BDTT is a relatively rare but well-known manifestation of HCC. According to the 22nd National Primary Liver Cancer Follow-up Survey Report in Japan (2012–2013), the frequency of bile duct tumor thrombus was 3.4% by imaging diagnosis in all registered cases, including operated and non-operated cases, and 3.2% according to pathological findings [7]. This is lower than the frequencies of portal vein tumor thrombus (imaging, 13.9%; operative findings, 15.9%) and hepatic vein tumor thrombus (imaging, 4.6%; operative findings, 6.5%), indicating that this is a relatively rare form of invasion.
Clinical manifestations of BDTT are often obstructive jaundice and biliary hemorrhage [5, 8]. Jaundice is characterized by the spontaneous resolution of intrahepatic cholangiocarcinoma due to tumor growth and necrosis in the bile duct, and increased intraductal bile duct pressure may be caused by the induction of intraductal pressure due to the induction of tumor necrosis and jaundice, as well as stone-like symptoms, such as pain and vomiting [9].
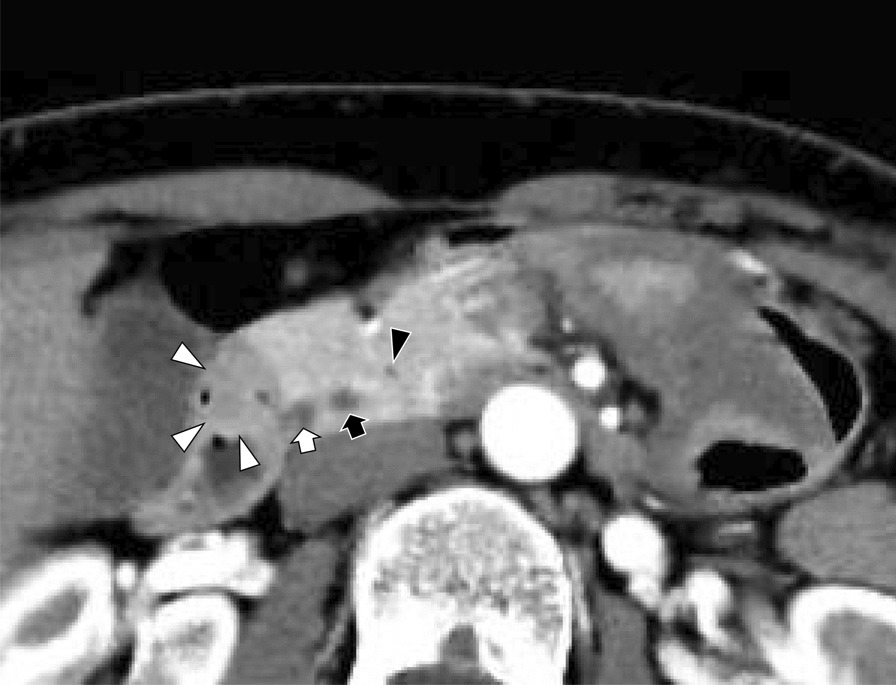
Despite the remarkable progress in diagnostic imaging, it is often difficult to differentiate hepatocellular carcinoma with intraductal growth of the bile duct, especially in cases with obstructive jaundice as the initial symptom and no obvious intrahepatic mass, from hilar bile duct carcinoma or intraductal growth of the bile duct-type hepatoma [10]. Correct preoperative diagnosis has been reported in only 26.5% of cases, indicating the challenges of clinical diagnosis [5]. In the present case, intrahepatic intraductal papillary neoplasm of the bile duct was considered as the primary diagnosis, because the preoperative imaging showed no obvious cirrhosis, the bile ducts were dilated at the periphery of the mass, and the contrast pattern of the tumor was not typical for HCC. The tumor initially appeared to have an internal cystic component, although it was a space between the BDTT and the bile duct wall, and the AFP and PIVKA-II were within the standard values.
Several hypotheses have been proposed regarding the mechanism underlying BDTT development [5]. A distal tumor may grow continuously until it fills the entire extrahepatic biliary system; a fragment of necrotic tumor may separate from the proximal intraductal growth, migrate to the distal common bile duct, and cause an obstruction, and eventually hemorrhage from the tumor may partially or completely fill the biliary tract with tumor-containing blood clots [4, 11,12,13,14]. In the present case, although the tumor was small (2 mm), it is possible that the necrotic tissue of the HCC originating in the hepatic parenchyma near the right hepatic duct may have migrated and developed into BDTT at the right hepatic hilum. As recent studies suggest that HCC with BDTT may arise from liver stem/progenitor cells in the canals of Hering particularly when the primary lesion is very small [15, 16], it is possible that the tumor in this case originated from such a mechanism.
Pathological characteristics include a large tumor diameter, portal vein invasion, often with intrahepatic metastases, and intermediate or poorly differentiated histology [17]. The 5-year survival rate after curative resection is 48%, and poor prognostic factors include tumor size greater than 5 cm, positive vascular invasion, and cirrhosis [8]. As these factors are not compatible with the present case, long-term survival was expected.







留言 (0)