In the case reported herein, the medical record review showed that CT-guided percutaneous needle biopsy was an indicated diagnostic procedure considering the medical history of the patient, the radiological findings, and the impossibility of formulating a diagnosis of the lung lesion through EBUS-TBNA. Unfortunately, the patient experienced a systemic air embolism (SAE) that directly lead to his death shortly after the procedure. Mortality due to systemic air embolism (SAE) following CT-guided percutaneous needle biopsy of the lung is reported to be approximately 0.0002% in the largest series [8]. To the best of our knowledge and after a thorough review, only seven SAE fatal cases of air embolism have been thoroughly described in the literature [9,10,11,12,13,14,15], as summarized in Table 1. While the vast majority of SAEs are undiagnosed in asymptomatic patients, in cases of life-threatening SAE, diagnosis is generally clinically suspected based on the abrupt decline of the neurologic and/or cardiovascular condition of the patient, like that seen in the patient presented. The prognosis of SAE depends primarily on the quantity of air entering the vascular system. Brain and chest CT scans can provide a radiologic confirmation by detecting bubbles (typically seen as a void in the contrast material within the vessel) in the cerebral vascular system, ascending aorta, the left side of the heart, and pulmonary veins [16]. Early treatment of a SAE consists of prompt administration of 100% oxygen and placing the patient in the left lateral decubitus position with lowering of the head in an effort to increase the intracavitary pressure of the left atrium and avoid cerebral embolization of air [17].
Table 1 Fatal cases of air embolism complicating CT-guided percutaneous needle biopsy of the lung reported in the literature
From a pathophysiological point of view, arterial air embolism stems from air entering the pulmonary veins during percutaneous needle biopsy of the lung. According to the literature, several different mechanisms may be responsible for air entry into the pulmonary venous system, firstly, through a hole in the pulmonary vein caused by the needle (catheter) after removal of the inner stylet, resulting in the rising of the pressure gradient between atmospheric pressure and the pulmonary venous pressure (likely occurring during inspiration). In this case, air may enter directly through the catheter. Secondly, air may be directly injected during the procedure into the pulmonary arterial circulation and then enter the pulmonary veins by crossing the pulmonary capillaries. Lastly, the needle may simultaneously penetrate the pulmonary vein and an adjacent air-containing space (i.e., alveolar space, bronchus, air cyst, cavity), creating a communicating fistula. In the latter case, Valsalva maneuvers can increase the pressure in the air space, resulting in vascular air embolism [5, 12]. It is worth mentioning that an air volume of 0.5–1.0 mL is enough to cause cardiac arrest through coronary artery air embolism, and 2.0 mL is enough to cause a fatal stroke through cerebral air embolism [18].
The prevention of SAE includes operator and patent-related measures. The operator must ensure the occlusion of the introducer needle by the inner stylet or own finger, while the patient should be instructed to avoid breathing deeply and coughing during the biopsy [19]. Some authors suggest an increased probability of SAE when using a coaxial approach and larger needles. In fact, the coaxial method increases the risk of communication of the lung parenchyma with the atmosphere after extraction of the inner stylet, whereas larger needles show an increased risk of pulmonary vein puncture along the needle path [20]. However, fatal SAE may also occur using techniques other than the coaxial method [9, 10, 12, 13] and with smaller needles [15]. The patient’s position during the procedure has also been discussed as a potential risk factor for the development of fatal SAE [4]. However, analysis of the literature about SAE cases has shown that a fatal event can occur regardless of the patient’s position during the procedure. Additional potential risk factors mentioned in the literature are post-inflammatory changes in the portion of the lung traversed by the needle, including increased vascularity, vasculitis, or friable lung tissue. All of these could affect the physiologic hemostatic mechanisms resulting in protracted exposure of the blood flow to the airway [5].
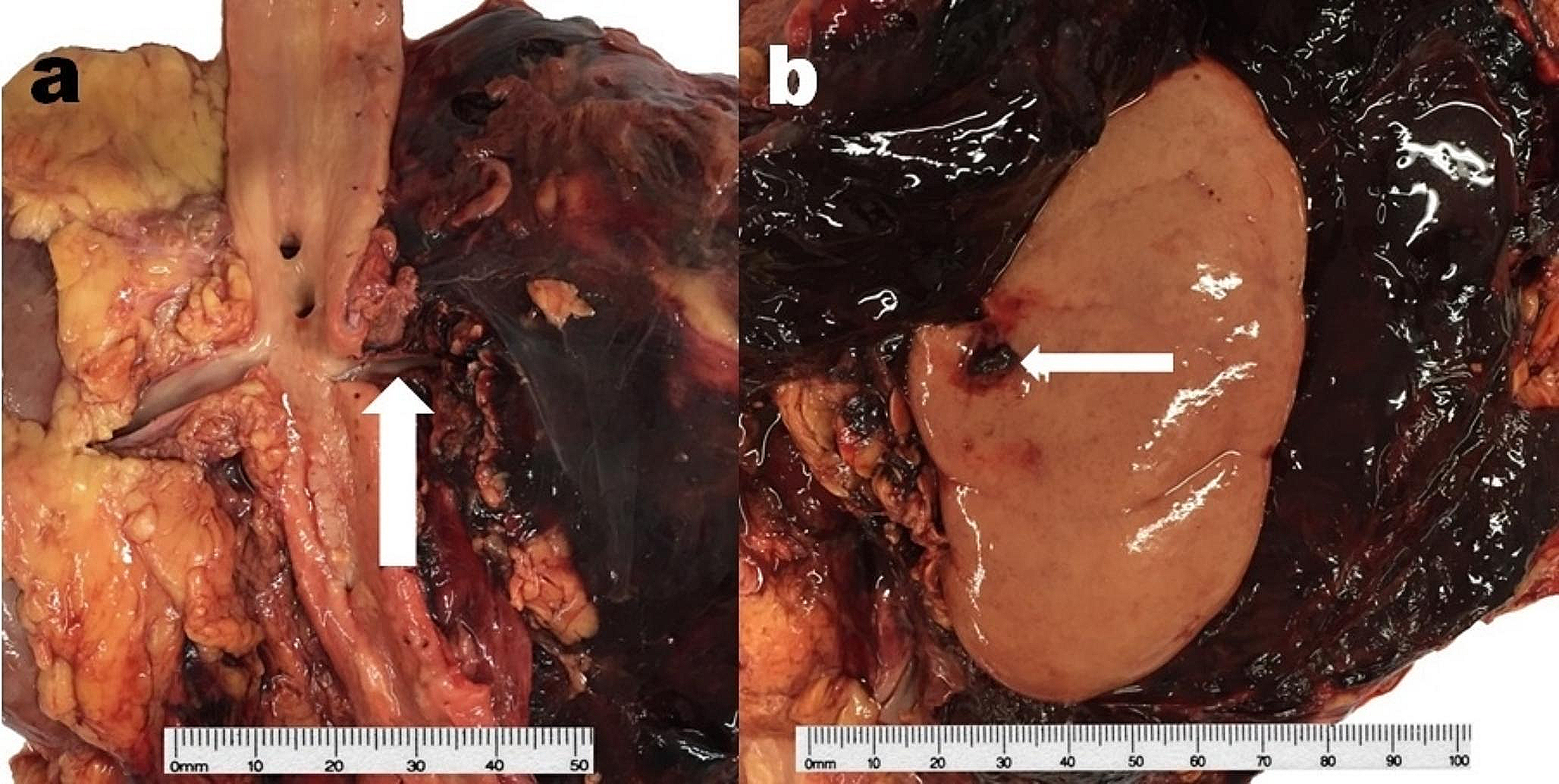
To the best of our knowledge, this is the first case of fatal SAE to be discussed within a medicolegal context and with available radiological and autopsy evidence to assist with evaluating operator behavior. In particular, the macroscopic and microscopic analyses of the lung revealed the presence of a distinct and straight pathway through the parenchyma from the skin to the lung mass. This, along with the CT scans obtained during the procedure, supports the adherence of the operator to the international procedural guidelines [17], which recommend choosing the shortest needle path to the lesion to reduce the thickness of the involved parenchyma. In this case, it was obtained by keeping the patient in the prone position and by using a coaxial method that allowed for multiple needle biopsy sampling with a single intraparenchymal path created by the core biopsy needle.
The above considerations ruled out medical errors regarding indication and/or operative technique and further identified the occurrence of cardiac air emboli as an intervention complication. In our opinion, given the clinical and autopsy findings, a significant entry of air through a fistula between the air-containing space (alveolar space) and an adjacent pulmonary venous vessel created during the needle penetration likely occurred. It is likely that the Valsalva maneuver related to the cough of the patient at the end of the procedure facilitated air penetration into the vascular system. Air reached the left heart and coronary arteries through the pulmonary vein causing heart and coronary embolism with resulting myocardial ischemia, decreased myocardial function, and death.
Despite the unfavorable outcome, the multidisciplinary review of the procedure indicated that in the absence of any known risk factors, alternatives such as conservative surveillance through imaging and invasive surgical options both shared significant risks when compared to CT-guided percutaneous needle biopsy. Furthermore, the consent procedure was adequate, and ultimately, the patient was able to make an informed decision regarding his care plan, correctly carried out, giving to the patient all the information needed for his choice.
The medicolegal point of view proposed herein for analyzing fatal SAE cases is important because air embolism following CT-guided percutaneous needle lung biopsy is a complication that is difficult to prevent and could serve as a possible source of litigation. Although several recommendations and precautions have been suggested to reduce the risk of SAE following CT-guided percutaneous needle biopsy of the lung, this complication can occur particularly in cases with long operative exposure and despite careful technical execution. It is often worth acknowledging that in the context of personalized treatment, this diagnostic procedure represents a major trend in the future [21]. On this basis, a thorough disclosure of the procedure given preferably by the operator during the consent process, including all procedure-associated risks, even the rarest but potentially fatal ones, is recommended. In fact, to ensure adequate informed consent, providing accurate and in-depth information, including alternative invasive and conservative approaches, is essential to reduce medicolegal litigation issues.







留言 (0)