COVID-19 is widespread diffused, but many studies and reports worldwide have demonstrated that risk of infection and outcomes are socially patterned with the most deprived population groups usually experiencing the worst outcomes [2,3,4,5,6,7,8,9,10,11,12,13,14]. A narrative review of 42 studies, all focused on the first pandemic wave, found an association between socio-economic deprivation and an increased likelihood of contracting COVID-19; the strongest evidence was arisen from three large observational studies. The other compelling association was observed with regard to race or ethnicity [42]. On the other hand, a minority of studies, a number of which incidentally were conducted in Italy, did not show such association or even reported opposing results [15,16,17,18,19,20].
By using the SEHDI, our study allowed us to validly and reliably identify the main factors related to socio-economic deprivation, as demonstrated by the high total explained variance value (74.2%), and to study their impact on COVID-19 incidence and fatality.
The factors and census variables composing the SEHDI included in this analysis were the family structure, the characteristics of the house and the education level, which are known to be associated with the socio-economic status of the population [43]. In particular, the main determinants of socio-economic status considered in our study were: single-member household composition, older age, housing conditions and lower education level.
In agreement with the literature [44], most of the census variables considered in our study highlighted the discomfort of single-member families, especially those composed by an elderly individual due to their greater need for both domestic and personal care.
Regarding the housing conditions, it is well known that adequate housing and hygiene conditions are essential for preventing or limiting the spread of respiratory infections [45]. Indeed, overcrowding living conditions and poor-quality housing challenge social distancing increasing the risk of COVID-19 transmission [2, 3, 8, 22].
In terms of education level, it is well known that low education level negatively impacts health and is correlated with a higher incidence of chronical non-communicable diseases (e.g., cardiovascular diseases, diabetes, respiratory chronic diseases, cancer), which in turn may increase the susceptibility to COVID-19 infection and related mortality [25, 26, 46]. Additionally, low education is often associated with elementary occupations, which have been demonstrated to be correlated with a particularly high rate of mortality from COVID-19 [22]. Furthermore, education is recognised as a strong factor influencing health literacy and correct health behaviours both overall and in the specific COVID-19 context [47,48,49]. During the first epidemic wave in Italy, the already existing mortality gap between the high and low education level population groups further increased and individuals with lower education level were more exposed to those factors increasing COVID-19 mortality risk [50].
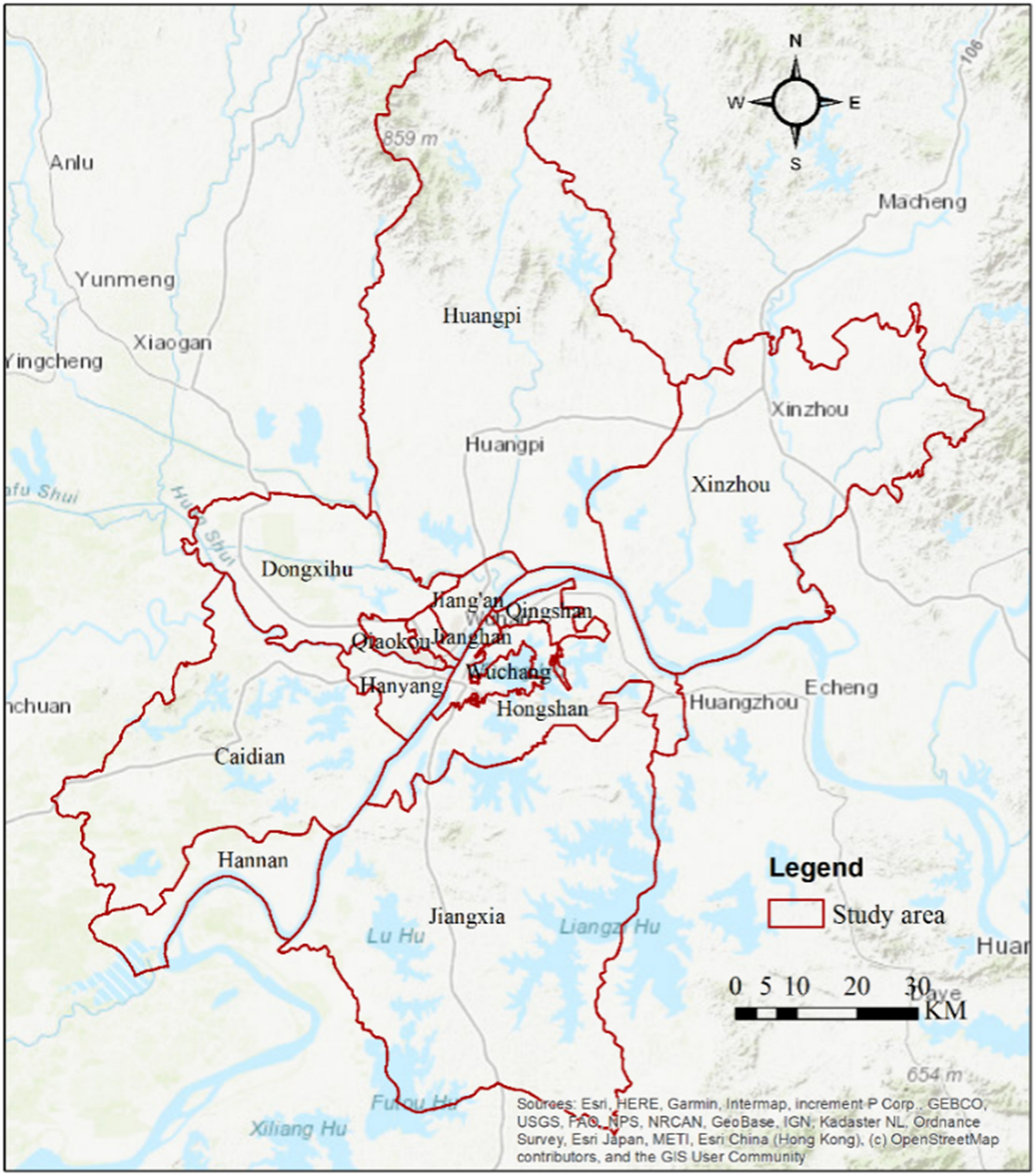
In our study, the most deprived groups lived in the capital city and the main municipalities of Foggia province, where the majority of the elderly population resided. Within the Foggia municipality, the most deprived area was the old part of the city (Southern part of the city centre), which is at a longer distance from healthcare services and has restricted availability of public transport [32]. The lower accessibility to healthcare facilities is known to influence health service utilisation and delay patients care affecting health outcomes [51, 52].
Our study showed that the majority of COVID-19 cases were aged 0–64 years, belonged to medium–low/low deprivation groups, were not employed in the healthcare system and did not have a connection with a nursing home. As for the lack of correlation between COVID-19 and high deprivation observed in our study, which is in disagreement with a part of the literature, a potential explanation behind the observed discrepancy may be the younger age of the population living in the least deprived areas of the Foggia province. Younger individuals may be more exposed to the virus due to occupational and recreational reasons. The younger age of COVID-19 cases was also confirmed by the low connection with nursing homes, the low number of resulting deaths and the low number of comorbidities in the COVID-19 case group.
Secondly, a lower ethnic heterogeneity of the Foggia population compared with most studies in the literature may have removed one of the main determinants of COVID-19 differential susceptibility (i.e., presence of racial minorities). Indeed, most studies in the literature have been conducted in the UK and US, countries with an extremely high ethnic heterogeneity [3,4,5,6, 8,9,10, 21]. Findings from a later phase of the pandemic confirm the different impact of deprivation and ethnicity [53].
Also the SIR distributions by sex, age and age by sex across the SEHDI groups confirmed that the incidence of COVID-19 increased with decreasing deprivation and was higher in the 0–64 year age group. Furthermore, a higher incidence of COVID-19 in men compared with women emerged from our study. Sex disparity in COVID-19 incidence and mortality has extensively been documented in the literature. Women seem to mount a stronger immune response to infections, being protected by oestrogens and being more inclined to preventive care, healthy lifestyle, and hand hygiene [54,55,56].
The lack of association between fatality and socio-economic status of COVID-19 cases observed in our study is in disagreement with some studies [2,3,4,5,6,7,8,9,10,11,12,13,14]. Compared with the other European countries, the Italian population is known to be less affected by mortality-related social inequalities thanks to the protection of the Mediterranean diet, family support and the universal character of the healthcare system [50, 57]. As opposed to our study, the similar Italian study conducted by Di Girolamo et al. in the Emilia Romagna region demonstrated a higher mortality burden in the most deprived areas of the region. [30]. This discrepancy could be explained by the different pattern of diffusion of COVID-19 and different COVID-19 case fatality rate during the first epidemic wave between the two Italian regions which prevent a meaningful comparison of the data. Based on the ISS-Istat report published on March 2021, 26,564 COVID-19 cases and 4238 COVID-19 deaths were reported in the Emilia Romagna region compared with 4804 cases and 537 deaths in the Apulia region during the first epidemic wave (March–May 2020) [25, 26]. During this period, the percentage of COVID-19 deaths observed in the Emilia Romagna region over the total of COVID-19-related deaths in Italy was nearly 8 times higher compared with the number reported in the Apulia region [50].
Knowledge gained as the epidemic progressed revealed that the impact of deprivation on COVID-19 outcomes has been different in the subsequent waves and varied from country to country. Studies conducted in Spain, Belgium, and Germany, observed, from the first to the last wave, an increasingly detrimental trend for the deprived subgroups or even a small advantage in terms of incidence from living in a disadvantaged area. [17, 20, 58]. These findings differ from what has been observed in the UK, where incidence during the second wave increased more in less deprived areas than in more deprived areas [59].
Multiple factors have been invoked to account for this variability, some of which, such as the diffusion of knowledge of the risk factors and the adoption of preventive behavior related to individual awareness, are inversely related to deprivation level [17, 30]. Furthermore, fake news and conspiracy theories rapidly spread online during the first wave of the COVID-19 pandemic generating confusion and insecurity among the population and potentially leading to serious implications for the individual and community [60,61,62,63]. Such misinformation regarded an exaggeration by the experts about the disease severity and the extent of virus spread, and the cause of the disease itself, among other factors [60, 61]. In such a context of misinformation, the education level appears to have contributed to health inequality as communities with lower education levels are more likely to believe in fake news leading to an increased risk of SARS-CoV-2 infection or worse disease outcome [64,65,66,67].
A study that followed the entire evolution of pandemic in the Apulia Region [19] suggests that deprivation has a greater impact the greater is the viral circulation and the fewer are the restrictions. In our study, the burden of deprivation may have been somewhat mitigated due to the fact that we addressed the first wave, when a total lockdown was imposed and when Apulia was a region with a low incidence compared to other Italian regions.
Furthermore, the lack of correlation between socio-economic status and COVID-19 fatality observed in our study may be explained with the higher incidence of COVID-19 among the least deprived population groups of the Foggia district, which may be more exposed to SARS-CoV-2 virus for occupational reasons (e.g. work-related travel to high risk areas) and lifestyle. This portion of the population resides in urban areas with prompt access to healthcare facilities and live in better conditions. Another explanation for the lack of association between fatality and socio-economic status could be the younger age of COVID-19 cases, that represents an enhancement in the survival probability.
Similarly, Gadeyne et al. reported [15], during the first COVID-19 wave in Belgium, higher excess mortality among certain subgroups, specifically high-income men aged 25–64 years, middle- and high-income men and women aged 65–84 years, and non-resident men and women aged 85 years and over. These results were ascribed to an increased risk of infection through leisure and work-related travel for the younger, affluent, and active subgroup, and to the interfamilial exposure and transmission for the older subgroup.
On the other hand, a significantly lower case fatality rate among healthcare workers (0.7% in the healthcare worker group vs. 16.8% in the non-healthcare worker group) emerged from our study. This is in line with the overall Italian trend and may be explained by more frequent testing of healthcare workers compared with the general population enabling faster detection of asymptomatic or mildly symptomatic cases [1]. A low case fatality rate among healthcare workers has also been reported worldwide by a systematic review and meta-analysis including 594 records [68].
This work has some strengths and limitations. The robust model adopted providing an accurate picture of the Foggia population by SEHDI alongside a detailed analysis of the main socio-economic, demographic and clinical factors that could have an impact on COVID-19 incidence and fatality may be considered a strength. Furthermore, the low ethnic heterogeneity of the Foggia population may have limited the weight of a determinant which was not the subject of our analysis.
A major limitation is the unavailability of the number of people tested, rather than of positive cases. It has been reported that disadvantaged people are less likely to be tested and more likely to test positive, be hospitalised or die [12, 58]. This seems to have been particularly prevalent during the first wave due to the scarcity of testing, [13, 14, 17, 58] which was reserved to symptomatic or moderate-severe cases and could represent a bias masking/underestimating the actual incidence of COVID-19 cases among the most deprived population.
Another limitation, though shared with the most studies evaluating the relation between deprivation and COVID-19 dynamics, is the adoption of a composite measure of deprivation, with the intrinsic difficulty to discriminate the role of each factor contributing to the SEHDI score.




留言 (0)