
記住我

Upper endoscopy is the method of choice in the diagnosis of diseases in the upper gastrointestinal tract. The total number of endoscopies performed has been steadily increasing, with a 54% increase in upper endoscopies performed in the USA between 2000 and 2009 [1]. Simultaneously, the incidence of esophageal adenocarcinoma is increasing in Western countries, and therefore increasing demands are being placed on the quality of upper endoscopy performance not only in Asian countries with a high incidence of gastric cancer, such as Japan and South Korea [2]. A number of European guidelines have been published, however, some important quality parameters are still missing due to a lack of data [2,3]. Especially in the diagnosis of early neoplastic lesions that can be curatively managed endoscopically and where the 5-year survival rate of patients exceeds 85%, a sufficiently clear mucosa of the examined area is essential [2,4]. Mucosal clarity is often reduced by the presence of mucus, bubbles, food residue, bile, or blood. The European Society of Gastrointestinal Endoscopy (ESGE) recommends, as a preprocedural precaution, only fasting for 6 h before the procedure, with fluids allowed for a maximum of 2 h before the examination [3]. Also, no widely accepted score assessing mucosal visibility in the upper gastrointestinal tract, such as the Boston Bowel Preparation Scale for colonoscopy, is available [2,5]. Still discussed is the use of premedication with mucolytics (n-acetylcysteine, pronase) and simethicone given before gastroscopy. Pronase is a proteolytic enzyme available and used in Asia, whereas n-acetylcysteine and simethicone are agents commonly available in Europe. Simethicone, as an antifoaming agent, is recommended by the ESGE for administration as part of bowel preparation prior to colonoscopy [6]. A number of studies, mostly Asian, have been conducted to evaluate the effect of these agents on increasing mucosal transparency in the upper gastrointestinal tract [7–19]. Most of these studies have demonstrated an effect primarily of simethicone [8–11,17,18]. The question then remains as to the effect and use of n-acetylcysteine in this regard, and the results of studies in this regard, particularly regarding its effective dose, are equivocal. The aim of this study was to demonstrate that a higher, maximal dose of mucolytic administered before gastroscopy improves mucosal clarity in the upper gastrointestinal tract compared with placebo, that is, with or without administration of plain water or mucolytic solution.
MethodsThe study was conducted from May to September 2021, at the Digestive Diseases Center, Vitkovice Hospital, Ostrava, Czech Republic. The endoscopists involved in the study were experienced endoscopists who perform more than 300 gastroscopies per year. The study protocol was approved by the local ethics committee, the State Institute for Drug Control of the Czech Republic, and was registered in the Clinical Studies Registry at ClinicalTrials.gov (NCT04641455). All patients enrolled in the study signed informed consent and a General Data Protection Regulation consent form. Patients who met the inclusion criteria, that is, aged over 18 years, who were able to understand and sign the informed consent, indicated for diagnostic gastroscopy were included in the study. The exclusion criteria included planned therapeutic endoscopy, known organic gastric disease or status post gastric surgery, gastroscopy indicated for bleeding, dysphagia or impaired passage, gastroscopy under general anesthesia, allergy to mucolytic solution components and excipients, and pregnancy. All patients fasted 6 h before gastroscopy.
Randomization and blindingOn arrival at the endoscopy reception, a consultation with the examining physician took place. The patient was allowed to ask questions and those who met the inclusion criteria of the clinical trial and signed informed consent were randomized into four branches, randomization ratio 1 : 1 : 1 : 1. Each patient was given an envelope at the endoscopy reception, inside the envelope was the number which was assigned to the patient and under which they appeared in the study. Each number was assigned a letter, A–D, which characterized the relevant branches, according to the randomization sequences. In accordance with this, the nurse at the reception desk, who was unblinded, subsequently prepared and administered the solution to the patient, in the case of branch A 100 ml of water + 600 mg n-acetylcysteine + 400 mg simethicone, in branch B 100 ml of water + 400 mg n-acetylcysteine + 20 mg simethicone, in branch C 100 ml of water, or the solution was not given in the case of branch D. The study was double-blinded, with the patient, the endoscopist performing the procedure, the endoscopic nurse assisting with the procedure, and the endoscopists assessing the photodocumentation taken at the second time point. The solution was administered in a white plastic cup, and as n-acetylcysteine was administered in the form of ACC NEO tablets with a blackberry flavor, the patients in branch C were given 50 ml of pure water + 50 ml of berry-flavored mineral water as a placebo, which made the risk of the patient blinding the administered solution virtually zero. Only the nurse at the endoscopy desk had access to the randomization codes until the study unblinding. The exception was in case of need of the emergency situation, when the investigating physician or the endoscopist, unless they were the same person, could immediately know which branch the patient was randomized to. The study was then blinded from the start of the study, that is, the inclusion of the first patient, until the final evaluation of the blinded data obtained. The final evaluation of the blinded data obtained means the completion of the evaluation of the photodocumentation of the last patient by the blinded endoscopist. After that, the study was unblinded and the obtained data were statistically evaluated.
ProcedurePatients were informed about the possibility of participating in the trial when they made an appointment for endoscopy, and they received informed consent for the study. They presented for gastroscopy 1 h prior to the procedure, at which time consultation with the investigating physician took place, and then, if they met the inclusion criteria and signed the informed consent, randomization to each branch with solution administration took place. Women able to become pregnant were required to undergo an orientation urine pregnancy test before inclusion in the study. After drinking the solution, upper endoscopy was then performed 20–30 min later. In the case of sedation, midazolam was used at a dose of 1–3 mg. The procedures were performed with endoscopes from Olympus (CF-HQ190L and 180L Olympus, Evropská, Czech Republic). Carbon dioxide was used for insufflation. The performing endoscopist evaluated mucosal visibility and determined the so-called visibility score of the upper gastrointestinal tract during gastroscopy before mucosal lavage and biopsy. He then performed mucosal rinsing and gastroscopy as usual. At the same time, he recorded the gastroscopy time from insertion to removal of the endoscope, including photodocumentation and the amount of residual fluid in the stomach, where a score of 0 corresponds to no fluid in the stomach, 1 is a slight amount that cannot be suctioned, 2 is a small amount that can already be suctioned, and a score of 3 corresponds to a gastric lake [3]. At the second time point, the photodocumentation was then evaluated and the mucosal visibility score was determined by two blinded endoscopists. If sedated, the patient was observed in the recovery room for 30 min after the procedure. The following day, within 24 h after the procedure, patients were contacted by phone to record any late adverse events.
Clinical trial objectives and plansThe primary endpoint of the study was to demonstrate that a higher, maximal dose of mucolytic, administered 20–30 min prior to gastroscopy (group A), increases visibility score compared to no administration of water or mucolytic solution (group D). Visibility score is defined as the sum of five scores 0–5 in the esophagus, fundus, body, and antrum of the stomach and duodenum, for a total of 0–25 (Fig. 1).
 Fig. 1.:
Fig. 1.: Assessment of visibility score during upper endoscopy; 5 = completely clear mucosa throughout without fluid or any coating; 4 = clear liquid residue; 3 = reduced visibility on <25% of the area of the evaluated section (turbid fluid, mucus, bubbles, bile, food debris); 2 = reduced visibility on 25–50% of the area of the evaluated section (turbid fluid, mucus, bubbles, bile, food debris); 1 = reduced visibility over >50% of the area of the assessed section (turbid fluid, mucus, bubbles, bile, food debris); 0 = reduced visibility in most (>75%) of the area of the assessed section (turbid fluid, mucus, bubbles, bile, food debris).
The secondary objective was to demonstrate that mucosal visibility after administration of a higher, maximal dose of mucolytic (group A), is higher than the score after administration of a lower dose of mucolytic (group B).
The visibility score was also assessed by blinded endoscopists using 10 photographs taken, again given by the sum of five scores 0–5 in the esophagus, fundus, body, and antrum of the stomach and in the duodenum [3] (Fig. 2).
 Fig. 2.:
Fig. 2.: Photodocumentation during upper endoscopy.
Statistical analysisOn the basis of a power analysis, where the primary objective was to compare group D (gastroscopy without administration of mucolytic solution and water) to group A (with maximum mucolytic dose), estimates of 26 patients per branch were determined. We assumed a 10% increase in the mean visibility score, power 0.8, based on data from our previous study, where the visibility score in the group of patients without administration of mucolytic solution or water was 17 ± 2.0 [16]. Branches B and C were the control branches. The study ultimately enrolled 30 patients in each branch, for a total of 120 patients.
The chi-square test was used to analyze patients by sex. Analysis of variance was then used to analyze patients by age, to assess the visibility scores for each study branch, and to assess the amount of residual fluid in the stomach and the time of examination. The Mann–Whitney U test was used to compare the visibility scores between study branches, and the significance values of the Mann–Whitney U test were then corrected by the Bonferroni for multiple comparisons.
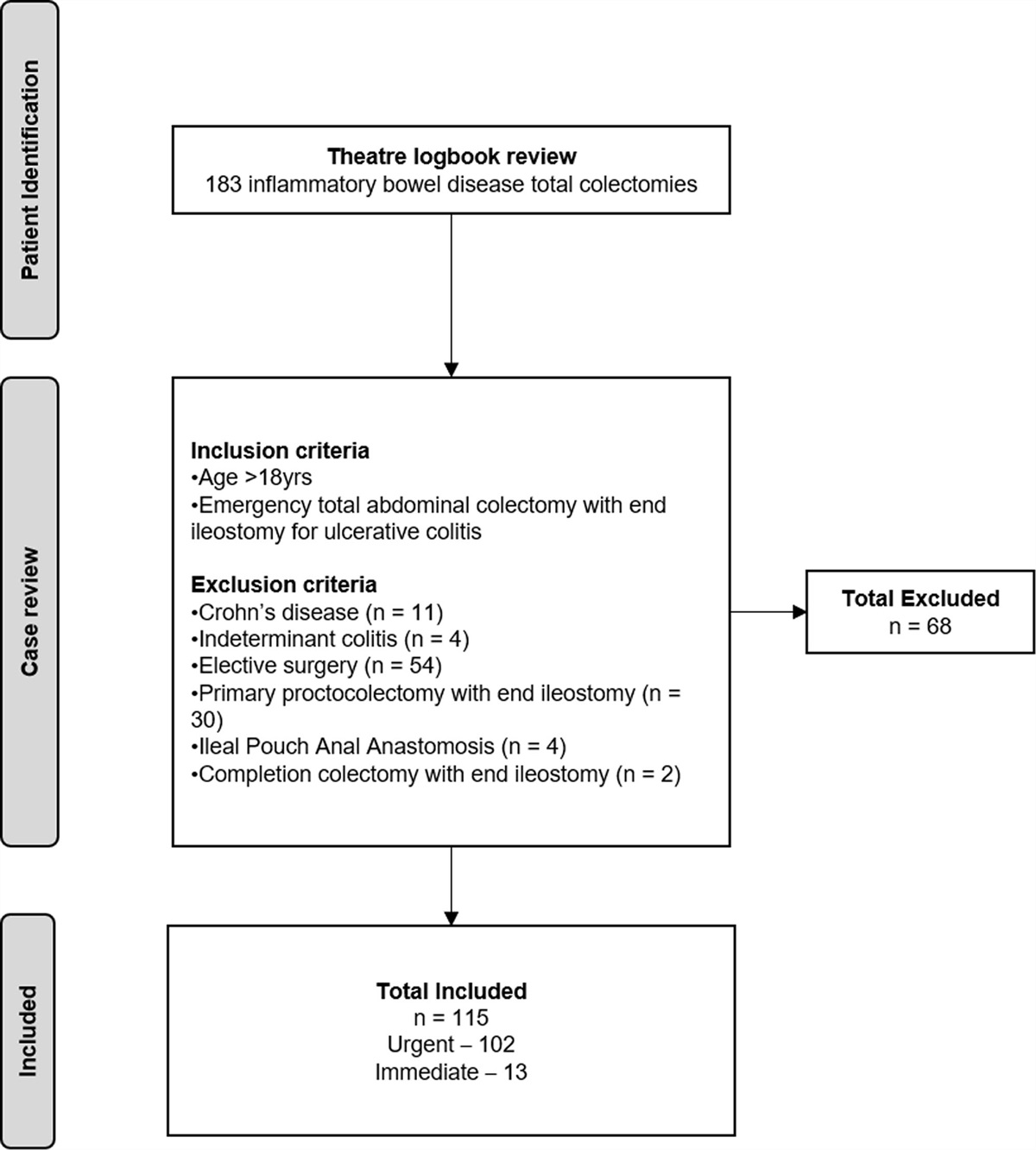
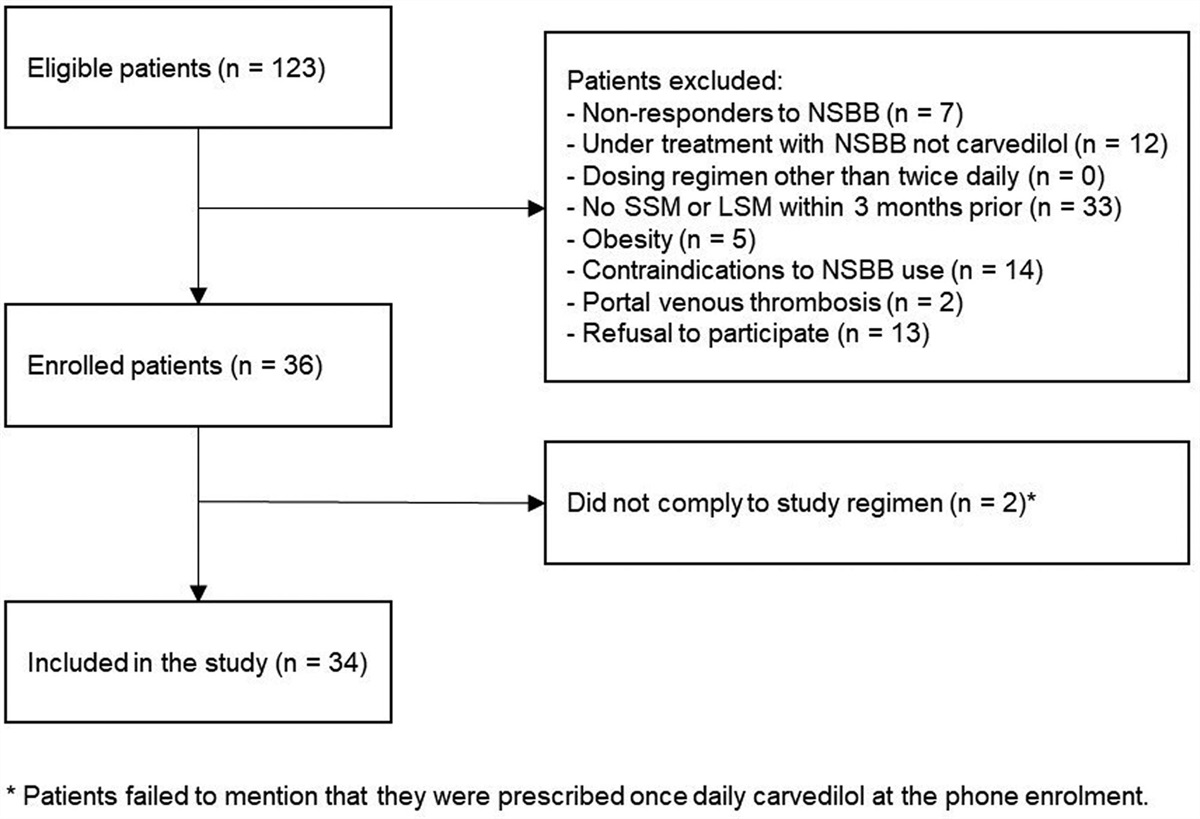
ResultsA total of 129 patients who met the inclusion criteria were included in the study. The patients were randomized into four groups (Fig. 3). Nine patients were subsequently excluded because of procedure intolerance, technical failure in image acquisition, or gastric peristalsis disorder detected during the procedure. Patients did not differ significantly in age (P = 0.342), sex distribution (P = 0.785), or indications for examination (P = 0,523; Table 1). The primary endpoint, the overall visibility score as assessed by the performing endoscopist, was similar between branches A, B, and C (18.9 ± 2.9 vs. 18,5 ± 3.4 vs. 18.6 ± 3.0, P = 1.000; Table 2); however, when comparing visibility scores of group A, B, and C to group D, only branch A demonstrated significantly higher visibility scores compared with branch D (18.9 ± 2.9 vs. 16.6 ± 3.3, P = 0.023; Table 3). The secondary endpoint, or the total visibility score assessed by the two blinded endoscopists from the photodocumentation taken, was different between the two endoscopists, and when the total visibility score was compared between all endoscopists, or the endoscopist performing the procedure and the two blinded endoscopists, there was a significant difference in the total visibility score between branches A and D only when assessed by the endoscopist performing the procedure (Table 3). There was no significant difference in the amount of residual fluid in the stomach between the branches when evaluated (P = 0.540; Table 4). The total examination time was comparable between branches (P = 0.132). Adverse effects of the administered medication were rare, with abdominal pain in a patient in group A and abdominal pain and diarrhea in a patient in group C.
Table 1. - Baseline patients characteristics Arm A (n = 30) B (n = 30) C (n = 30) D (n = 30) P valuea Age, mean ± SD, years 52.5 ± 11.9 47.1 ± 14.7 50.8 ± 12.7 52.7 ± 13.8 0.342a Sex, n (%) Male 15 (50.0) 13 (43.3) 15 (50.0) 17 (56.7) 0.785b Female 15 (50.0) 17 (56.7) 15 (50.0) 13 (43.3) Indication, n Dyspepsia 7 7 11 7 0.523c Pyrosis 7 3 2 5 Abdominal pain 10 9 12 14 Globus 1 0 1 0 Celiac disease 1 1 0 0 Idiopathic bowel disease 1 0 0 1 Before bariatric surgery 3 7 4 2 Anemia 0 2 0 1 Before cholecystectomy 0 1 0 0aOne-way analysis of variance (ANOVA).
bChi-squared test, (χ2-test).
cFisher exact test.
The table shows the significance values of the Mann–Whitney U test corrected by Bonfferoni for multiple comparisons. Significant difference in case of P < 0.05.
aTotal visibility score as assessed by the endoscopist performing the procedure.
bTotal visibility score assessed by the first blinded endoscopist.
cOverall visibility score as assessed by the second blinded endoscopist.
VS, visibility score assessed by the endoscopist performing the procedure; VS1, visibility score assessed by the first blinded endoscopist; VS2, visibility score assessed by the second blinded endoscopist; VS SUM, total visibility score as assessed by the performing endoscopist; VS1 SUM, total visibility score as assessed by the first blinded endoscopist; VS2 SUM, total visibility score as assessed by the second blinded endoscopist.
aOne-way-analysis of variance (ANOVA).
A score of 0 corresponds to no fluid in the stomach; a score of 1 is a tiny amount that cannot be suctioned; a score of 2 is a small amount that can already be suctioned; a score of 3 corresponds to a gastric lake.
n, total number; m, percentage.
aOne-way-analysis of variance (ANOVA).
 Fig. 3.:
Fig. 3.: Study flow diagram.
DiscussionThe main prerequisite for upper endoscopy is a sufficiently clear mucosa in the upper gastrointestinal tract. In addition to lavage before the procedure, mucosal transparency can be increased by distension of the lumen of the organ under examination by insufflation of air or carbon dioxide, suctioning of the remaining fluid, and rinsing of the mucosa with water with the possible addition of substances with antifoaming and mucolytic effect such as simethicone, n-acetylcysteine and the enzyme pronase [3,20]. In our study, the doses of the individual components of the solution were based on the results of studies already performed, which show that, in particular, the effect and dose of n-acetylcysteine in this indication are not completely clear, and the recommendations given in the Summary of Product Characteristics of the two substances used. Most studies have demonstrated an effect of simeticone in combination with water, with effective doses ranging from 100 to 200 mg [9,10]. Data evaluating the effect of n-acetylcysteine alone are scarce. Most studies have evaluated the effect of solutions containing both substances, that is, n-acetylcysteine together with simethicone at different concentrations. Monrroy et al. demonstrated improved mucosal clarity when using both 500 and 1000 mg of n-acetylcysteine in combination with 200 mg of simethicone and water [13]. Also, Manfredi et al. demonstrated that premedication with 2 ml of simethicone and 600 mg of n-acetylcysteine facilitated significantly better endoscopic visualization of gastric mucosa [14]; however, Elvas et al. did not demonstrate improved mucosal clarity when using a solution containing 200 mg simethicone, 600 mg n-acetylcysteine, and water versus 200 mg simethicone alone with water [17]. Stepan et al. then in their study did not demonstrate improved mucosal clarity when using low doses of the substances, that is, 20 mg simethicone, and 400 mg n-acetylcysteine with water [16]. Therefore, in our study, we chose the maximum recommended daily doses of both substances that can be given to adults of the general population, according to the Summary of Product Characteristics of the State Institute for Drug Control of the Czech Republic, which is 400 mg and 4 ml for simethicone and 600 mg for n-acetylcysteine, respectively, if we do not consider patients with mucoviscidosis, where the doses are higher. The amount of water we used in the solution, 100 ml, as well as the timing of the administration of the solution before gastroscopy, appears to be effective and safe according to the study’s performer [8–19]. Our study showed a significantly higher overall mucosal visibility score in the upper gastrointestinal tract after administration of the solution, with the maximum dose of mucolytic solution compared to the branch without administration of solution or water, when the visibility score was evaluated by the endoscopist performing the procedure. The endoscopists who evaluated the visibility score from the photodocumentation taken did not confirm this result; moreover, when the overall clarity score was compared between endoscopists, there was a significant difference in the scores in virtually all branches, which we see some limitations of this study. We believe that this may be due to an overall better and more comprehensive view of the mucosa by the examining endoscopist during the procedure, compared with endoscopists who assessed mucosal clarity only from the photodocumentation taken. Therefore, in future studies with a similar design, it will be interesting to assess the evaluation among endoscopists, for example, from the video footage taken. This study has increased our knowledge of the issue of upper gastrointestinal mucosal preparation before endoscopy, and based on our results, we can recommend the administration of mucolytic solution with the maximum dose of both substances in clinical practice before upper endoscopy. Further studies should clarify the missing data on this issue, especially the effect of both agents on the detection of pathological lesions in the upper gastrointestinal tract and the effect and effective dose of n-acetylcysteine without its combination with simeticone.
AcknowledgementsThe authors thank Eva Hruskova Reinova, State Institute for Drug Control, Czech Republic, for her help with application for approval of the study by the State Institute for Drug Control. This work was supported by the Agel Educational and Research Institute (grant number: INT2021005). The funder played no role in the study design, analysis, decision to publish, or preparation of the manuscript.
Conflicts of interestThere are no conflicts of interest.
References 1. Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology 2012; 143:1179–1187. 2. Januszewicz W, Kaminski MF. Quality indicators in diagnostic upper gastrointestinal endoscopy. Ther Adv Gastroenterol 2020; 13:1756284820916693. 3. Bisschops R, Areia M, Coron E, Dobru D, Kaskas B, Kuvaev R, et al. Performance measures for upper gastrointestinal endoscopy: a European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. Endoscopy 2016; 48:843–864. 4. Chiu PWY, Uedo N, Singh R, Gotoda T, Ng EKW, Yao K, et al. An Asian consensus on standards of diagnostic upper endoscopy for neoplasia. Gut 2019; 68:186–197. 5. Lai EJ, Calderwood AH, Doros G, Fix OK, Jacobson BC. The Boston Bowel Preparation Scale: a valid and reliable instrument for colonoscopy-oriented research. Gastrointest Endosc 2009; 69:620–625. 6. Hassan C, East J, Radaelli F, Spada C, Benamouzig R, Bisschops R, et al. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Update 2019. Endoscopy 2019; 51:775–794. 7. Kim GH, Cho YK, Cha JM, Lee SY, Chung IK. Efforts to increase image quality during endoscopy: the role of pronase. World J Gastrointest Endosc 2016; 8:267–272. 8. Neale JR, James S, Callaghan J, Patel P. Premedication with N-acetylcysteine and simethicone improves mucosal visualization during gastroscopy: a randomized, controlled, endoscopist-blinded study. Eur J Gastroenterol Hepatol 2013; 25:778–783. 9. Chang W, Yeh M, Hsu H, Chen H, Hu M. Efficacy of simethicone and N-acetylcysteine as premedication in improving visibility during upper endoscopy. J Gastroenterol Hepatol 2014; 29:769–774. 10. Song M, Kwek ABE, Law NM, Ong JPL, Tan JY, Thurairajah PH, et al. Efficacy of small-volume simethicone given at least 30 min before gastroscopy. World J Gastrointest Pharmacol Ther 2016; 7:572–578. 11. Keeratichananont S, Sobhonslidsuk A, Kitiyakara T, Achalanan N, Soonthornpun S. The role of liquid simethicone in enhancing endoscopic visibility prior to esophagogastroduodenoscopy: a prospective, randomized, double-blinded, placebo-controlled trial. J Med Assoc Thai 2010; 93:892–897. http://www.mat.or.th/journal. [Accessed August 2010] 12. Chen HW, Hsu HC, Hsieh TY, Yeh M-K, Chang W-K. Pre-medication to improve esophagogastroduodenoscopic visibility: a meta-analysis and systematic review. Hepatogastroenterology 2014; 61:1642–1648. https://www.researchgate.net/publication/268986386_Pre-Medication_to_Improve_Esophagogastroduodenoscopic_Visibility_A_Meta-Analysis_and_Systemic_Review. [Accessed September 2014] 13. Monrroy H, Vargas JI, Glasinovic E, Espino A, Gonzalez R, Parra-Blanco A, et al. Use of N-acetylcysteine plus simethicone to improve mucosal visibility during upper GI endoscopy: a double-blind, randomized controlled trial. Gastrointest Endosc 2018; 87:986–993. 14. Manfredi G, Berte R, Liritano E, Alicante S, Londoni C, Brambilla G, et al. Premedication with simethicone and N-acetylcysteine for improving mucosal visibility during upper gastrointestinal endoscopy in a Western population. Endosc Int Open 2021; 09:E190–E194. https://eref.thieme.de/ejournals/2196-9736_2021_02#/10.1055-a-1315-0114. [Accessed February 2021] 15. Chang C, Chen S, Lin C, Hsieh C, Lou H, Suk F, et al. Premedication wi
留言 (0)