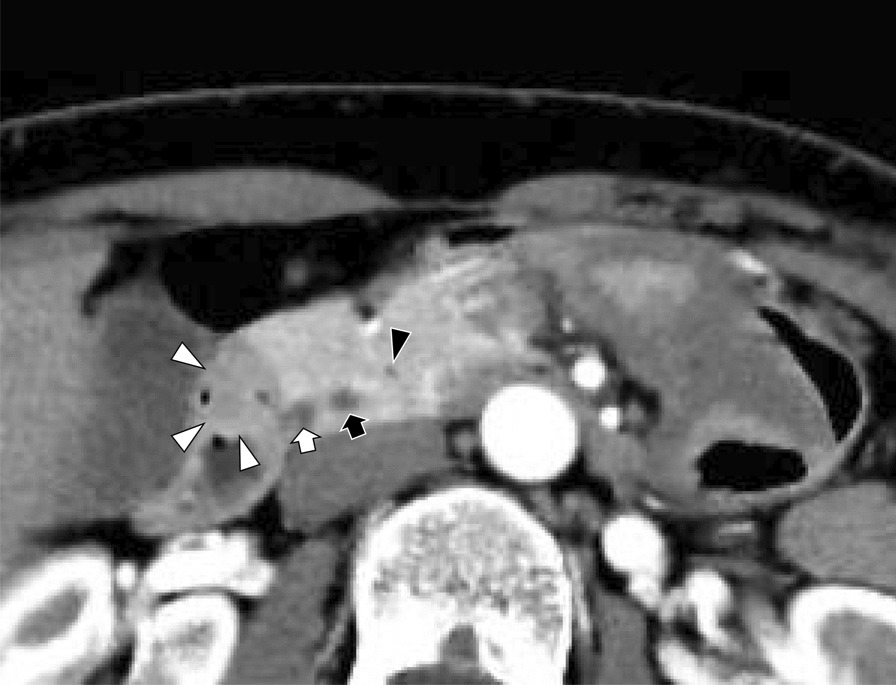
When the development of schwannoma is observed during the postoperative follow-up of a malignant tumor, a definitive diagnosis is difficult. Although differential diagnoses for GIS include GIST, NET, leiomyoma, leiomyosarcoma, and adenocarcinoma, it is difficult to confirm these diagnoses through imaging studies alone. GIS appear as well-defined homogenous tumors with low enhancement on CT compared to the heterogeneous appearance of GIST or the obscure characteristics of adenocarcinoma. However, these features are not highly specific [6]. CT has been reported to have a sensitivity of 61–90%, specificity of 90–92%, and accuracy of 58–90% in the diagnosis of NET metastases [7,8,9,10]. It is difficult to distinguish NETs from CTs alone. Unlike highly differentiated NETs, many cases of schwannoma show increased accumulation on FDG-PET/CT. However, it is difficult to distinguish benign from malignant tumors, and it is also not possible to distinguish between GIS and NETs [6]. SRS for NETs is highly specific (93%), but it is neither sensitive (52%), nor accurate (58%) [8]. Additionally, it is not possible to distinguish between GIS and NETs if SRS is negative. Many cases could not be definitively diagnosed even when multiple modalities were used. Therefore, a histopathological examination is required for a definitive diagnosis. In this case, although CT showed findings suspicious for GIS and NET, FDG-PET/CT did not show typical findings of schwannoma, and SRS did not lead to the diagnosis of NET. Imaging alone could not distinguish between peritoneal dissemination of NETs and GIS, and histopathological examination was required.
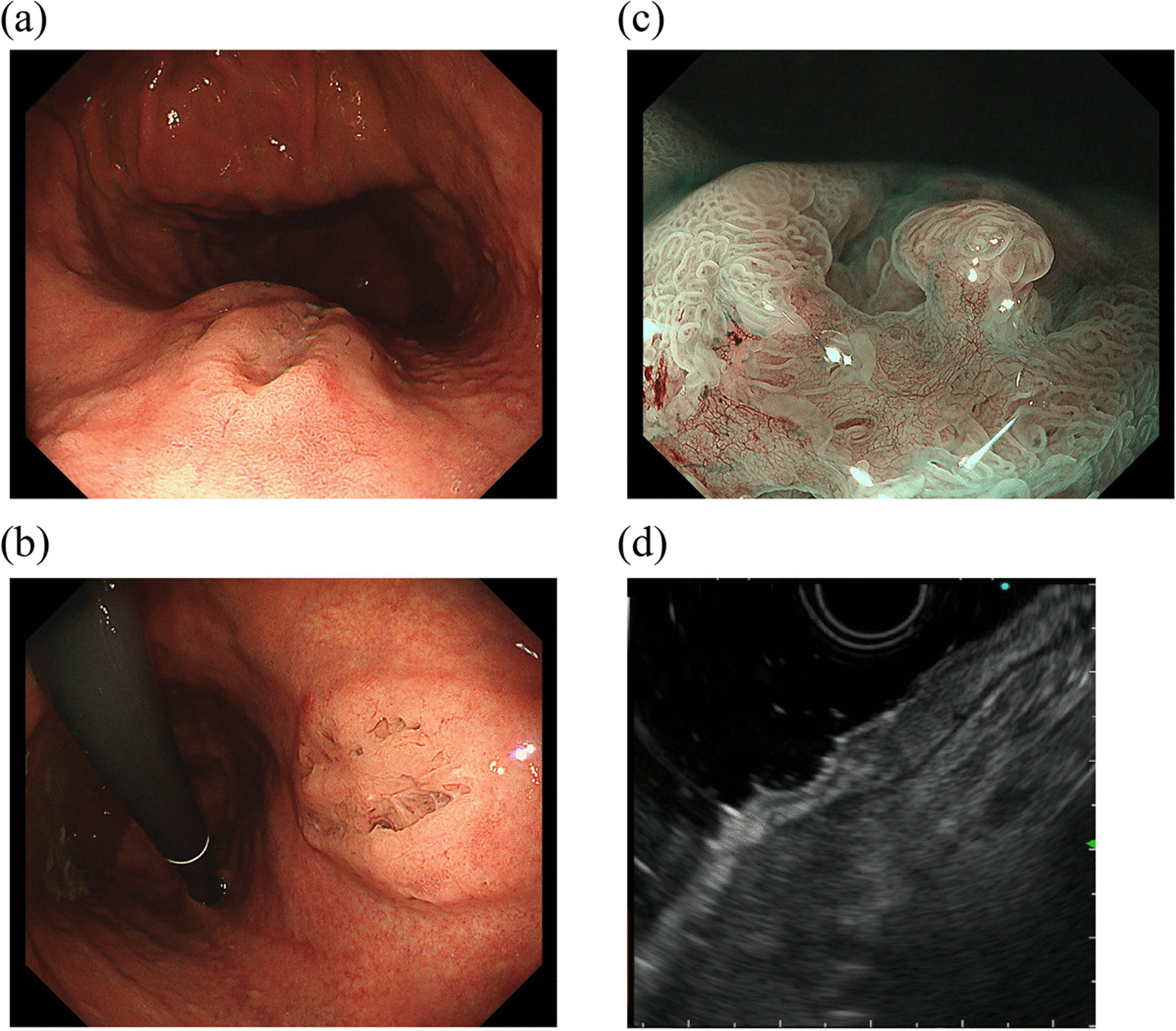
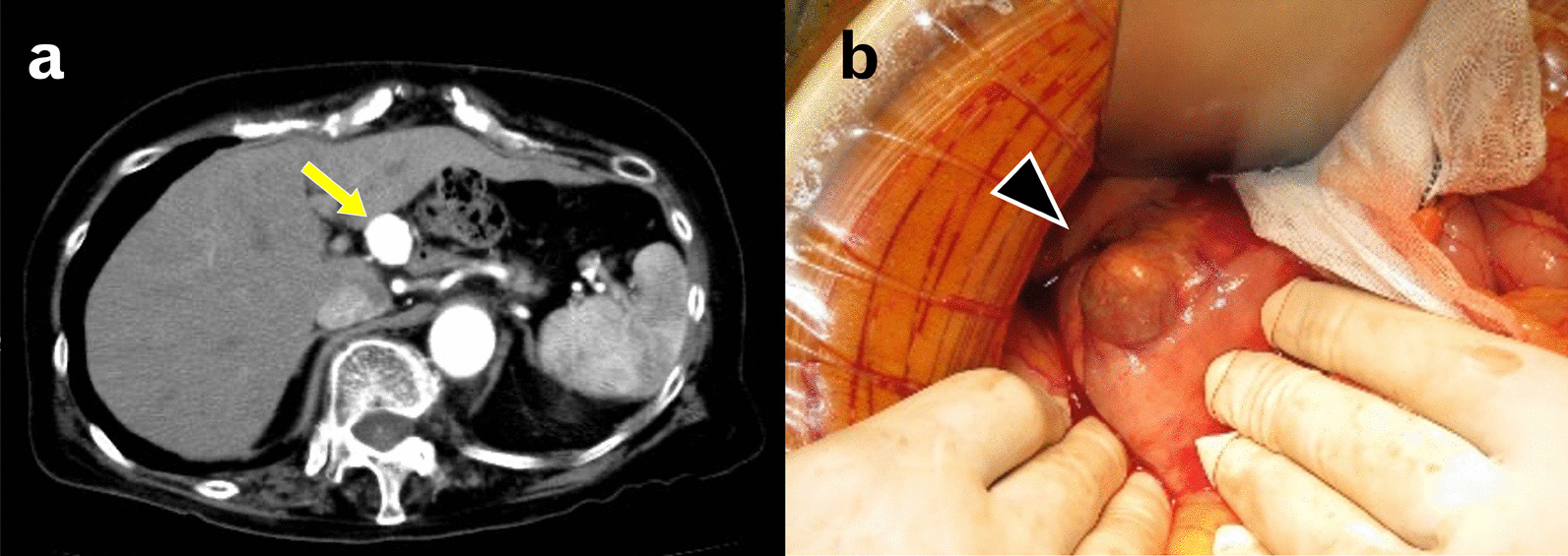
A histopathological diagnosis of GIS can be made by endoscopy or surgery. Although endoscopic identification is possible in some cases, surgery may be required in cases where endoscopic lesions are not seen or a biopsy is difficult to diagnose [6]. In the present case, no lesion was endoscopically identified, and surgery was necessary for a histopathological diagnosis. Peritoneal dissemination of PNET was suspected because of the gradual increase in tumor size, but no other metastases, invasion into the surrounding tissue, or enlargement of lymph nodes were observed. Thus, the patient underwent laparoscopic surgery for diagnostic and therapeutic purposes. Laparoscopy in bowel surgery has been associated with lower perioperative mortality, lower complication rates, earlier discharge, and lower hospitalization costs compared with open surgery and is therefore considered less invasive [11]. In addition, laparoscopic surgery allows a wider view of the abdominal cavity when adhesions are minimal. CT scans and FDG-PET are useful for detecting peritoneal dissemination, and the combination of both modalities allows for the detection of most lesions; however, their combination may be insufficient for detecting very small lesions. Although adhesions are expected in cases with a history of surgery, it could be possible to search for intra-abdominal lesions by combining preoperative imaging with laparoscopy, which is less invasive and allows for intra-abdominal inspection. Therefore, we selected the laparoscopic approach, ensured radical resection, and achieved a definitive diagnosis with minimal invasiveness.







留言 (0)