
記住我
Small intestinal bacterial overgrowth (SIBO) is increasingly recognized as a pathophysiological driver of a wide range of gastrointestinal (GI) symptoms, including those that meet the symptom criteria for irritable bowel syndrome (IBS) (1). SIBO is characterized by abnormal bacterial colonization in the small intestine and is associated with GI symptoms such as bloating, distension, flatulence, abdominal discomfort, diarrhea, and, in severe cases, even weight loss and significant micronutrient deficiencies. Certain factors, such as the presence of underlying gut dysmotility or a history of GI surgery, increase the risk that an individual will develop SIBO. Recently, increased methane production via methanogens (microbes that produce methane with carbohydrate fermentation) has been recognized as a potential cause of constipation (and associated symptoms of bloating, gas, and/or abdominal pain) (2–4). Clearly, making a diagnosis of SIBO and/or methanogen overgrowth is critical for the management of patients suffering from a wide range of chronic GI symptoms.
The gold standard test for SIBO—direct culture of small intestinal contents—is technically cumbersome, invasive, costly, and subject to some contention regarding diagnostic thresholds of bacterial counts. Previously, diagnostic criteria for SIBO using aspirates were defined using a threshold of ≥105 cfu/mL, but the North American consensus guidelines and the American College of Gastroenterology (ACG) guidelines recommend a threshold of >103 cfu/mL to define SIBO given evidence that asymptomatic controls rarely exceed 103 cfu/mL, values >103 cfu/mL have been shown to be clinically relevant, and ≥105 cfu/mL was generally seen in patients with altered anatomy (3,5). This threshold is supported in a 16S ribosomal RNA gene sequencing–based study, which found that a culture-based cutoff of >103 cfu/mL correlated well with clinical symptoms, breath test results, and sequencing (6). Debate on the appropriate diagnostic threshold remains, for instance, the Asian-Pacific consensus guidelines support the use of both diagnostic thresholds (7). Variable sampling and processing techniques have been an additional limitation with the use of small bowel aspirates. However, several strides have been made to develop robust methods for small bowel sampling under aseptic, or near aseptic, conditions (3). Despite improved methods to collect and analyze small bowel aspirates, there are limitations to such testing and barriers to widespread implementation. Because breath testing provides an alternative, noninvasive, inexpensive, and relatively straightforward mode of testing, it has been rapidly and widely adopted to aid in the diagnosis of SIBO (8). Yet, the clinical decisions surrounding the use of these breath tests remain poorly characterized. It is critical for clinicians to recognize the strengths and limitations of hydrogen-methane breath testing, how and when to conduct such testing, and the factors that influence the results and the study interpretation.
In this article, we present a comprehensive review the role of hydrogen-methane breath testing to diagnose SIBO. We will cover indications for testing, an overview of the test paradigm, strategies to optimize test performance, and a review of factors that may influence the interpretation of test results. We will then explore the test performance characteristics (sensitivity, specificity, positive and negative predictive values, likelihood ratios, and diagnostic odds ratio [DOR]) that influence clinical decisions on diagnosis and treatment. We will explore testing alternatives and complementary approaches for the diagnosis of SIBO and potential research applications of breath testing. Finally, we report the prevalence of SIBO in various clinical populations and discuss the application of breath testing under different clinical scenarios.
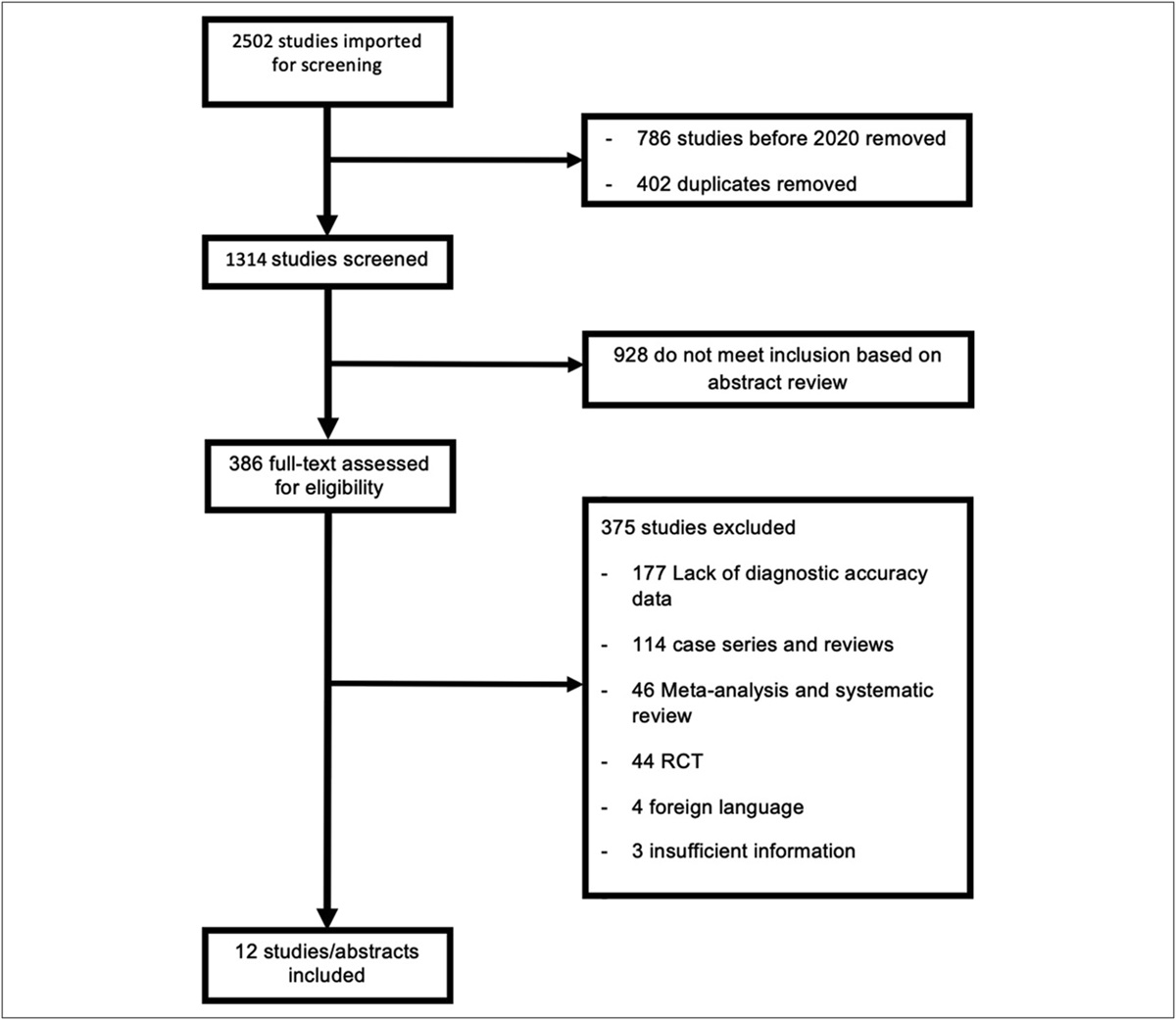
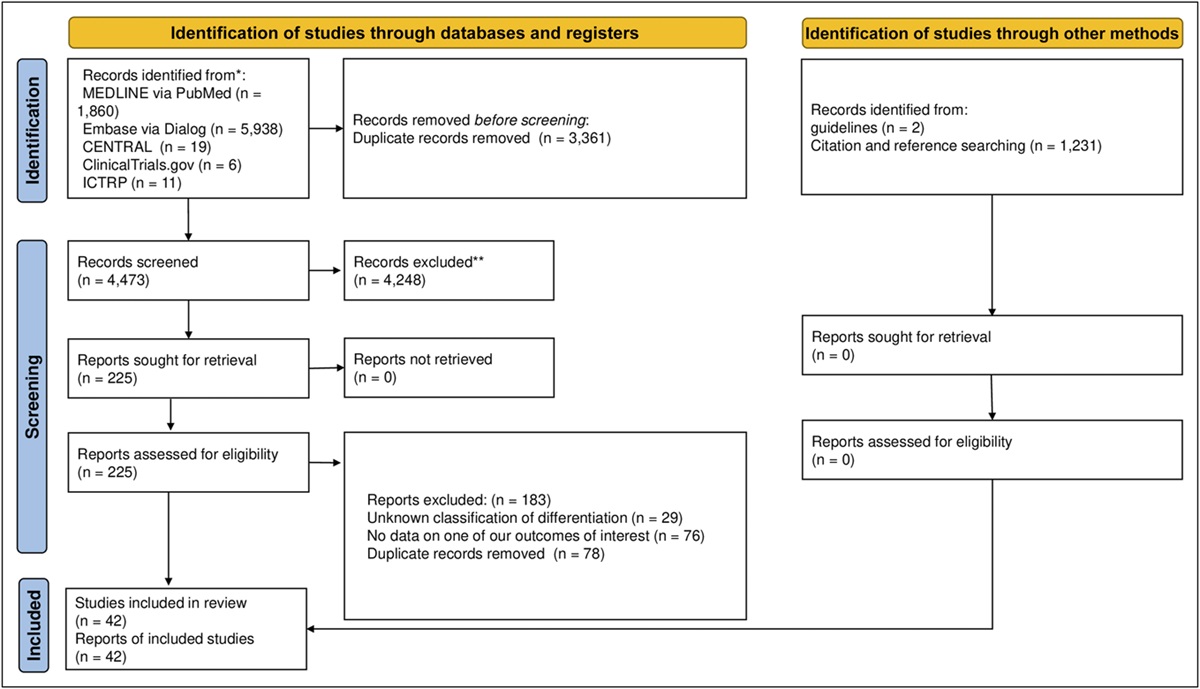
METHODSWe searched PubMed from its inception through January 20, 2023, using a combination of keywords and MeSH terms (see Supplementary Table 1, https://links.lww.com/CTG/A909). We did not apply any search restrictions. Articles were screened first by title and then by abstract for possible relevance to this review. In addition, we hand searched references of relevant articles.
Full-text references were retrieved if articles appeared to be applicable. We extracted information on study protocols used for breath testing preparation.
To determine the diagnostic accuracy (i.e., sensitivity and specificity) of breath testing, we specifically included studies that used jejunal aspirates as a gold standard reference. To determine the prevalence of SIBO in higher-risk populations, we included English-only studies (systematic reviews, randomized clinical trials, cohort, case-control, or cross-sectional studies) that evaluated the prevalence of SIBO in adults (those aged ≥18 years) using breath tests (with lactulose or glucose as the substrate) and/or small bowel aspirates (duodenal or jejunal). As additional a priori study inclusion criteria, the patient population had to include a minimum of 100 patients and sufficient information to determine the prevalence of SIBO in this patient population. We focused on clinical populations that are routinely encountered by gastroenterologists. Furthermore, studies also had to include a control group of patients (either healthy asymptomatic subjects and/or symptomatic patient controls). For prevalence information, we extracted data from all included studies including title, journal, year, study design, number of participants included (if the article was a systematic review, the number and types of studies were also extracted), reference standard test used and definitions of positive tests, prevalence data, and additional information on patient population and control population where available. Because the primary goal was to formulate reliable prevalence numbers to inform clinical applications, we favored the inclusion of systematic reviews rather than individual articles. However, if a large population study was performed and not included in available systematic reviews, those individual studies were additionally included in our analysis. For multiple systematic reviews on the same population, we favored studies with more updated and/or rigorous methodology but considered inclusion of multiple studies if additional prevalence information was provided on the population of interest. For systematic reviews, we assessed the quality of the reported data and rejected meta-analyses in which the between-study heterogeneity (I2 statistic) was reported to be ≥ 90%. Both authors independently extracted data for all included studies and agreed on included studies with excellent Cohen kappa (>0.80). Where statistical calculations were needed, we used Stata 13.1 (College Station, TX).
Indications for breath testingHydrogen-methane breath testing is indicated for the following (1,3).
• Diagnosis of SIBO in symptomatic at-risk populations: ◦ Symptoms generally attributed to SIBO include steatorrhea, weight loss/inability to gain weight, abdominal pain, gas, bloating, distension, diarrhea, constipation, and anemia/neuropathy. In addition, a syndrome of brain fog, gas, and bloating has been described with resolution after discontinuation of probiotics and a course of antibiotics (9). Symptoms of anxiety and depression have also been linked to SIBO, although unclear whether this is directly related to SIBO, in response to symptoms from SIBO, or another mechanism (10). See Table 1 for a list of symptoms compatible with SIBO and their proposed pathophysiological mechanisms. ◦ At-risk populations include patients with motility disorders or who use medications that impact gut motility, those with surgically altered GI anatomy, patients with immunodeficiencies, or altered GI mucosal secretion or gut barrier function. See Table 2 for a list of mechanisms and associated disorders that increase the risk of SIBO. • Evaluation for excessive methane excretion (methane-producing microbial overgrowth) • Detection of specific disaccharidase deficiencies or impaired sugar absorption • Assessment of the responsiveness of GI tract microbial colonization to antibiotic therapy Table 1. - Symptoms implicated with small intestinal bacterial overgrowth and possible mechanisms (116,117) Symptom Possible mechanisms Bloating Multifactorial: increased gas production from bacterial fermentation, visceral hypersensitivity, and decreased small intestinal elasticity and/or transit Diarrhea Multifactorial: bacterial digestion produces gas and osmotically active byproducts, bacteria and byproducts injure mucosa resulting in increased water output, resulting in lactase deficiencies, and bacterial deconjugation of bile salts interferes with fat absorption Abdominal pain Multifactorial: brain-gut, visceral hypersensitivity, and decreased small intestinal elasticity and/or transit Constipation Methane production slows intestinal transit; increased gas distension interferes with intestinal contractions Anemia/neuropathy Bacterial consumption of vitamin B12 Inability to gain weight and weight loss Reduced availability of nutrients due to bacterial digestion Steatorrhea/fat-soluble vitamin deficiencies Bacterial deconjugation of bile acids resulting in insufficient absorption of fats and fat-soluble vitamins Systemic reactions (i.e., brain fog, anxiety/depression, and dermatologic conditions) Multifactorial: increased bacterial counts and intestinal barrier destruction can result in hypersensitivity reactions/immune response; vitamin deficiencies; bacteria and byproducts may traverse the disrupted intestinal barrier Distension Multifactorial: increased gas production from bacterial fermentation; decreased small intestinal elasticity and/or transitGLP, glucagon-like peptide.
We focus our discussion on the diagnosis of SIBO in symptomatic at-risk populations and briefly detail the other indications.
Overview of the testHydrogen-methane breath testing refers to the measurement of components of exhaled gases and can be performed in the office or at home. Hydrogen-methane breath testing relies on an administered oral substrate (generally a solution containing a readily metabolized carbohydrate) that is then metabolized by gut microbiota. Glucose and lactulose are the most commonly used substrates. Glucose is readily absorbed in the proximal small intestine, with much less reaching the colon. Lactulose passes unabsorbed through the small intestine and readily enters the colon. Thus, glucose and lactulose substrates differ in their spatial and temporal interaction with gut microbiota. Lactose and fructose are other substrates used in breath testing, but these substrates are used to diagnose specific malabsorption states, rather than SIBO, and will be briefly discussed separately.
When the patient consumes the carbohydrate substrate, bacterial contact with the substrate results in the production of gases (hydrogen, methane, and hydrogen sulfide) via fermentation (1). Prior tests relied on measuring hydrogen gas only, but overall, there has been a strong shift to support measuring both hydrogen and methane gas (3,11). Hydrogen and methane gases are exclusively produced by intestinal bacteria, and these gases diffuse across the gut mucosa into the portal circulation where they undergo gas transfer in the alveolar spaces and are subsequently exhaled. In healthy individuals, this process is initiated predominantly in the large intestine, where most gut bacteria reside. However, in patients with SIBO, bacterial fermentation of the substrate occurs more proximally within the small intestine. These gases are exhaled with normal tidal breathing and collected in bags at regular intervals throughout the breath testing period (1,3). Inferences about the anatomic location within the gut in which these fermentation reactions occur are based on the temporal pattern of gas production and exhalation following the ingestion of the substrate (3). In general, commercially available gas analyzers detect hydrogen somewhat more accurately than methane, but the measurement of both gases substantially improves the test's overall diagnostic accuracy and is recommended as a standard approach (3). There is increasing interest in measuring hydrogen sulfide gas, but hydrogen sulfide detection capability is not currently incorporated into most gas analyzers used in routine clinical practice (1). In addition, measuring carbon dioxide concentration if available aids not only to identify substandard samples but also allows for normalization of results to potentially improve diagnostic accuracy via correction factors that are applied to measured gas concentrations (12,13). Another less common alternative to measuring carbon dioxide is the measurement of oxygen concentration, which is similarly applied to confirm high-quality sample collection and properly account for sample dilution (3,14,15).
How is the hydrogen-methane breath test performed? Preparations for the test.Because breath testing is so reliant on gas production related to bacterial fermentation of the substrate in the small intestine, preparations before the test are necessary to decrease the presence of hydrogen and methane gases related to bacterial metabolism of substrates from other dietary sources (i.e., colonic bacterial fermentation from previously ingested food) (15). Preparation additionally involves minimizing the effect of medications and lifestyle factors that may alter the results.
Diet.The day before the test, patients should follow a low-residue diet consisting of white rice, fish, chicken, eggs, white (dairy-free) bread, clear broths, and plain black tea or coffee (3,8,15,16). During the restricted diet period, salt, pepper, powdered spices, and herbs are allowed (16). Cooking oil may be used in small amounts (17). A minimum of an 8-hour (ideally 12-hour) overnight fast (water only) is recommended before the test (3,18). Gum chewing and candy should be avoided during the test preparation and testing periods to avoid inadvertently driving bacterial fermentation of sugars (16,19).
Medications.Multiple medications can influence intestinal transit time, thereby affecting breath test interpretation, and if able to be tolerated by the patient, they should be held before testing. For instance, promotility drugs and laxatives should ideally be withheld at least 1 week before breath testing (3). The recent European H2-CH4-breath test group consensus statement recommends that fermentable carbohydrates (e.g., lactulose or lactose in gram doses), prokinetics, and laxatives should be stopped at least 24 hours before breath testing (15). Opioids have a well-established effect in delaying intestinal transit, and thus, opioids should be stopped the day before and during the test (8). If any of these medications are unable to be stopped due to patient intolerance or other clinical factors, this should be documented, and the test should be interpreted with some caution (3,15). Antibiotics can significantly alter the hydrogen and methane composition of exhaled breath by reducing the bacterial loads within the gut (20,21). Therefore, it is recommended that antibiotics should be stopped for 4 weeks before the test (15). There is limited evidence regarding the potential interference of probiotics and prebiotics with breath testing results (22,23). Although the North American Consensus guidelines for breath testing do not specify whether these agents should be held, the recent European H2-CH4-breath test group consensus statement recommends holding probiotic use for 24 hours before testing (15). Evidence suggests that proton pump inhibitors (PPIs) and histamine H2-receptor antagonists (H2 blockers) can influence the gut microbiome, but the need to hold these medications before breath testing is controversial (3,15,24,25). Currently, the North American consensus guidelines recommend that PPIs and hydrogen blockers do not need to be held (3). The recent European H2-CH4-breath test group consensus statement recommends that breath testing should be delayed at least 2 weeks after a colonoscopy due to known influences of bowel preps on gut microbial loads and community structure with persistent effects observed 2 weeks later (15,26). Some centers suggest delaying the breath test at least 4 weeks to minimize the influence of the colonoscopy on test results (15,18). Patients with diabetes should have directed instructions on how to adjust their medications before testing.
Lifestyle factors.The combustion of tobacco creates a potent, non-GI tract source of hydrogen gas that directly influences breath testing results (27–29). Increased hydrogen in exhaled breath increases markedly during active smoking. Although these levels do decline after smoking, breath hydrogen levels can remain above typical basal values for at least several hours after smoking (27–29). Thus, patients should be encouraged to refrain from smoking later in the evening before the test and throughout the testing period (3,15). Given that gas exchange rates are proportional to ventilation volumes, physical exercise should not be performed during the breath testing period, as increased ventilation could falsely reduce measured breath hydrogen concentrations via increased diffusion rates (3,15).
Choice of substrate.The North American Consensus guidelines recommend a substrate dose of 75 g glucose (preferred over 50 g) or 10 g lactulose (30). However, European guidelines favor 50 g for glucose or 10–20 g of lactulose (15). The chosen substrate is mixed with or followed by 1 cup of water (3). Some patients may not be able to rapidly ingest the test substrate due to the volume; if this is an issue, potentially smaller volumes or reduced substrate loads (i.e., 50 g glucose rather than 75 g) can be substituted as an alternative approach and recorded. Glucose is regarded as a more specific substrate and more commonly performed (31). Despite the increased sensitivity, some centers continue to prefer using lactulose as their primary substrate for breath testing (32). One way in which lactulose breath tests differ from glucose breath tests is that lactulose breath tests that are positive often have a double peak with an initial peak in the small intestine and then a second peak when lactulose reaches the colon, but this feature may not always be present (1). In the past, lactulose breath tests had also been used to determine transit times, but this approach is not considered reliable and is no longer recommended (1,15). Because lactulose is not directly absorbed by the small intestinal mucosa, lactulose breath testing results are more sensitive to alterations in small intestinal motility patterns than are glucose breath tests. Thus, lactulose may lead to higher false-positive rates than glucose substrates in patients with particularly rapid transit and in diarrheal states. There has been a gradual shift toward using glucose testing as a default substrate to improve the diagnostic accuracy of breath testing for the purposes of diagnosing SIBO (15,31). Yet, lactulose breath tests appear to still have some advantages over glucose substrates. For example, lactulose is a useful alternative substrate in patients with diabetes, as glucose can result in hyperglycemia that secondarily impacts test results (1). Lactulose may also be preferred in patients with slower GI transit who have a higher risk for false-negative test results with glucose testing, although this point remains unproven (33). In addition, lactulose breath testing results may predict response to therapy. In a study of patients with diarrhea-predominant IBS undergoing treatment with rifaximin, patients with a positive baseline lactulose breath test were more likely to have global response to rifaximin therapy, with improvement in abdominal pain and frequency of loose stools (59.7% vs 25.8%) (32).
Breath test administration.After a baseline breath sample is collected, the test substrate (glucose or lactulose) is administered in a single bolus over a brief amount of time. Bacterial contact with the test substrate leads to fermentation and production of hydrogen, methane, and hydrogen sulfide gases. These gases are absorbed into the circulation and released into the alveolar sacs and subsequently exhaled. Exhaled breath samples are collected in regular intervals, generally every 15 or 20 minutes over a period of 180 minutes. Symptoms reported by patients during the study period should be recorded in the study log. This can help correlate symptoms to specific gas levels and provide insight into the patient's symptom pattern. To collect breath samples, patients are advised to breathe normally into an alveolar collection device equipped with a syringe port to withdraw gas samples. Adult patients typically exhale a ∼100 cc volume into the bag, whereas pediatric patients generally exhale ∼50 cc volumes. A 20–30 cc volume of end-expiratory air is immediately collected and submitted for analysis using a gas chromatograph to detect hydrogen, methane, and, if available, carbon dioxide. Gas concentration data are reported in parts per million (ppm). The accuracy of most commercial gas analyzers is generally quite precise. For example, the Model SC (QuinTron Instrument, Milwaukee, WI) has a margin of error of ±3 ppm (17). Breath hydrogen samples are traditionally stable for 6 hours at room temperature, and if measurements are delayed beyond this, storage at −20 °C is needed (34,35). However, different storage approaches can help keep samples stable for longer periods. It is recommended to follow manufacturing recommendations regarding sample transportation and storage (15). Recent research into prolonged storage of samples from at-home testing suggests that methane gas levels may be more affected over longer storage times compared with hydrogen gas levels (36).
Conditions that influence breath test results and how to manage them.Higher levels of hydrogen and/or methane gas measured at baseline (before test substrate administration) suggest ongoing fermentation of carbohydrates. This is generally thought to be most commonly due to poor compliance with the dietary preparations before the test (and thereby measurement of fermentation from the colon), but higher baseline hydrogen levels may reflect other factors such as poor oral hygiene or the presence of foregut dysmotility (3). If high baseline hydrogen levels are observed, the test can be considered indeterminate, or at some centers, the test is aborted and rescheduled for another time (37). Because of these influential factors, it is critical to emphasize dietary prep before testing. The definition of an increased baseline level has not been defined, and interpretation of this point varies among centers. Elevated baseline levels of hydrogen defined with either a cutoff ≥10 or ≥ 20 ppm or methane ≥10 ppm have been reported in approximately a quarter of patients undergoing breath testing (17,38).
Rome guidelines had previously advocated for the use of chlorhexidine mouthwash before substrate administration to diminish fermentation by bacterial flora from the oral cavity (18,39). One method for administering chlorhexidine is to administer 10 mL of chlorhexidine (1.2 mg/mL) mouthwash around the mouth for 20–30 seconds, forcing it between teeth and gargling before spitting it out and rinsing the mouth with water (17). In 1 study of 388 consecutive hydrogen-methane breath tests, chlorhexidine mouthwash significantly reduced hydrogen and methane gas in patients with higher baseline values (defined as ≥ 10 ppm of either hydrogen or methane), reducing breath hydrogen in 67% of patients and/or methane gas in 93% (17). This study highlights the ability of oral dysbiosis/oral hygiene to impact measured gas levels, in some cases to a degree that impacts the interpretation of the test. The study also found that a single mouthwash immediately before breath testing resulted in an apparent early increase in expired gases in the first postsubstrate samples in 30 of 43 (69.7%), suggesting that the first single mouthwash may not be adequate to eliminate the role of oral flora, and mouthwashes before every sample may be more effective (17). However, further studies are needed to determine how frequently and how impactfully oral dysbiosis confounds breath testing in routine clinical practice. The North American consensus and ACG guidelines on breath testing do not specify whether oral antiseptic solutions are necessary, but the recent European guidelines do advocate for oral antiseptic use before testing (1,3,15). A recent study found that light walking for an hour, being careful to avoid hyperventilation, may reduce high baseline hydrogen and methane levels and allow for a meaningful examination while reducing diagnostic delays from rescheduling the test, but more research is needed to support this approach (38,40).
Increased baseline hydrogen levels could potentially also reflect the presence of significant foregut dysmotility, such as in patients with severe esophageal dysmotility (i.e., achalasia) or significantly impaired gastric motility (i.e., gastroparesis) (41). The concern with these conditions is that the ingested substrate will be metabolized by bacteria residing in the mouth, esophagus, or stomach and may not reliably reach the small intestine within the time windows typically used for interpreting breath test data. These conditions should be considered when determining whether the patient would be best served with adapted testing protocols (i.e., assessment of the orocecal transit time [OCTT]) or an alternative testing approach (i.e., small bowel aspirates).
Test results and interpretation.Hydrogen-methane breath tests are generally easy to record and straightforward to interpret. Hydrogen and methane gas levels recorded from samples collected over time are presented in a report and plotted graphically (sample test in Figure 1a,b). Figure 2 demonstrates various commonly observed patterns of glucose breath test results and their interpretation. There is consensus among all current guidelines to define a hydrogen gas rise of ≥20 ppm from baseline by 90 minutes as a positive test result for SIBO in both clinical and research settings (1,3). A methane gas rise ≥10 ppm at any time during the study period is also defined as positive breath test (1,3). Former protocols used different substrate dosages and cutoff levels. For example, the modified Rome protocol used a 50 g glucose load and a >12 ppm hydrogen and methane cutoff (18). Comparison of the North American and modified Rome protocols (North American 3,102 patients; modified Rome 3,193 patients) found that positive glucose breath tests were more common with the North American protocol (39.5% vs 29.7%, P < 0.001) (30). This result appeared to be due to generally higher peak methane levels with the North American protocol (P < 0.001) (30). Average times to achieve peak hydrogen and methane production levels were not found to differ between protocols. In addition, GI and extraintestinal symptoms during breath testing were more prevalent with the North American protocol (30). As such, there is a higher test positivity rate with the North American Consensus protocol.
 Figure 1.:
Figure 1.: (a and b) Sample glucose breath test reports generally consist of a table (a) with individual breath test values and plot of the data (b). The test is generally measured in 10–30-minute intervals and commonly performed in 2–3 hours. Breath test values at 90 minutes are used for interpretation (highlighted box), but all numbers are provided given variable individual factors that can influence values (i.e., orocecal time). Test interpretation uses the values of the first 90-minute results: peak hydrogen production: normal <20 ppm, increased methane production at any time: normal <10 ppm, f(CO2) closer to 1.00 is ideal. Because the corrected gas levels do not alter the interpretation, observed hydrogen and methane are plotted in Figure 1b. ppm, parts per million.
 Figure 2.:
Figure 2.: Possible patterns of glucose breath test results and their interpretation. x axis is time (minutes), y axis is gas (ppm), solid line is hydrogen values, and the dashed line represents methane values. (a–c) Small intestinal bacterial overgrowth (SIBO) supported: A. high hydrogen, no methane; (b) no hydrogen, high methane; (c) high hydrogen, high methane. (d–f) SIBO not supported: (d) low hydrogen, low methane; (e) no hydrogen, no methane (flat line); (f) high hydrogen baseline—consider retesting. ppm, parts per million.
Hydrogen.The patterns of hydrogen peaks in positive tests will vary based on the substrate given. In positive glucose breath tests, there is a peak in hydrogen production when the substrate enters the jejunum. In positive lactulose breath tests, there is generally a double peak, with the second peak occurring when the lactulose enters the colon (1). Lactulose breath tests have been previously considered a method to determine OCTT; however, for a variety of factors, this is not considered a completely reliable approach (1). As such, there is no current role in using lactulose to measure OCTT, and the presence of 2 separate peaks on lactulose breath testing is not required for a diagnosis of SIBO (1).
Methane.There is increasing recognition that methane gas production directly impacts GI function. Recent ACG guidelines proposed a new term to describe levels of increased methane gas production—intestinal methanogen overgrowth (IMO) (1). Distinguishing IMO from SIBO acknowledges that a different clinical phenotype is associated with higher levels of methane production (constipation) than hydrogen production (typically diarrhea). The IMO terminology also more accurately reflects the fact that methanogens are not actually bacteria but belong to the Archaea kingdom (1). Furthermore, methanogens may overpopulate either the colon or the small intestine (1). Finally, methanogens may not be adequately treated by single antibiotic treatments used in SIBO management and may require unique antibiotic treatment combinations (i.e., rifaximin and neomycin) (42). A level of methane gas level ≥10 ppm observed at any time during the breath testing (including at baseline in a fasting patient) is considered a positive IMO test result (43).
Multiple studies have identified that higher methane levels are positively associated with constipation and are inversely associated with diarrheal disorders (44,45) Methane gas has been shown to directly inhibit intestinal transit in dogs by 59% compared with insufflated room air (46), and methane levels correlate with the slower intestinal transit times (2,46–49). Methane-predominant SIBO/IMO is more prevalent in patients with constipation-predominant IBS (47–50). It is possible that future testing protocols may be modified if the intent of the breath test is to diagnose IMO. For example, lactulose has advantages over glucose substrates to determine IMO, given that lactulose accesses more distal regions of the GI tract and archaea overgrowth may occur in either the small intestine or the colon (1). Different testing protocols specifically for IMO could be considered in the future. A recent study evaluating a fasting single methane measurement (SMM) ≥10 ppm compared against standardized 2-hour breath tests demonstrated high test performance (compared with 2-hour glucose breath test: sensitivity 86.4%, specificity 100%, positive predictive value 100%, and negative predictive value 97.0%; compared with 2-hour lactulose breath test: sensitivity 86.4%, specificity 100%, positive predictive value 100%, and negative predictive value 97.6%) (43). The study also demonstrated that the SMM value is associated with constipation, is associated with Methanobrevibacter smithii colonization (a known intestinal methanogen), and that SMM decreases after antibiotics (43). In addition, studies assessing patients with a positive breath test for IMO have found that over 75% of patients had CH4 ≥ 10 ppm at baseline (51,52). As such, SMM testing could prove a useful surrogate for assessing treatment response. Future research studies are needed to identify additional clinical characteristics of patients with IMO and whether protocol adaptations may be helpful to detect patients with IMO.
Carbon dioxide.If available, measurement of CO2 concentration (%) is used to derive a correction factor, f(CO2), that accounts for dilution of the alveolar sample by ambient air or dead space, thereby allowing for correction of observed gas levels and also identifying significant sampling errors (3,15). To correct the sample concentrations of hydrogen and methane for possible dilution because of incorrect gas sampling, the observed H2 and CH4 values are multiplied by the correction factor calculated from f(CO2) = alveolar CO2 concentration/sample CO2 concentration, yielding normalized H2 and CH4 values (13). At our center, we assume an alveolar CO2 concentration of 5.5%, but some centers use 5% (13,36,37,53). Correction factor values close to 1.00 indicate excellent sample collection with minimal to no dilution, whereas high values indicate poor sample collection. Guidelines discuss the measurement of CO2 but do not formally discuss how it should be implemented in test interpretation (3). Our approach is to consider samples valid when CO2 correction factor ≤ 2.5, similar to the published literature (36). Regardless, carbon dioxide corrections generally only impact test interpretation for a minority of patients. One study that evaluated differences in results after correction found high agreement of positive breath test results with and without CO2 correction (Cohen kappa 0.92) (13).
Test performance characteristicsSeveral characteristics are used to evaluate the utility of a diagnostic test in discriminating the presence or absence of a disease. These test characteristics are sensitivity, specificity, positive predictive value, negative predictive value, likelihood ratios, and DOR (Figure 3). Here, sensitivity is defined as the ability of a positive breath test to accurately predict the presence of SIBO, expressed as the percentage of persons with SIBO who test positive. Specificity is defined as the ability of a negative breath test to accurately predict the absence of SIBO, expressed as the percentage of persons without SIBO who test negative. Positive predictive value is the ability of breath tests to separate true-positive results from false-positive results in a given population, expressed as the percentage of persons with a positive breath test who indeed have SIBO. Negative predictive value is the ability of breath tests to separate true-negative results from false-negative results in a given population, expressed as the percentage of persons with a negative test result who do not have SIBO. Finally, likelihood ratios are perhaps the most useful tool for clinical management and decision making. Positive likelihood ratios (PLRs) are defined as the probability of a positive breath test in a patient with SIBO, divided by the probability of a positive breath test in a person without SIBO. Negative likelihood ratios (NLRs) are defined as the probability of a negative breath test in a patient with SIBO, divided by the probability of a negative test in a person without SIBO. Likelihood ratios are always a positive number (ranging from zero to infinity). Likelihood ratios greater than 1 argue for the diagnosis of interest, and the larger the number, the greater the posttest odds that the patient truly has the SIBO. Findings between 0 and 1 argue against the diagnosis of interest. Values close to 0 indicate that SIBO is less likely and values close to 1 are equivocal. The DOR is a measure of the effectiveness of a diagnostic test. Here, it is defined as the ratio of the odds of the breath test being positive if the subject has SIBO, relative to the odds of the breath test being positive if the subject does not have SIBO. DORs for useful tests are greater than 1, with greater DORs indicating better test performance (e.g., a DOR of close to 10 indicates a very good test). Finally, the area under the curve (AUC) of receiver operator curves plots sensitivity and specificity, where 1 − specificity is on the x axis, and sensitivity is on the y axis. The AUC helps estimate the discriminative power of a test, where 1 indicates a perfect test, and lower values suggest a less discriminating test (i.e., a completely nondiscriminating test has an AUC of 0.5) (Table 3).
 Figure 3.:
Figure 3.: Diagnostic test parameters and formulas. SIBO, small intestinal bacterial overgrowth; ppm, parts per million.
Table 3. - Test characteristics of glucose and lactulose breath tests based on published data using jejunal aspirates as the gold standard (54)
留言 (0)