
記住我







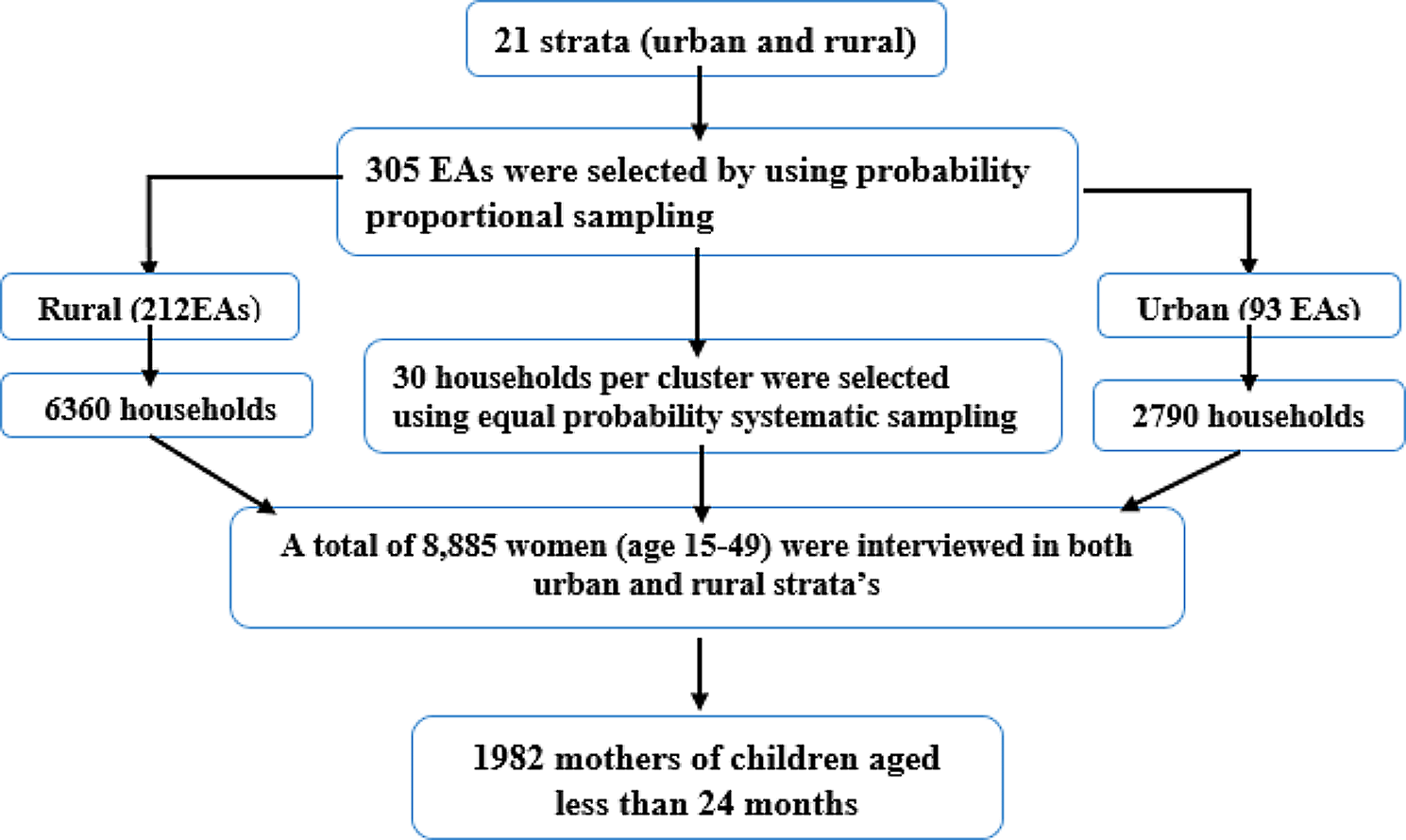
It can be seen in Table 1 that the total numbers of live birth of under-3 children were 2,994 in the last three years preceding the survey. Table 1 also shows the mother and child characteristics, which includes survival status of the child, sex of the child, number of births by mother, age of mother, education of mother, place of residence of mother, caste of the mother, wealth status of mother, relationship of the mother with household head, religion of mother, types of cooking fuel used in house and the mothers work and breastfeeding interaction. From a total of 2994 live births 85 children had died within 36 months of birth.
Table 1 Frequency distribution of maternal and child characteristics for under-3 death in Nepal 2012–2014Looking at Table 2 it can be seen that the risk of death of under-3 children from a mother who does not have education is 28% higher as compared to mothers who have some education (HR 0.722, P value < 0.05, 95% CI 0.65, 0.79). This is supported by the findings from the survey data from 17 developing countries regarding the positive statistical association between maternal education and the health and survival of under-2 years children on post neonatal risk, undernutrition during the 3–23month period, and non-use of health services [14]. Maternal education has a strong positive impact on child survival. Uneducated mothers have the highest risk of child mortality. Mother’s education is a strong determinant of child survival in India, Tanzania, and Ethiopia [15,16,17].
Table 2 Results of the Cox hazard analysis for selected predictor variables associated with under-3 mortality, NDHS 2012–2014Similarly, the risk of death of under-3 year old children other than nuclear family is 51% higher (HR 1.51, p value < 0.05, 95% CI 1.37, 1.655). The prevalence of malnutrition in the two rural areas of Peshawar is 35% in children under three years of age. Both socioeconomic factors (large family size of 87% respondents) and maternal factors were responsible for its high prevalence [18]. A study done in Pakistan found that the education of the mother, birth order number, preceding birth interval, size of child at birth, breastfeeding, and family size were found to have a significant effect on child mortality [19].
Further, the risk of death of under-3 children in the first baby is 84% higher as compared to the second and third baby of mothers. A Comparative Analysis of child mortality from 39 countries and a study from India found that mortality and risk of dying chance of first children compared to those born in middle and last-born child shown to be higher than average while other factors are controlled [20, 21]. Likewise, the risk of death of under-3 children from a mother who is not a household head is 55% higher (HR 0.45, p value < 0.05, 95% CI 0.31, 0.65). It was further supported by the theory of family development and structure and feministic perspectives, according to this theoretical perspective, women experience changes over time such as when the family structure changes from extended family to nuclear family system. In a nuclear family the decision-making power of a woman is high, independent of making decisions, and will involve income-generating work [10].
Further Table 2 also shows that the risk of death of under-3 children from a mother who does not work and does not breastfeed her child is 57% higher (HR 0.42, p value < 0.05, 95% CIs 0.24, 0.75). This was supported by the study done in 26 developing countries of sub-Saharan Africa, South Asia and the Middle East. Using demographic health survey findings from logistic regression analysis this study shows that maternal work is associated with a 24.5% higher risk of child mortality as compared to those mothers stay at home [22]. Furthermore, the risk of death of under-3 children from other than rich families is 61% higher (HR 0.39, p value < 0.05, 95% CI 0.331, 0.46). This result is justifiable as rich quintiles families can supply sufficient nutrients for the child and mother [23].
A study from North India found that socioeconomically advantaged children had significantly lower death rates [24] and women and children from the poor wealth quintile have a greater disadvantage in all indicators of women and child health [25]. Likewise, a State-Level Analysis of the correlation between wealth and health of India found a positive correlation between children’s health and the economic growth of the country from 1990 to 2007 [26].
The risk of death of under-3 children from the Terai caste of Nepal is 35% higher than other castes of Nepal. This result is strongly supported by the study done in north India, that found that the scheduled tribes and scheduled castes having poor wealth quintile and northern Indian women and children are at a greater disadvantage in all indicators of women and child health as compared to other groups [25]. Furthermore, the risk of death of under-3 children from the Hindu population is much lower than other religions, as Hindu people enjoy more social support and access to formal health facilities. The study in Mozambique also found that in the predominantly Christian area, church membership increases the likelihood of getting social support and high access to healthcare facilities, [27]. Likewise, findings from Nigeria suggest that age, place of residence, educational status, wealth index, and religion of fathers and mothers are major determinants of childhood mortality [28].
Figure 1 presents the Cox proportional hazards regression analysis which presents the probability of survival of children below 3 years of age based on the status of the interaction of the mother’s work and her breastfeeding interactions. Interactions of the mother’s work and breastfeeding status are divided into 4 categories and the probability of survival of the child is clearly shown in the Figure. It can be seen from Fig. 1 that the survival of children from mothers who were working and breastfeeding was higher than other categories. The Figure also shows that the survival status of the children from the mothers who were not working and who were not breastfeeding their children was the lowest among the 4 categories, as shown in the blue line. Further child survival status of the mothers who were breastfeeding but not working is second after mothers who were both breastfeeding and working.
Fig. 1
Prediction of survival of child by the caste of mother and paid maternity, 2012–2014, Nepal
Furthermore, the survival status of the children of mothers who were working but not breastfeeding was below mothers who were both working and also breastfeeding their babies. The survival status was above the mother who was working but not breastfeeding their child and the mother who was neither working nor breastfeeding.
Limitation of the studyData used here may have some recall bias. For example, dependent variables may have recall bias as respondents are asked about the events as far back as three years before the day question is asked. Another issue regarding dependent variable is that survey is cross-sectional, so it does not follow the children until they reach three years old, and unfortunately, some children are likely to die before reaching three years of age although they are alive during the survey time and date. It is also possible that whatever led to the child’s death also led to cessation of breastfeeding; thus, cause and effect could be reversed.
留言 (0)