
記住我





In the United States, chronic wounds affect around 6.5 million patients a year and cost more than $25 billion to treat.1 The burden to treat wounds is growing rapidly due to increasing healthcare costs; contributing factors include an aging population and rises in the prevalence of diabetes mellitus and obesity. Negative pressure wound therapy (NPWT) is routinely used on a variety of wounds.2Negative pressure wound therapy is frequently delivered via relatively large, multiple-user devices, also referred to as “traditional” NPWT systems.3–5 Although these systems have multiple advantages, such as the ability to handle large volumes of fluid, there are limitations to their use in clinical practice. For example, traditional NPWT devices are challenging when delivered in outpatients or home care settings, with a complex administrative burden to ensure that billing accurately reflects usage on each individual patient.4 These devices can also be relatively expensive, with scheduled collection and returning of each device costing an average of $60 per home visit.6,7 In addition, devices must be cleaned between patients' reducing availability.4 From the patient's perspective, larger devices can be cumbersome and may impair mobility.5
Single-use NPWT devices (also referred to as personal-use devices) are an alternative to multiple-user devices.3–5 These systems are compatible with use in the outpatient and/or home care setting.3,5 Their small size makes them discreet and less likely to impair patient mobility and activities of daily living, especially in ambulatory patients.5 Their design avoids the need for many administrative tasks associated with tracking, pickup, cleaning, billing, and reissuing to another patient.5 Furthermore, single-use NPWT devices may be used at home. The aim of this study was to evaluate the effects of treatment with a single-use NPWT system in a patient group from an outpatient's setting.
METHODSThe study design was a multiple case series reporting individually selected outcomes using a single intervention. Participants were drawn from 2 clinics located in the Southeastern United States (Austell and Augusta, Georgia). Inclusion criteria were adults 18 years of age or older with varying wound types and determined to be in need of NPWT by a physician provider and were deemed eligible for enrollment. Exclusion criteria were patients with wounds containing necrotic tissue with eschar, untreated osteomyelitis, nonenteric and unexplored fistulas, malignant wounds, or wounds with solid organs, large vessels, along with anastomotic sites of blood vessels or bypasses. Study procedures were reviewed and approved by a central Institutional Review Board (IntegReview IRB, subsequently renamed Advarra, protocol number: GHC1901, date of approval: November 11, 2020). Study participants were enrolled between December 2020 and May 2021.
Study OutcomesThe study design allowed multiple outcomes based on the goals of care established by the participant's care provider. Specifically, a primary goal of treatment was individually determined by the participant's physician or other provider based on wound type, immediate goals of wound care, comorbid conditions, and other factors. The individualized goal was determined during a baseline visit and after informed consent for study participation was obtained. Possible outcomes were (1) decrease in wound volume, (2) decrease in size of the tunneling area, (3) decrease in size of the undermining, (4) decrease in amount of slough, (5) increase in granulation tissue formation, (6) decrease in periwound swelling, and (7) wound bed progression enabling transition to another treatment modality such as topical therapy, surgical closure, or a flap or skin graft. We also evaluated the ease of device use perceived by providers caring for study participants and participant satisfaction with the device. Objective measures of these study outcomes were measured at baseline assessment and subsequently at weekly clinic visits (Table 1).
TABLE 1. - Overview of Study Procedures End Points Measured Method of Assessment Procedure Performed by Study Personnel Determination of end point measures at baseline visit The study end points were determined by the physician at the time of enrollment, upon documentation of the goal of therapy. Goal of therapy documented at baseline visit.Abbreviations: CRF, Case Report Form; NPWT, negative pressure wound therapy.
The intervention was NPWT delivered via a single-use NPWT system (Medela INVIA Motion Endure, Medela, Switzerland) (Figure 1). The device included a portable, rechargeable, battery-powered pump with a typical battery life of 10 hours. The device has a canister with a 150-mL capacity and delivers suction levels varying from −40 to −175 mm Hg. The device provides continuous or intermittent suction, similar to multiuse devices.3 Wound dressing kits designed for this device (INVIA Foam Dressing Kit with FitPad, Medela, Switzerland) were used.
 Figure 1.:
Figure 1.: Single-use NPWT system.
Study ProceduresTable 1 provides a detailed summary of study procedures completed during baseline and subsequent visits. Negative pressure wound therapy began at the baseline visit and after completion of informed consent. After a thorough wound assessment at the baseline visit, the wound was cleansed and debrided as indicated, and a cyanoacrylate-based polymer skin protectant was applied to the periwound skin. A nonadherent contact layer was placed prior to the placement of foam wound filler into the wound if deemed necessary. The foam was cut to size and shape of the wound before placing it in the wound bed, and a transparent adhesive film was then applied. Finally, a hole was cut into the transparent film to allow a double lumen suction pad to be positioned. The dressing tubing was attached to the pump tubing, and therapy parameters such as negative pressure level and continuous versus intermittent suction therapy were selected.
Research staff attended weekly clinic visits, and a wound assessment was completed that included an evaluation of the individualized outcome selected at the baseline visit. The research staff also collected data on any pump issues or complications that the study participant experienced each week. Photographs of the dressing on the wound prior to dressing application as well as photographs of the wound after dressing removal were obtained. The research staff obtained a weekly survey from the wound clinic staff member to determine ease of use and total wound dressing resources required. An assessment of any adverse events (AEs) related to the study device was also conducted at each weekly visit. As noted earlier, study end points were the achievement of the participant's individualized goal or the completion of 4 weekly visits.
Data AnalysisDescriptive analyses were computed using R software (R Core Team [2021]; R Foundation for Statistical Computing, Vienna, Austria). Table 1 summarizes the primary outcome selected for each participant. Changes in each outcome were measured as the difference at baseline versus the outcome at the study end point for that participant. Based on the outcome variable selected, descriptive data are presented as mean and standard deviation or median and interquartile range (IQR). In addition, individually selected outcomes are plotted on a graph to better identify time trends. For the evaluation of the progression of the wound bed toward transition to another treatment modality, the frequency and percentage of study participants reaching this outcome at any time point were analyzed. Wound area (maximum length × width) and volume (area × maximum depth) were calculated. Differences in wound measurements between baseline and the end of the study were expressed as mean (SD) or median (IQR) as appropriate. No inferential statistical analyses were calculated; therefore, no attempt was made to calculate a minimum sample size calculation, and results are considered observational. The sample of 25 patients was used to illustrate the use of the personal-use NPWT system in a relevant population. Any missing data points (from postbaseline time points) were imputed using last observation carried forward.
RESULTSTwenty-five participants were enrolled, all of whom received at least 1 application of NPWT. Seven study participants were withdrawn for a variety of reasons: 2 suffered an AE (deemed unrelated to the study device) requiring hospitalization, 1 withdrew of his or her own choice, 1 withdrew due to pain unrelated to NPWT, and 3 were withdrawn by their physician (2 were lost to follow-up and 1 was admitted to hospital for an AE not related to the study device).
Table 2 summarizes participant characteristics; safety data were collected on all 25 participants. The group had a mean age of 51.2 years (SD: 18.2; range: 19-79 years). Fourteen were male (56%), 14 were African American (56%), 10 were White (40%), and 1 was Pacific Islander (4%). Wound types were diabetic foot ulcer (n = 4), pressure injury (n = 1), abscess or cyst following either debridement or an incision and drainage procedures (n = 7), necrotizing fasciitis needed management of a debrided wound (n = 4), nonhealing postsurgical wound (n = 5), and other types of wounds (n = 4).
TABLE 2 - Participant Demographic and Pertinent Clinical Characteristics at Baseline N = 25 % Male, n (%) 14 (56) Age, mean (range), y 51.2 (19-79) Race, n (%) African American 14 (56) Pacific Islander 1 (4) White 10 (40) Wound type, n (%) DFU 4 (16) PI 1 (4) Abscess/cyst 7 (28) Necrotizing fasciitis 4 (16) Nonhealing surgical wound 5 (20) Other 4 (16) Assigned primary treatment goal, n (%) Decrease in wound volume 22 (88) Increase in granulation tissue 3 (12)Abbreviations: DFU, diabetic foot ulcer; PI, pressure injury.
The most common individualized treatment outcome was to achieve a decrease in wound volume, chosen for 22 of 25 study participants. The goal to increase granulation tissue was chosen for the remaining 3 study participants. Additional goals were identified for 17 (68%) study participants, with multiple additional goals selected for 3 study participants. The most common additional goal was an increase in granulation tissue (14 study participants). Also selected were decrease in the size of tunneling and/or undermining area (2 study participants), decrease in wound volume (2 study participants), decrease in edema (1 study participant), and progressing acceptably toward a transition to another treatment modality (1 study participant). The treatment goals “decrease in the amount of slough” or “decrease in edema/periwound swelling” were not selected for any of the study participants in this study.
Progress Toward Primary OutcomeA completed analysis was conducted on 23 of 25 participants who received baseline and at least 1 additional NPWT visit; 18 of the 23 (78.3%) participants who reached a study end point (achievement of their primary treatment outcome or 4 weekly visits) achieved their preindividualized treatment outcome.
The change in wound dimensions was objectively measured by monitoring wound area and volume at weekly intervals throughout treatment (Figure 2). Overall, median (IQR) results showed that wound area reduced from 55.0 (19.4-69.9) cm2 at baseline to 19.3 (8.1-39.5) cm2 at the final visit, an absolute median reduction of 19.3 (3.0-37.5) cm2. When converted into a percentage reduction in wound area, the median percentage reduction was 42.7% (IQR: 25.7-71.5). Wound volume reduced from a median (IQR) of 105.0 (24.0-247.5) cm3 at baseline to 12.0 (4.2-44.9) cm3at the final visit, an absolute median reduction of 59.3 (11.1-140.3) cm3. The median percentage reduction in wound volume by the final visit was 87.5% (IQR: 30.7-94.6) compared with baseline. In this subset, the median (IQR) duration of NPWT therapy was 19 (14-21) days. The proportion of study participants with granulation tissue in the wound bed was recorded at each visit. At baseline, 16 (69.5%) study participants had granulation tissue in their wound bed; this increased to 23 (100%) study participants by the final visit.
 Figure 2.:
Figure 2.: Reduction in wound area and volume. Percentage of reduction in wound area and volume at the end of therapy in comparison with baseline are shown expressed as median (horizontal line); mean is expressed as x. n = 23.
SafetyAs described earlier, safety outcomes were calculated for 25 participants who received the intervention (single-use NPWT). Their median (IQR) time with dressing was 18 (14-21) days. Five AEs were recorded in 4 study participants, including 4 serious AE (SAE). Four (80%) were not associated with device use, and 1 was associated with device use. One study participant experienced 2 SAEs: postoperative angina in the setting of ischemic cardiomyopathy and, subsequently, shortness of breath and chest pain. This study participant was hospitalized and withdrawn from the study. A second study participant suffered a stroke, was admitted to the hospital, and was withdrawn from the study. A third study participant was hospitalized for aggressive behavior and, subsequently, withdrawn from the study. The fourth patient experienced localized contact dermatitis of the periwound area, an AE that associated with the device (the dermatitis was associated with use of a transparent sealing film, part of the NPWT dressing kit). This AE was not deemed serious and resolved during the course of treatment with no further sequelae.
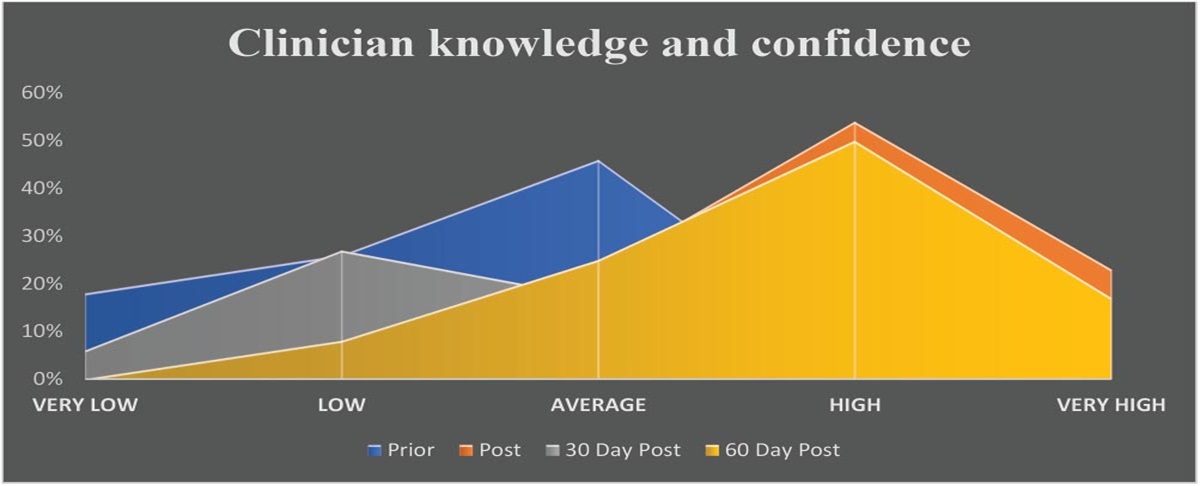
Clinician SatisfactionClinician satisfaction with the device was assessed following baseline applications for all 25 study participants (Figure 3). Analysis at baseline indicated that 64% of clinicians were “satisfied” and 28% were “more satisfied” with the single-use NPWT device compared with the use of a traditional (multiuser) NPWT device used in the clinic. For ease of use overall, at baseline, clinicians were “satisfied” or “more satisfied” in 56% and 32% of applications, respectively, compared with the traditional NPWT device usually used in the clinic. Two of the satisfaction questions pertained specifically to the ability of the NPWT device to manage wound fluid. The majority of clinicians were satisfied or more satisfied when questioned about the “ability [of the device] to maintain a dressing seal” (56% and 28%, respectively) and the “ability [of the device] to manage exudate” (52% and 20%, respectively).
 Figure 3.:
Figure 3.: Clinician satisfaction. Satisfaction results obtained following baseline application; n = 25.
DISCUSSIONThe primary objective of this study was to determine the effect of a single-use NPWT system based on individualized goals of treatment in a variety of wound types. The individualized treatment goals were met in participants (18 of 23, 78.3%) who completed the study protocol.
When initiating NPWT, it is important to clearly define the clinical reasons why NPWT is needed by setting treatment goals. It is also important to monitor progress against those goals at regular intervals, using objective measures. An expert panel previously recommended that a single goal should be chosen as the primary treatment goal, and when that goal is achieved within a predetermined time frame, the remaining needs of a wound should then be reassessed.8 This reevaluation was deemed necessary to avoid overuse of NPWT and promote prompt identification of alternative wound treatments when indicated. Median reductions in wound area and volume in this study set were 42.7% and 87.5%, respectively, over a median treatment duration of 19 days; these clinical outcomes were comparable to previous data using the same single-patient-use NPWT system.9
Our results compared well with other literature on NPWT-treated study participants with similar wound indications. One randomized controlled trial assessing outcomes of NPWT in difficult-to-heal wounds reported that wounds treated with NPWT halved in volume within a median time of 2 weeks.10 One widely used benchmark, suggestive of good progress toward healing, is a 50% reduction in wound area over a 4-week treatment period, or a 10% to 15% reduction per week.11 Given the median duration of therapy of 19 days (2.7 weeks), the overall percentage reduction in wound area, reported in this study (42.7%), appears to satisfy this expected minimal benchmark, supporting the role in wound healing of this device.
LimitationsThe study had several limitations. Multiple study outcomes were identified, and inferential statistical tests could not be used to analyze outcomes. Treatment outcomes were assigned by the participant's physicians, who judged the progress toward the outcome creating a risk of detection bias. We attempted to minimize this bias by evaluating objective outcomes such as wound volume; we acknowledge that some outcomes employed subjective assessments. Study withdrawal may have influenced the generalizability of findings.
CONCLUSIONSThe single-use NPWT system evaluated in this study achieved multiple therapeutic outcomes in a variety of wound types (etiologies). Clinicians were satisfied with the performance and ease of use of the device. No serious AEs occurred that were associated with the use of the device.
ACKNOWLEDGMENTSEditorial assistance was provided by JMS Medical Writing Services Ltd. Statistical analysis was provided by Dr Delphine Courvoisier (University Hospitals of Geneva, Switzerland).
REFERENCES 1. Sen CK. Human wound and its burden: updated 2020 compendium of estimates. Adv Wound Care. 2021;10(5):281–292. 2. Apelqvist J, Willy C, Fagerdahl A, et al. Negative pressure wound therapy—overview, challenges and perspectives. J Wound Care. 2017;26:S1–S113. 3. Banasiewicz T, Banky B, Karsenti A, Sancho J, Sekáč J, Walczak D. Traditional and single use NPWT: when to use and how to decide on the appropriate use? Recommendations of an expert panel. Wounds Int. 2019;10(3):56–62. 4. Hurd T, Kirsner RS, Sancho-Insenser JJ, et al. International consensus panel recommendations for the optimization of traditional and single-use negative pressure wound therapy in the treatment of acute and chronic wounds. Wounds. 2021;33(suppl 2):S1–S11. 5. Crumley C. Single-use negative pressure wound therapy devices: a technologic analysis. J Wound Ostomy Continence Nurs. 2021;48(3):195–198. 6. Morrison Informatics, Inc. A Comprehensive Cost Analysis of Medicare Home Oxygen Therapy: A Study for the American Association for Homecare. Morrison Informatics, Inc; 2006. 7. Marquardt C, Koppes P, Krohs U, et al. Negative pressure wound therapy using PHMB gauze for the management of postoperative subcutaneous surgical site infection. Coloproctology. 2014;36:364–369. 8. Birke-Sorensen H, Malmsjo M, Rome P, et al. Evidence-based recommendations for negative pressure wound therapy: treatment variables (pressure levels, wound filler and contact layer)—steps towards an international consensus. J Plast Reconstr Aesthet Surg. 2011;64(suppl):S1–S16. 9. Mullins RF, Wilson J, Hassan Z, et al. The role of personal-use negative pressure wound therapy with enhanced functionality in achieving wound-related treatment goals: a small prospective study. Wounds. 2023;35(3):53–58. 10. de Laat EH, van den Boogaard MH, Spauwen PH, van Kuppevelt DH, van Goor H, Schoonhoven L. Faster wound healing with topical negative pressure therapy in difficult-to-heal wounds: a prospective randomized controlled trial. Ann Plast Surg. 2011;67(6):626–631. 11. Gottrup F, Apelqvist J, Price P. Outcomes in controlled and comparative studies on non-healing wounds: recommendations to improve the quality of evidence in wound management. J Wound Care. 2010;19(6):237–268.
留言 (0)