
記住我









Anterior cruciate ligament (ACL) injury is an increasingly common knee injury in young athletes participating in jumping, cutting and pivoting sports.1 2 Despite lengthy rehabilitation, often exceeding 9–12 months, only 65% of people return to their preinjury level of sport following an ACL injury.3 Many ACL-injured individuals report ongoing pain, poorer knee function and reduced quality of life (QOL) than uninjured individuals.4–8
Sex (female/male/intersex determined by biological characteristics)9 and gender (woman/girl/man/boy/transgender/non-binary relating to socially constructed roles and behaviours)10 can influence ACL injury outcomes independently. Sex and gender can also interact.11 Despite being distinct and non-binary, sex and gender are rarely defined and often erroneously used interchangeably (ie, woman and man are used to describe sex, or female or male are used to describe gender) in sport and exercise medicine research. This practice makes it difficult to interpret study findings,12 and challenging to synthesise sex and gender data.
Female athletes/women/girls experience a 2–6 fold higher risk of ACL injury than male athletes/men/boys, thought to be due to a complex interaction of multiple factors (eg, anatomical, biomechanical, neuromuscular, environmental).9 13 Sex and/or gender disparities may exist following ACL injury.14 Female athletes/women/girls are less likely to return to preinjury sports,3 experience more instability15 and exhibit greater psychological distress15 after ACL reconstruction (ACLR) than male athletes/men/boys. Less is known about sex and/or gender differences in broader physical activity (eg, leisure pursuits) and knee-related outcomes (eg, function, QOL).
‘Individuals’ perceptions of their physical activity, knee function and QOL after ACL injury can be measured with valid self-reported measures accessible in clinical and research settings.16 17 Sex/gender differences in ACLR outcomes were synthesised in 2014, but focused on adults following ACLR and did not assess risk of bias or certainty of evidence.15 18 Therefore, this systematic review and meta-analysis aimed to investigate whether sex and/or gender differences exist in perceived activity and knee-related outcomes, regardless of age, initial ACL injury management and rehabilitation.
MethodsWe conducted this systematic review and meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)19 and PRISMA in Exercise, Rehabilitation, Sport medicine and SporTs science20 guidelines (online supplemental appendix 1). The protocol was prospectively registered with PROSPERO (CRD42021205998, 3 August 2021).
Study selection and eligibility criteriaStudies were included if they reported self-report activity or knee-related outcomes in female athletes/women/girls and male athletes/men/boys after an ACL injury. Inclusion criteria were: (1) at least 10 females/women/girls and 10 males/men/boys, of any age, after ACL injury with or without surgery and (2) a sex and/or gender analysis and/or sex-stratified and/or gender-stratified data on any self-reported activity or knee-related outcome and/or return to sport (RTS). Studies also had to focus on primary ACL injury—studies that included >15% of participants with reinjury or revision ACLR were excluded to minimise heterogeneity. ACL injuries were confirmed by imaging, arthroscopy or positive clinical tests and manuscripts written in English, Portuguese or Spanish were included. Studies that included an uninjured comparison group were included if data for the ACL injured population was presented separately by sex and/or gender. Studies of operative management using synthetic ACL grafts or ACL revisions only were excluded. Reviews, case reports, editorials, conference abstracts, clinical commentaries, dissertations or unpublished studies were also excluded.
Search strategyWe searched seven electronic databases (CINAHL, Cochrane Central Register of Controlled Trials, Embase, Medline, PsycINFO, Scopus and SportDiscus) from inception to December 2021. The search strategy was built around three main concepts of ACL injury, sex/gender, and outcome measures, and adapted for each database (online supplemental appendix 2).
We limited the search strategy to include self-reported activity or knee-related outcome measures that have undergone psychometric evaluation,16 and frequently used questions of activity and function such as RTS/physical activity and perceived knee function, respectively (as these elements impact on knee satisfaction.21 22 The main ACL outcomes specifically searched included: Knee injury and Osteoarthritis Outcome Score (KOOS), International Knee Documentation Committee Subjective Evaluation Form (IKDC), International Physical Activity Questionnaire, Lysholm Knee Score, Tegner Activity Scale, Cincinnati Knee Rating System, Marx Activity Scale, ACL-QOL questionnaire and RTS (online supplemental appendix 3).
Reference list scanning of included studies and citation tracking was conducted using Web of Science. All studies identified from searches were loaded into Covidence (Veritas Health Innovation) and duplicates removed. Two authors (paired by their experience level from a pool of eight: AMB, EAR, MH, JM, MFP, JLW, LT and MGK) independently screened titles and abstracts against inclusion criteria. To determine final inclusion, full texts of potentially relevant studies were retrieved and evaluated independently against the eligibility criteria by at least two of eight authors (less experienced: EAR, MH, LT and JM matched with more experienced AMB, MFP, JLW and MGK). For feasibility, we did not contact the study authors for additional information to determine eligibility. Two additional reviewers (AMB and MGK) cross-checked the final selection of articles, with disagreements resolved by a third reviewer (AGC) as reported previously.23
Data extractionOne author of six authors (AMB, LT, EAR, MGK, KC and JLC) independently extracted data using a standardised form, with all extracted data checked by a second author from the same pool. Extracted data included: publication information, study design, study aims, standardised rehabilitation (yes/no), evidence-based rehabilitation (yes/no/not reported), participants (number, females/males/intersex/women/men/girls/boys/other gender, age, height, weight, body mass index), ACL treatment (operative or non-operative management, concomitant injuries), preinjury activity level, length of follow-up (ie, post-ACL injury, post-ACLR), the physical activity or knee-related outcome measure assessed (online supplemental appendix 3),16 17 sex-specific and/or gender-specific results (ie, for continuous data: means, SD, median, ranges, IQRs, standardised mean difference (SMD) and 95% CI; for dichotomous data: number who did and did not RTS or OR and 95% CI), and/or analysis, and main conclusions. We defined evidence-based rehabilitation as supervised rehabilitation/physiotherapy (≥6 months), including structured agility and landing exercises, followed by an independent return to structured gym exercises and return to activity with supervised full RTS (where applicable).24 25 RTS was operationalised as returning to any sport or level.
Data synthesis and statistical analysisTo aid in clinical interpretability, meta-analyses were conducted when two or more studies were considered homogeneous (ie, the same outcome and follow-up). Sex and/or gender was considered as one construct (sex/gender) as these terms were often used interchangeably, making it impossible to separate them. Additionally, sex/gender was treated as dichotomous (female athletes/women/girls compared with male athletes/men/boys) based on familiarity with ACL literature treating sex/gender as binary. To examine sex/gender differences for each activity (including RTS), and knee-related outcomes (including perceived knee function), we pooled the SMD or OR, grouped by time from an ACL injury for those non-operatively managed (ie, ACL deficient) and time post-ACLR/repair for those operatively managed. This approach aimed to group individuals with similar musculoskeletal impairments and rehabilitation goals recognising some delays between ACL injury/ACLR will exist. The follow-up groupings were preoperative, 0 to <12 months post-ACL injury/ACLR, 1 to <5 years post-ACL injury/ACLR, 5 to <10 years post-ACL injury/ACLR, ≥10 years post-ACL injury/ACLR. Missing data (eg, SDs), OR analysis preparation (ie, transforming to log OR) or converting OR (upper band, lower band) to SMD (95% CI) were calculated using the methods described in the Cochrane Handbook.26 All meta-analyses were conducted using fixed-effects models to account for systematically varying results between large and small studies27–29 in Stata V.15.1 (StataCorp) and reported as SMD (95% CI). If a study reported data at 1 and 2 years post-ACL injury/ACLR, 1-year data contributed to the 0 to <1 year meta-analyses and the 2-year data were allocated to the 1 to <5 year meta-analyses. The proportion of the total variability that is plausibly due to between-study statistical heterogeneity was examined using the I2 statistic, where a value of 0% indicates no observed heterogeneity, <25% was considered to have low levels and 100% indicated a completely heterogeneous sample.30 Weighted mean differences were calculated for all continuous data to enhance clinical interpretation and applicability. We further explored between-study heterogeneity by comparing results from studies grouped by age (adolescent (<19 years old) vs adults), initial management (operative vs non-operative), rehabilitation (ie, met evidence-based guidelines) and individual study RTS definition (return to preinjury sport vs return to any sport) using stratified meta-analyses. Meta-regression was used to further explore between study heterogeneity by comparing if individual study effect size differed according to several study characteristics (ie, sample size, mean age, body mass index). When meta-analyses were not possible, we reported means, SDs and/or effect sizes as reported in the original study for individual study outcomes, and qualitatively synthesised any sex/gender difference as none, females/women/girls inferior outcomes compared with males/men/boys, females/women/girls superior outcome compared with males/men/boys.
Risk of bias and certainty of evidenceFive teams of pairs (AMB/MGK, JLK/MH, SLC/SMC, JM/MFP and AME/TJW) independently assessed risk of bias of included studies using the modified Newcastle-Ottawa Scale31 (online supplemental appendix 4) or Cochrane ROB232 for observational studies and randomised controlled trials (RCTs), respectively. All modified Newcastle-Ottawa Scale criteria were operationally defined relevant to our review aims, discussed in detail, tested on different study designs before approving at a consensus meeting prior to assessment. Consistent with recommendations,33 observational studies were rated as high or low risk of bias, while RCTs were rated overall as low (all domains low risk), unclear (all domains low or unclear risk) or high risk of bias (one or more domains high risk). Cohen’s kappa assessed the extent of agreement between risk of bias assessors, where a kappa value ≥0.75 was deemed excellent agreement.34
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system was used to evaluate the certainty of evidence for each meta-analysis.35 An RCT began as the highest quality of evidence, while observational studies were considered low. Downgrading occurred based on predetermined criteria: (1) risk of bias (methodological heterogeneity); (2) inconsistency (statistical heterogeneity); (3) indirectness; (4) imprecision and (5) publication bias) (online supplemental appendix 5). Publication bias secondary to small study effects was assessed using funnel plots and the Egger’s test for any meta-analysis including ≥10 studies.
Any discrepancies in study selection, data extraction and risk of bias assessment were initially resolved through discussion, and mutual consensus, with a third reviewer (AMB, AGC or MGK) consulted if consensus could not be reached.
Equity, diversity and inclusion statementOur study investigates sex and/or gender differences after ACL injury. Given that these terms are rarely defined and often erroneously used interchangeably and treated as binary, we chose an encompassing term sex/gender and were limited to dichotomous variables for our analyses (ie, females/women/girls and males/men/boys). We acknowledge that this may have resulted in some people being misclassified and does not represent people for whom gender or sex is not binary or gender is fluid. To understand the diversity and inclusivity of source study samples, we extracted sociocultural factors including race/ethnicity and education. The author group included diverse perspectives, including those of women and men, clinicians (physiotherapists) and clinician scientists with a diversity of career stages (research assistants, PhD candidates through to professor), and members of the LGBTIQA+ community. We acknowledge the majority of authors are from one country, and lack the perspectives of persons from middle-income to low-income countries.
ResultsStudy selectionFrom an initial yield of 11 034 potentially eligible studies, 236 studies met eligibility criteria (figure 1). Seventy-three per cent (1912/2614) of excluded studies did not report sex-stratified/gender-stratified data and/or did not investigate sex/gender differences on activity or knee-related outcomes. Manual searching identified six additional studies, resulting in 242 included studies (online supplemental appendix 6).
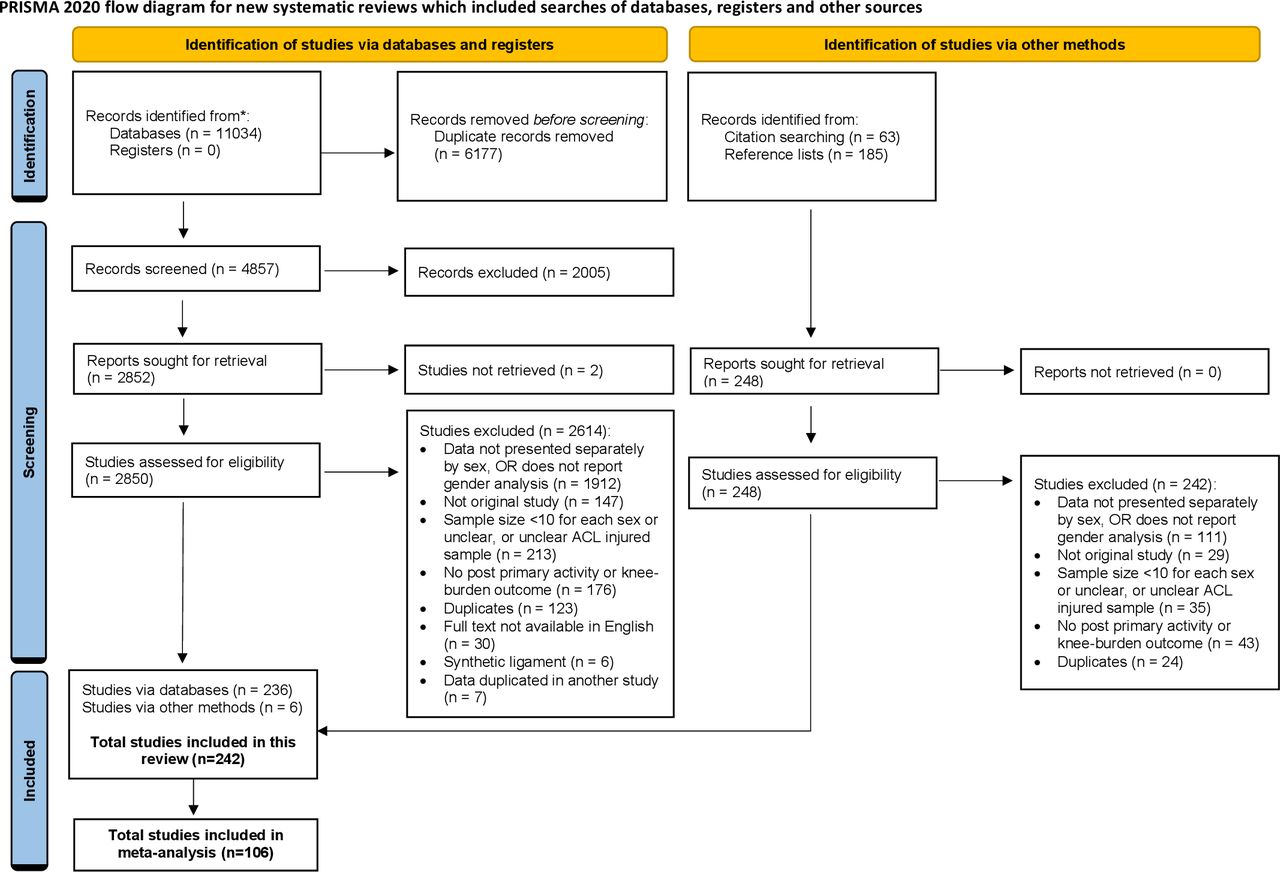 Figure 1
Figure 1 Flow chart of included studies. ACL, anterior cruciate ligament; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristicsData were extracted from 242 studies (7 RCTs, 235 observational/cohort), including 123 687 participants (43% females/women/girls, mean age 26 years at ACL surgery), aged between 10 and 64 years at ACL injury or follow-up, most (94%) operatively managed, and follow-up ranged from 2 months to 31 years post-ACL injury/ACLR (online supplemental appendix 7). Notably, only 13 studies included an exclusively non-operatively managed group36–48; however, 25 studies reported preoperative (7 meta-analyses) data. Six studies included both operatively and non-operatively managed individuals.49–54 Eighteen self-reported measures of activity or knee-related outcomes were identified. Twenty-seven (11%) studies reported participant sociocontextual characteristics (eg, education, ethnicity). One hundred and six studies reported data sufficient for meta-analyses, one with a non-operative population (111 people).42 45 Reasons for precluding pooling of 136 studies included: insufficient data (eg, only p values reported, incomplete sex-stratified/gender-stratified data, single statements of sex/gender significance and/or effect size results, unclear follow-up period) or outcomes used by single studies (online supplemental appendix 8).
Risk of bias and certainty of evidenceFor observational studies, ‘sample size’ and ‘non-respondent’ criteria were most frequently rated as high risk of bias, while ‘selection of the reference (males/men/boys) cohort’ and ‘assessment of outcome’ criteria were most frequently rated as low risk of bias irrespective of publication date (online supplemental appendix 9). Most RCTs were assessed as having at least some risk of bias concerns,55–59 with one assessed as having an overall high risk of bias.48 Agreement between reviewers was excellent (Cohen’s kappa 0.77). All meta-analyses scored very-low certainty evidence using the GRADE system (online supplemental appendix 5). Publication bias was examined in six meta-analyses that included ≥10 studies. There was no evidence of publication bias except for the Lysholm scale at 1 to <5 years post-ACL injury/ACLR, where studies were more likely to be published if females/women/girls experienced a worse outcome (Egger’s test p=0.048) (online supplemental appendix 10).
Activity outcomes (including return to any sport or level)Activity outcomes were assessed in 152 (63%) studies (online supplemental appendix 7). RTS was the most frequently used measure of activity (n=81), followed by the Tegner Activity Score (n=59), Marx Activity Scale (n=13), and Cincinnati Sports Activity Scale (n=5). Less frequently used physical activity-oriented questionnaires included: Godin-leisure time exercise (n=2), Minnesota physical activity (n=1), and Hospital for Special Surgery Paediatric Functional Activity Brief Scale (n=1). Very-low certainty evidence from seven out of eight meta-analyses across activity outcomes (ie, RTS, Tegner Activity Score, Marx Activity Scale), including 72 studies (15 814 participants), found females/women/girls had inferior outcomes compared with males/men/boys after ACL injury/ACLR (figures 2 and 3).
 Figure 2
Figure 2 Summary of return to sport meta-analysis by follow-up period. Note—three studies presented data separated by different ACL treatment or age groups, nine studies contributed data to >1 meta-analysis. ACLR, anterior cruciate ligament reconstruction; GRADE, Grading of Recommendations Assessment, Development and Evaluation.
 Figure 3
Figure 3 Summary of activity and knee-related outcome by follow-up period. ACLR, anterior cruciate ligament reconstruction; GRADE, Grading of Recommendations Assessment, Development and Evaluation; IKDC, International Knee Documentation Committee; SMD, standardised mean difference; WMD, weighted mean difference.
Return to sportData pooled from 61 studies found that, compared with male athletes/men/boys, female athletes/women/girls had approximately 25% reduced odds of returning to sport (figure 2, online supplemental appendix 10). Observed effect sizes ranged from OR 0.75 (45 studies, 95% CI 0.69 to 0.82, I2 13.1%) at 1 to <5 years post-ACL injury/ACLR, to OR 0.77 (9 studies, 95% CI 0.57 to 1.04, I2 48.6%) at 5 to <10 years post-ACL injury/ACLR (figure 2, online supplemental appendix 11).
Tegner Activity ScaleFemale athletes/women/girls exhibited inferior levels on the Tegner Activity Scale at most times post-ACL injury/ACLR compared with male athletes/men/boys (figure 3, online supplemental appendix 11). Observed effect sizes ranged from SMD −1.68 (5 studies, 95% CI −1.82 to −1.54, I2 98.1%) preoperatively, to SMD −0.13 (9 studies, 95% CI −0.21 to −0.04, I2 74.2%) at 1 to <5 years post-ACL injury/ACLR.
Marx Activity ScaleFemale athletes/women/girls experienced inferior activity outcomes on the Marx Activity Scale than male athletes/men/boys at ≥10 years post-ACL injury/ACLR (3 studies, SMD −0.12, 95% CI −0.19 to −0.06, I2 97.3%, figure 3, online supplemental appendix 11).
Qualitative narrative synthesis of activity outcomesQualitative synthesis generally displayed no consistent sex/gender differences in activity outcomes (online supplemental appendix 8). Studies unable to be pooled in existing meta-analyses evaluated RTS (n=17), Tegner Activity Scale (n=43) and Marx Activity Scale (n=4). In summary, findings included RTS (1 observed a significant difference, 16 did not), Tegner Activity Scale (11 observed a significant difference, 22 did not, 10 unclear) and Marx Activity Scale (2 observed a significant difference, 1 did not, 1 unclear). These studies and others assessing the Cincinnati Sports Activity Scale (n=4), Minnesota Leisure Time Physical Activity Questionnaire (n=1) Hospital for Special Surgery Paediatric-Functional Activity Brief Scale (n=1) and Godin Leisure-Time Exercise Questionnaire (n=2) unable to be included in meta-analysis generally displayed no consistent sex/gender differences.
Knee-related outcomesKnee-related outcomes were assessed in 158 (65%) studies (online supplemental appendix 7). The IKDC was the most frequently used (n=80), followed by KOOS (n=73), Lysholm Knee Scale (n=53), ACL-QOL (n=6), Cincinnati Knee Rating System (n=6), Perceived Knee Function (n=6), Knee Outcome Survey Activities of Daily Living Scale (n=5), Satisfaction (n=4) and single studies used the Hospital for Special Surgery ACL Postoperative Satisfaction Survey, Forgotten Joint Score (Knee) and Western Ontario and McMaster Universities Osteoarthritis Index.
Very low-certainty evidence from most knee-related outcome meta-analyses (70%, 19/27), including 50 studies (44 275 participants), found females/women/girls had inferior outcomes to males/men/boys (figures 3 and 4). The magnitude of differences varied between measures and across time, with KOOS-sport and recreation subscale exhibiting the largest sex/gender differences. Meta-analyses could only be conducted for the IKDC, Lysholm and KOOS subscales.
 Figure 4
Figure 4 Summary of Knee injury and Osteoarthritis Outcome Score (KOOS) by follow-up period. ACLR, anterior cruciate ligament reconstruction; GRADE, Grading of Recommendations Assessment, Development and Evaluation; SMD, standardised mean difference; WMD, weighted mean difference.
IKDC subjective evaluation formFemales/women/girls experienced inferior outcomes always compared with males/men/boys on the IKDC (figure 3, online supplemental appendix 11). Observed effect sizes ranged from SMD −0.26 (n=5, 95% CI −0.47 to –0.04, I2 16%) within 1-year post-ACL injury/ACLR, to SMD −0.08 (n=5, 95% CI −0.15 to –0.02, I2 79.1%) at ≥10 years post-ACL injury/ACLR.
Knee injury and Osteoarthritis Outcome ScoreCompared with males/men/boys, females/women/girls experienced inferior knee-related outcomes on most KOOS meta-analyses (87%, 13/15) within 5 years post-ACL injury/ACLR (figure 4, online supplemental appendix 11). Observed effect sizes ranged from SMD −0.16 (KOOS-symptoms, n=5, 95% CI −0.21 to –0.12, I2 67.3%) to SMD −0.30 (KOOS-sport and recreation, n=7, 95% CI −0.35 to –0.26, I2 98.1%) within the 1-year post-ACL injury/ACLR. Sex/gender differences existed preoperatively on 4/5 subscales, ranging from SMD −0.13 (KOOS-activities of daily living, n=5, 95% CI −0.18 to –0.08 I2 97.9%) to SMD −0.31 (KOOS-sport and recreation, n=5, 95% CI −0.36 to –0.26 I2 99.4%). Pooling of between two to four studies (927 to 4819 participants) showed no sex/gender differences existed on any KOOS subscale ≥10 years post-ACL injury/ACLR (figure 4).
Lysholm Knee ScoreFemales/women/girls experienced inferior outcomes compared with males/men/boys on the Lysholm Knee Score, ranging from SMD −3.74 (n=4, 95% CI −3.96 to –3.53 I2 99.4%) preoperatively, to SMD −0.58 (n=5, 95% CI −0.83 to –0.33 I2 88.2%) at 5 to <10 years post-ACL injury/ACLR (figure 3, online supplemental appendix 11). No sex/gender differences existed at 1 to <5 years post-ACL injury/ACLR (figure 3).
Qualitative narrative synthesis of knee-related outcomesQualitative synthesis generally displayed no consistent sex/gender differences in knee-related outcomes (online supplemental appendix 8). Studies unable to be pooled in existing meta-analyses evaluated IKDC (n=60), KOOS (any subscale) (n=40) and Lysholm (n=43). In summary, findings included IKDC (14 observed a significant difference, 42 did not, 4 unclear), Lysholm (7 observed a significant difference, 43 did not, 1 unclear) and KOOS (ADL 6 observed a significant difference, 12 did not; symptoms 3 observed a significant difference, 14 did not; pain 8 observed a significant difference, 18 did not; sport/rec 7 observed a significant difference, 18 did not, 1 unclear; QOL 6 observed a significant difference, 22 did not, 3 unclear). These studies and others assessing the KOOS4 (n=19 (4 observed a significant difference, 12 did not, 3 unclear), ACL-QOL (n=6), Cincinnati Knee Rating System (n=6), Perceived Knee Function (n=6), Knee Outcome Survey Activities of Daily Living subscale (n=5), Satisfaction (n=4), Forgotten Joint Score (Knee) (n=1) and Western Ontario and McMaster Universities Osteoarthritis Index (n=1) unable to be included in meta-analysis generally displayed no consistent sex/gender differences.
Stratified analysesSex/gender differences observed were generally similar irrespective of age (ie, adolescents or adults) (online supplemental appendix 11, 12). The reduced odds for female adolescent athletes/girls returning to sport compared with male adolescent athletes/boys were similar between studies with a mean age <19 (OR 0.68, 95% CI 0.41 o 1.13, I2 0.0%;) and adults (OR 0.76 95% CI 0.69 to 0.82, I2 21.8%, online supplemental appendix 11). No between-group study heterogeneity existed for any age-stratified activity or knee-related outcome meta-analyses (online supplemental appendix 12). Irrespective of RTS definition, female athletes/women/girls had lower odds of returning to sport compared with male athletes/men/boys within the first 5 years after ACL injury/reconstruction (online supplemental appendix 11). Female athletes/women/girls had poorer RTS outcomes when using return to any sport definition compared with returning to preinjury sport definition at 1 to <5 years post ACL injury/reconstruction (p<0.001, return to any sport OR 0.56 95% CI 0.47 to 0.67, preinjury OR 0.83 95% CI 0.75 to 0.92(online supplemental appendix 11). The lack of non-operatively managed studies (n=2) and reporting of rehabilitation provision prevented the exploration of sex/gender differences between operatively and non-operatively managed ACL individuals and between those that conducted evidence-based rehabilitation or not, respectively. Finally, meta-regression found that sample size, age at ACLR/injury, or body mass index did not explain sex/gender differences (online supplemental appendix 13).
DiscussionThis systematic review aimed to investigate self-reported sex/gender differences on activity and knee-related outcomes after ACL injury. Including 242 studies and 123 687 individuals, very low-certainty of evidence from 26/35 (74%) meta-analyses found females/women/girls experience worse self-report activity and knee-related outcomes within the first 10 years after ACL injury compared with males/men/boys. Preoperative knee-related meta-analyses suggest these similar differences also exist before ACLR (ie, ACL deficient). While many sex/gender differences were small (eg, IKDC two-points worse for females/women/girls, figures 3 and 4) we found an important 25% reduced odds for female athletes/women/girls to RTS within the first 5 years after ACL injury. We also found a likely clinically meaningful difference in difficulty with sport and recreation as measured by KOOS-sport and recreation subscale faced by females/women/girls (10 points worse, figure 4) compared with males/men/boys. Although the differences in many outcomes did not reach previously estimated minimally clinically important thresholds,60 even the presence of a small observed change (eg, 2–5 points on KOOS-quality of life) may be perceived meaningful to females/women/girls.61 Furthermore, no meta-analysis found poorer results for males/men/boys. These findings highlight the importance of improving outcomes for females/women/girls following ACL injury.15 62 63
Higher risk of ACL injuries in females/women/girls is well established.64 We found that females/women/girls (irrespective of age) also have poorer outcomes after ACL injury than males/men/boys, consistent with some previous reviews,15 63 but not others.18 Our current analyses extend findings from these previous reviews by combining data from an additional 165 studies, assessing risk of bias and certainty of evidence using the GRADE system, and grouping meta-analyses by follow-up where patients may be at similar stages of recovery (eg, rehabilitation phase, patient goals, motivation, ongoing symptoms). Risk of bias assessment highlighted the significant under-reporting of non-responder characteristics (79%), leading to potential recruitment bias. In addition, less than half of the studies failed to match males/men/boys and females/women/girls participants (or account for statistically) on important confounding factors (eg, age, body mass index, sport exposure). Therefore, the relationship between sex/gender and outcomes is difficult to isolate. Although inferior outcomes among females/women/girls were found on RTS, Tegner Activity Scale, KOOS subscales, IKDC and Lysholm measures, the results must be interpreted with caution due to the very low-certainty of evidence. Grouping studies by follow-up since ACL injury/ACLR provide insight that knee-related sex/gender disparity varies over time. However, lack of long-term follow-up limits sex/gender differences interrogation beyond 10 years post-ACL injury/ACLR. More studies examining long-term activity and knee-related outcomes are needed.
Why might female athletes/women/girls experience inferior outcomes after ACL injury?Worse outcomes for female athletes/women/girls, particularly in regard to returning to sport and difficulty with sport and recreation, could be due to a complex interaction of many factors—both knee and non-knee related.
BiologicalIt is unclear if biological factors (eg, anatomy, physiology, hormones) are associated with self-reported activity and knee-related sex/gender disparity after ACL injury.62 65 Limited evidence from small studies suggests knee laxity,66 67 and asymmetrical limb behaviour68 69 sex/gender disparities exist in ACL-deficient adults. Increased knee instability may partly explain the worse preoperative knee symptoms and activity limitations as found in six out of seven meta-analyses. However, the detected inferior instrumental knee laxity among females/women after ACLR is minimal—and undetected in clinical examination.15 Worse activity and knee-related function post ACL injury among females/women/girls may also be influenced by sex-based skeletal muscle differences.70 Some studies suggest female athletes/women have weaker quadriceps strength after ACLR compared with male athletes/men,71 72 and lower hamstring activation postlandings,73 others do not.15 18 Hormonal fluctuations throughout the menstrual cycle and associated symptoms74 may also influence exercise performance,75 pain perception and perceived knee difficulties during ACL injury recovery. A greater understanding of the menstrual cycle,76 other biological differences including neuromuscular response to training77 and higher adiposity on knee-related outcomes after ACL injury is needed.
Sociocultural: psychologicalFear of reinjury and lack of knee confidence may prevent female athletes/women/girls from returning to sport at the same rate as their male athletes/men/boys counterparts. Small studies have found that, compared with male athletes/men/boys, females/women/girls more frequently reported fear of reinjury as a reason preventing return to preinjury sports (17% (n=10) vs 2% (n=1)).78 Furthermore, higher self-efficacy post-ACLR, less psychological distress and greater readiness to RTS during rehabilitation may enhance male athletes/men/boys’ confidence to return to preinjury sports compared with female athletes/women/girls.79 80 Male athletes/men/boys are also more likely to endorse competition and winning as motivators for sports participation and exhibit risk-taking behaviour.81 82
Sociocultural: rehabilitationOptimal rehabilitation is critical for ACL injury recovery.83 However, insufficient reporting of standardised and/or evidence-based rehabilitation hindered interrogation of rehabilitation’s impact on preoperative or postoperative sex-based/gender-based differences. Our findings of inferior activity, pain, difficulty with sport and recreation, and quality of life among females/women/girls may indicate that current rehabilitation (prehabilitation and postreconstruction) are inadequate to address their activity limitations and impairments. Existing ACL rehabilitation clinical practice guidelines do not suggest interventions need to differ by sexgender.66 68 84–86 It is unclear if sex/gender differences exist for other preoperative complaints such as joint effusion, lower limb strength and psychological impairments despite reports that knee complaints may vary by age and gender among adults.86 It is also unclear if inherent biases among therapists and coaches preferentially support male athletes/men/boys to return to preinjury sport after ACL injury compared with female athletes/women/girls. A recent call to consider gendered training environment, particularly during resistance training14 would be relevant to ACL rehabilitation. Given that resistance training is often used during evidence-based ACL rehabilitation,87 we must consider the influence of access to equipment, space and discomfort in a man-dominated space during rehabilitation and its influence on outcomes. Further research should consider reporting environmental and social factors by sex/gender.
Sociocultural: social rolesCompeting lifestyle demands and societal roles might also contribute to female athletes/women/girls’ reduced odds of returning to preinjury sport and other inferior outcomes.88 ACL injuries can occur at an age when caring responsibilities, work and/or study demands are at their greatest. Personal lifestyle changes in family commitments, job demands and life stages (eg, getting older) were prominent themes influencing almost half of female athletes/women choosing not to return to their pre-ACL injury sport (n=20).89 Furthermore, unequal time distribution (ie, hours per/day) to health-supportive activities among females/women and males/men leads to health inequities.90 For females/women after ACL injury, reduced physical activity levels are a likely consequence of work, family and unequal household time commitments, unaffected among males/men.
Inherent sex/gender biases and sociocultural factors may also influence responses in some outcome measurement instruments. For example, the Tegner Activity Scale allocates higher scores to moderately heavy labour occupations (eg, truck driving) than light work (eg, nursing).91 Historically, heavy labour is dominated by males/men, which may account for higher scores than females/women. Similarly, a higher proportion of males/men participate in cutting sports than females/women,82 which could explain better outcomes for males/men/boys than females/women/girls.
Clinical recommendationsFemale athletes/women/girls have unique biological and sociocontextual factors that can contribute to a poorer outcome after ACL injury, however information is lacking.10 Perhaps unsurprisingly, only 27 (11%) studies reported participant sociocontextual factors (eg, education, ethnicity, marital status), and only one reported number of children. Clinicians are well positioned as primary practitioners to consider how gendered roles and environments may influence physical and psychological ACL rehabilitation outcomes. For example, exploring past and current training experiences (eg, resistance, leisure pursuits) may highlight the greater need for education, supervision and technique feedback. A peer support group class may be indicated to improve psychological health, well-being and/or exercise adherence. Menstrual cycle monitoring may help to inform exercise planning to optimise rehabilitation performance. It is important to acknowledge that some outcome measures such as the Tegner Activity Scale may disadvantage female/women athletes compared with male/men athletes, because the sport examples provided on the scale are typically male-dominated (eg, soccer, football, rugby). Clinician’s self-reflection on unconscious gender biases, and how they may influence the delivery of education, treatment choice, exercise prescription and training environments are necessary to promote equity in outcomes for female /women/girls athletes after ACL injury.
Research recommendations: priorities to improve outcomes for females/women/girls after ACL injuryTo address sex/gender disparities, we need to understand contributing factors and associations with outcomes. Cohort studies can include sociodemographic questions such as employment status, care-giving roles, social support and health literacy. Interventional trials can improve intervention reporting (eg, dosage, intensity, progression, supervision), and explore mediating and moderating factors to inform clinical practice.92 The validity of previously established outcome measures should be evaluated through a gendered lens to understand if measurement properties differ by gender. Qualitative methodologies can assist in understanding social roles (eg, caring) and supports, and contextual factors (eg, access to treatment, health and medical team culture, gender-neutral training environments) and associations on activity and knee-related outcomes. Including the patient voice to codesign ACL injury prevention, rehabilitation and implementation research will enhance women’s outcomes across the lifespan.88 93 Where feasible, future studies should include data reported separately for all sexes and genders. This will allow researchers to combine data sets where appropriate, to explore relationships, mediating and moderating factors. Collectively, these recommendations are important steps to better understand influencing ACL recovery factors and inequalities between sexes/genders.
LimitationsLack of data separated by sex/gender meant smaller meta-analyses, or no meta-analyses, for some follow-ups, or outcome measures. For example, only 50% of trials examining activity outcomes contributed to meta-analyses. While requesting additional data from authors of included papers may have resulted in more data for meta-analyses, we did not contact any authors due to limited resources and the already large number of included studies (n=242). The meta-analyses results may be influenced by studies only presenting sex-separated/gender-separated findings when significant and may be at risk of confounding due to other unknown factors. The high I2 values suggest heterogeneity between studies exists, but is unexplained by the variables examined. Although we aimed to examine sex and gender (ie, how individuals viewed themselves in society) independently, it was not possible because many of the included studies used the terms interchangeably and did not report if they asked participants to identify based on their biology or sociocultural identity. Only 6% of studies reported race/ethnicity, and combined with limiting to English, Spanish or Portuguese studies, our findings may not reflect experiences of black, Indigenous and people of colour, people from the Global South or Far North, people from low-income or middle-income nations, or people from stateless communities. Future research should aim to report and/or include members of equity-deserving communities including females/women/girls, transgender and non-binary gender, black, Indigenous and people of colour and low-income and middle-income communities in sports exercise medicine research.94 While objective measures of activity are desired,95 the large body of work in self-reported outcomes alone meant we a priori decided to focus on self-reported measures. We operationalised RTS to include any sport or level given the many ways RTS data are collected. However, even our stratified analyses evaluating different RTS definitions could not explore other sport-related factors such as whether participants returned to the same level of competition or performance/skill. Lack of adequate details reported for rehabilitation content and combined injury prevalence (eg, meniscal tears) meant we could not explore the impact of different rehabilitation approaches or presence of a combined injury on sex/gender differences.96 Although we did not limit study inclusion based on age or initial management strategy, generalisability of our findings to paediatric/adolescent or non-operatively managed population is limited due to only 17 and 13 included studies, respectively. Of the 13 exclusively non-operative data studies, 2 were included in meta-analysis, and the others were not due to lack of clinical homogeneity in outcome, time points or statistical estimate. Finally, the very low-certainty evidence for all meta-analyses reflects the high I2 values signalling large amounts of heterogeneity in knee-related data.
ConclusionThis is the first study to synthesise evidence by sex/gender of self-reported activity and knee-related outcomes after ACL injury among adolescents and adults, considering risk of bias and certainty of evidence. The findings highlight the sex/gender outcome inequality after ACL injury—very low-certainty evidence indicates that females/women/girls experience inferior activity and knee-related outcomes on 26/35 (74%) meta-analyses compared with males/men/boys. A concerted effort is required from clinicians, researchers, healthcare funders, gyms/infrastructure to enhance outcomes for females/women/girls. To improve equality for female athletes/women/girls after ACL injury, we need more studies to assess, acknowledge and address sex/gendered factors (eg, menstrual cycle symptoms, psychological factors, access, social support, gender-neutral resistance training environments) during rehabilitation.
留言 (0)