
記住我









Patient-reported outcomes (PROs) are necessary to evaluate outcomes following anterior cruciate ligament reconstruction (ACL-R).
The minimal important change (MIC) for different PROs has recently received increased interest in orthopaedic research and has been subsequently used to evaluate effects of patient characteristics on post-operative outcomes.
Although improvements in the Knee injury and Osteoarthritis Outcome Score subscale scores have been associated with ACL-R, there are still patients who do not achieve the MIC after ACL-R.
WHAT THIS STUDY ADDSThe increased understanding of the patients who do not benefit from the surgical treatment have a high clinical relevance and subsequently, can help tailor treatment for individual patients.
Achievement of the MIC after ACL-R may be multifactorial and therefore the identified possible risk factors should be considered in a treatment plan to establish realistic expectations for the patient.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYClinicians should be aware of both modifiable and non-modifiable risk factors for not achieving an MIC after ACL-R and thus, should adjust the treatment approach and establish realistic expectations for the patient.
The MIC values may be different for patients with different baseline PRO scores requiring further research.
IntroductionInjury to the anterior cruciate ligament (ACL) is one of the most common severe injuries in the knee leading to decreased knee function, activity level and quality of life (QoL).1 2 Currently, ACL injuries can be treated with either rehabilitation alone or combined with surgical reconstruction ACL (ACL-R), where the surgical treatment is reported to improve the likelihood of returning to more knee-strenuous sports (RTS).3 4 During the past decades, there has been an increasing interest in using patient-reported outcomes (PROs), such as the Knee injury and Osteoarthritis Outcome Score (KOOS), to evaluate outcomes related to different treatment options for patients with ACL injuries.4 5 In addition, different patient characteristics (sports participation, age), injury characteristics (concomitant injuries) as well as surgical factors (graft diameter, graft fixation, time from injury to surgery) have been demonstrated to affect post-operative outcomes,6–12 and subsequently, contribute to variation in outcomes following ACL-R. A growing interest has recently developed in estimating the minimal important change (MIC), defined as the smallest change in outcome that a patient perceives as important,6 for different PROs. The MICs have been used to identify the effects of demographic and surgical factors on post-operative outcomes for individuals undergoing ACL-R to evaluate.6 13
While a large part of previous studies investigating improvement in knee function following ACL-R primarily focus on evaluating changes in PRO scores, less is known about the patients not achieving an MIC for specific combined KOOS subscales.4 14 15 An increased understanding of the patients who do not benefit from ACL-R can have a high clinical relevance and help tailor treatment for individual patients. Therefore, the purpose of this study was to determine patient and surgical risk factors for not achieving the MIC in both the KOOS Function in Sport and Recreation (Sport/Rec), and Knee-Related QoL subscales 1 year after ACL-R.
MethodsThe study is presented according to the Strengthening the Reporting of Observational studies in Epidemiology guidelines.16
This registry study was based on data obtained from the Swedish National Knee Ligament Registry (SNKLR). The purpose of the SNKLR is to collect data on patients undergoing treatment for ACL injury and uses a web-based protocol for data registration consisting of patient-reported and surgeon-reported sections.17 Surgeons report on patient demographic characteristics, injury-related and surgery-related factors, while patients answer questionnaires regarding knee function, including the KOOS Sport/Rec and QoL subscales. The SNKLR has previously been described in detail.18
Study populationData on patients >15 years of age at time of primary ACL-R with pre-operative and 1-year post-operative KOOS data in the SNKLR between 1 January 2006 and 30 October 2019 were extracted for this study. The study population was divided into two groups: (1) those that did not achieve the MIC for the KOOS Sport/Rec and QoL subscales and (2) those that achieved the MIC for both or only one of the subscales 1 year after ACL-R.
Patients with any prior knee surgery, concomitant fracture, nerve, or vascular injury, concomitant posterior cruciate ligament (PCL) injury or surgically treated medial collateral ligament (MCL) or lateral collateral ligament injuries were excluded. Patients treated with double bundle ACL-R or revision ACL-R were also excluded from the analysis. Furthermore, patients with either high preoperative KOOS Sport/Rec (>87.9) or QoL (>81.7) scores were excluded since the achievement of the MIC could not be observed in these patients.19
Data regarding patient demographics (sex, age, body mass index (BMI), smoking status), injury characteristics (activity at time of injury, concomitant injury) and surgical factors (time from injury to surgery, graft type) were also retrieved from the SNKLR. The KOOS Sport/Rec and QoL subscale scores before surgery and at 1-year follow-up were also extracted from the SNKLR. Activities at the time of injury were further divided into sports-related (alpine/skiing, pivoting sport, non-pivoting sport, other physical activity) and non-sports-related activities (other, traffic-related activities).
Outcome measuresThe KOOS consists of 5 subscales including Pain, Other Symptoms, Sport/Rec, QoL and Activities of Daily Living, each of which are scaled from 0 to 100, where a higher score indicates a better outcome.20 The KOOS has been previously validated and specifically described to be a reliable assessment tool to measure function and QoL in patients undergoing ACL-R,19 21 with intraclass correlation coefficients reported to be 0.75 and 0.89 for KOOS Sport/Rec and QoL, respectively.21 The threshold scores for achievement of the MIC have been previously calculated using an anchor-based approach that made use of a 7-point global rating of change question as the external anchor for an important change and use of predictive modelling methods and receiver operating characteristic (ROC) curve analyses. The MICs were found to be 12.1 and 18.3 for Sport/Rec and QoL, respectively.19
The main outcomes of interest for this study were the KOOS Sport/Rec and QoL subscale scores, which were dichotomised into those not achieving versus achieving the MIC for each subscale. Subsequently, achievement of the MIC for each subscale was combined into a single variable that represented failure to achieve the MIC for both the Sport/Rec and QoL subscales (MIC KOOS Sport & QoL). Thus, the primary outcome for this study was the MIC KOOS Sport & QoL that consisted of patients who failed to achieve the MIC on both the KOOS Sport/Rec and QoL subscales versus those that achieved the MIC in either one or both of the KOOS subscales.19
Equity, diversity and inclusionThis study included both female and male patients undergoing ACL-R. Our multidisciplinary research team involved both female and male researchers from different medical areas (orthopaedics and physiotherapy) and age categories (junior researchers, professors). Data were collected from the SNKLR and thereby, data collection did not differ between the included patients. All patients undergoing ACL-R, including different ethnicities, culture, socioeconomic level, sex and gender are included in the SNKLR.
Statistical analysesThe statistical analyses were performed with the SAS System for Windows (V.9, SAS Institute). Continuous and ordinal data were presented by using the mean and SD as well as median with minimum and maximum. Count (n) and proportion (%) were used to summarise dichotomous variables. In addition, univariable and stepwise multivariable logistic regression analyses were used to determine demographic and surgical factors associated with not achieving the MIC for both the Sport/Rec and QoL subscales and presented as OR, p value and 95% CI. Variables included in the stepwise multivariable logistic regression analyses were age at time of surgery, sex, meniscal and cartilage injury as well as ACL graft type and pre-operative KOOS Sport/Rec and QoL scores. The OR for patient age and pre-operative KOOS scores, calculated in the univariable and stepwise multivariable logistic regression analysis, were based on a 10-year and 10-point increase, respectively. Furthermore, the area under the curve (AUC) with 95% CI was used to present the results from the univariable analyses. The AUC varies between 0.5 and 1, where a greater AUC represents better predictive capacity. Further, the AUC between 0.5 and 0.7 indicates poor predictive capacity, while the AUC between 0.7 and 0.9 or between 0.9 and 1.00 represents acceptable/good and excellent predictive capacity, respectively. All significance tests were two sided and conducted at the 5% significance level.
Supplemental analysesSupplemental analyses were performed separately to identify factors associated with not achieving the MIC for either the KOOS Sport/Rec or QoL subscales. Univariable and stepwise multivariable logistic regression analyses were performed to determine demographic and surgical factors associated with not achieving the MIC for the KOOS Sport/Rec or QoL subscales 1 year after ACL-R. Variables included in these stepwise multivariable logistic regression analyses were the same predictor variables that were included in the primary analysis
ResultsBaseline characteristicsOf the 16 131 patients included in the study, 8274 were males (51%) and the mean age at time of surgery was 29 years±11. The median time from injury to surgery was 7.9 (0–551) months. A hamstring tendon autograft was found to be the most commonly used autograft (93%), while patellar tendon autograft was used in 4.8% of the cases. Additionally, concomitant injuries were found to be common among the patients (57%), where 27% and 44% of the patients had concomitant cartilage and meniscus injuries, respectively (table 1). Most of the ACL injuries were the result of a pivoting sport activity (64%) (table 2). The average scores for the pre-operative Sport/Rec and QoL subscales for the KOOS were found to be 37±25 and 32±17, respectively. Post-operatively, the average scores for the KOOS Sport/Rec and QoL subscales were 64±27 and 58±23, respectively (table 3).
Table 1Baseline characteristics of patients
Table 2Activities at time of injury for patients undergoing ACL-R
Table 3Pre-operative and post-operative KOOS
Minimal important changeIn total, 7109 (44%) of patients included in the study did not achieve the MIC for both the Sport/Rec and QoL scales 1 year after ACL-R. Results from univariable logistic regression are presented in the figure 1. From the multivariable stepwise logistic regression, older patients (OR 0.91, 95% CI 0.88 to 0.94; p<0.0001), males (OR 0.93, 95% CI 0.87 to 0.99; p=0.034) and patients undergoing ACL-R with hamstring tendon autograft (OR 0.70, 95% CI 0.60 to 0.81; p<0.0001) had lower odds of not achieving the MIC for both the Sport/Rec and QoL subscales compared with younger patients, females and patients undergoing ACL-R with a patellar tendon autograft. Furthermore, patients with concomitant cartilage injuries (OR 1.17, 95% CI 1.09 to 1.27; p<0.0001) had higher odds for not achieving the MIC for both the Sport/Rec and QoL subscales 1 year after ACL-R compared with patients without concomitant cartilage injuries. In addition, patients with higher pre-operative KOOS Sport/Rec and QoL scores had higher odds for not achieving the MIC for both the Sports/Rec and QoL subscales 1 year after ACL-R (OR 1.34, 95% CI 1.31 to 1.36; p<0.0001) (figure 2). Neither activity at time of injury (OR 0.95, 95% CI 0.87 to 1.04; p=0.30) nor BMI (OR 1.00, 95% CI 0.99 to 1.01; p=0.90) were found to be associated with not achieving the MIC for both the Sport/Rec and QoL subscales 1 year after ACL-R (table 4). The predictive capacity of the multivariable model was relatively poor as the AUC was 0.65 (95% CI 0.64 to 0.66).
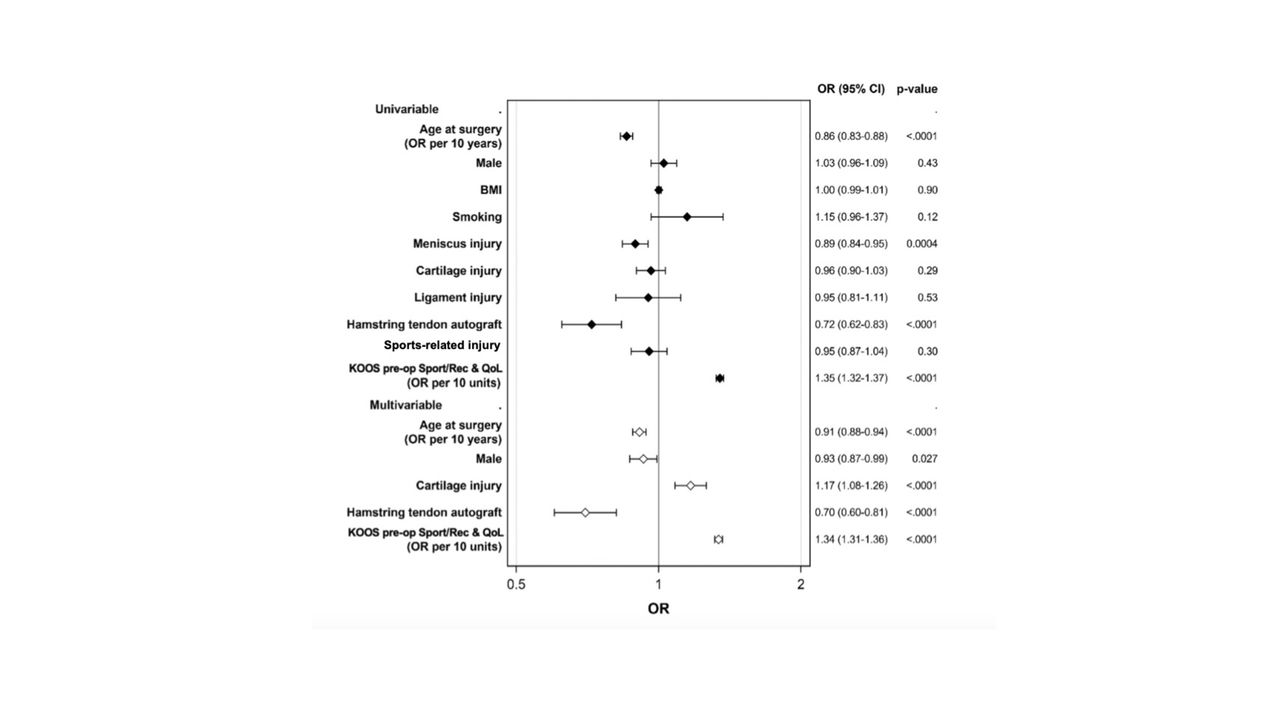 Figure 1
Figure 1 Forest plot illustrating the OR and 95% CI for predicting not achieving MIC for Combined Sport/Rec and QoL KOOS subscales 1 year after ACL reconstruction. OR>1 = not achieving MIC; OR<1 = achieving MIC. ACL, anterior cruciate ligament; BMI, body mass index; KOOS, Knee Injury and Osteoarthritis Score; MIC, minimal important change; Pre-op, pre-operative; QoL, quality of life; Sport/Rec, function in sport and recreation.
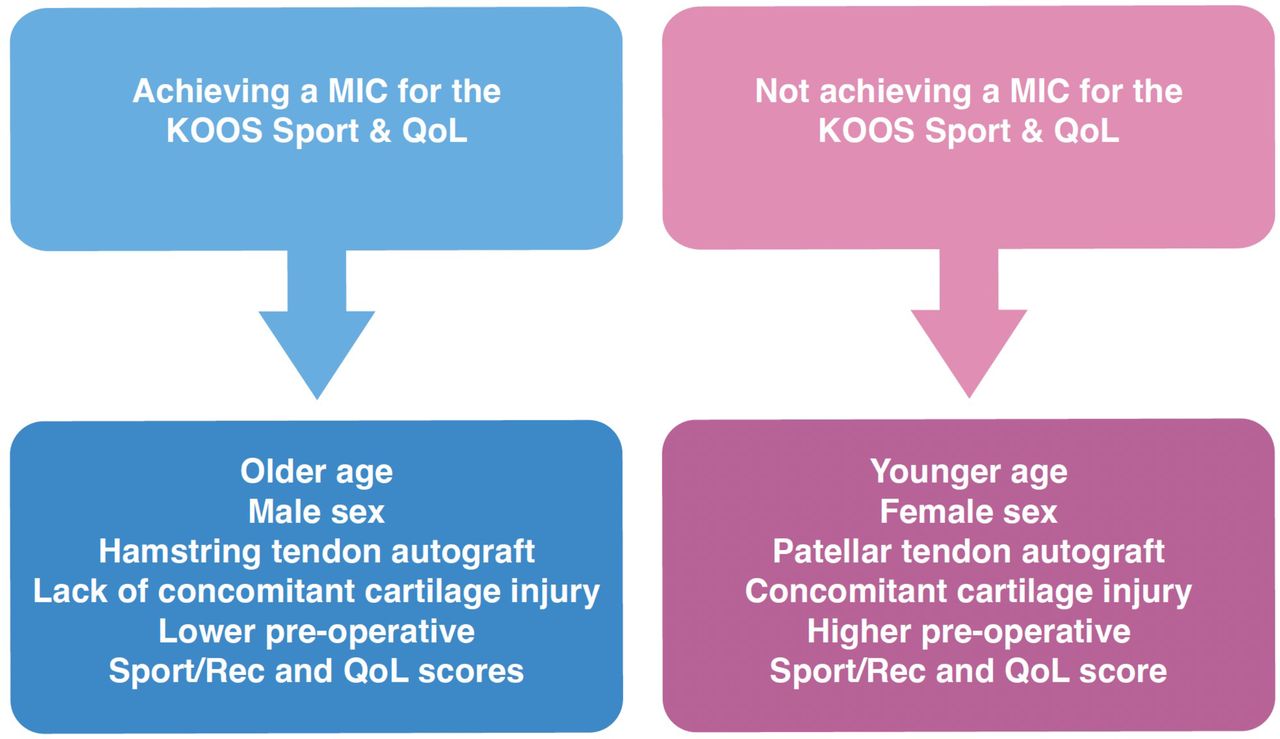 Figure 2
Figure 2 Diagrammatic overview of the factors associated with achieving and not achieving MIC for Combined Sport/Rec and QoL KOOS subscales (KOOS Sport/QoL) 1 year after ACL reconstruction. ACL, anterior cruciate ligament; KOOS, Knee Injury and Osteoarthritis Score; MIC, minimal important change; QoL, quality of life; Sport/Rec, function in sport and recreation; Sport/QoL, combined Sport/Rec and QoL KOOS subscales.
Table 4Results from univariable and multivariable logistics regression analysis. Prediction for not achieving the MIC for Combined Sport/Rec and QoL KOOS Scores.
Supplemental analysesIn total, 4959 (31%) and 5490 (34%) of included patients did not achieve the MIC for the KOOS Sport/Rec and QoL, respectively. Results from the supplemental univariable and multivariable stepwise logistic regression models were comparable with the results from the univariable and multivariable analyses for the combined KOOS Sport/Rec and QoL scales. Demographic and surgical factors associated with not achieving MIC for the KOOS Sport/Rec or QoL subscales 1 year after ACL-R are presented in online supplemental material tables 5–7.
DiscussionThis large, registry-based study identified several factors associated with the risk for not achieving the MIC for both the Sport/Rec and QoL subscales 1 year after ACL-R. Both modifiable and non-modifiable factors were found to be associated with not achieving the MIC for both the Sport/Rec and QoL KOOS subscales 1 year after ACL-R. Approximately 44% of the patients included in this analysis did not achieve a change in both the Sport/Rec and QoL KOOS subscales larger than the MIC 1 year after ACL-R, suggesting that they failed to perceive an important change in both Sport/Rec and QoL.
The results of this study demonstrate that older individuals at the time of ACL-R, males and patients undergoing reconstruction with a hamstring tendon autograft had lower odds of not achieving the MIC for both the Sport/Rec and QoL KOOS subscales 1 year after ACL-R. Furthermore, patients with concomitant injuries to the cartilage and patients with higher pre-operative KOOS Sport/Rec and QoL scores had higher odds of not achieving the MIC for both the Sport/Rec and QoL KOOS subscales 1 year after ACL-R. As such, our results suggest that the association between injury-related, surgical-related and patient-related factors and not achieving the MIC for the Sport/Rec and knee-related QoL is multifactorial.
There are several factors that might contribute to our results suggesting lower odds for not achieving the MIC in older patients, where, for instance, older individuals tend to be less physically active and this group of patients usually includes a smaller proportion of athletes compared with a younger population.22 The lower odds of not achieving the MIC for both the Sport/Rec and QoL subscales 1 year after ACL-R in older population, may be explained by the difference in expected knee function following ACL-R, where older individuals might have lower expectations on future knee function compared with younger individuals.23
In agreement with previous research, males were found to have better outcomes following ACL-R.24–26 This was supported by our results that found that males had lower odds of not achieving the MIC for both the Sport/Rec and QoL KOOS subscales 1 year after ACL-R. This association between male sex and better post-operative outcomes following ACL-R may be explained by the different rehabilitation strategies and psychosocial barriers related to self-efficacy compared with females, where males have been reported to maintain a more positive mindset compared with females.26 27 Thus, the eventual discrepancy in post-operative care between females and males migh have had an impact on the post-operative outcomes 1 year after ACL-R. This discrepancy in outcomes followed by an ACL injury between males and females has previously been discussed to be potentially influenced by ‘gender environment’ of ACL rehabilitation, where gender has been explained to function as an extrinsic determinant over the course of treatment for ACL injury.26 Furthermore, self-efficacy has previously been identified as an important predictor of the KOOS Sport/Rec and QoL scores at 1 year follow up28 and subsequently, could partly explain our study results reporting better post-operative outcomes in males.
This study also found that patients undergoing ACL-R with hamstring tendon autograft had lower odds for not achieving the MIC for both the Sport/Rec and QoL KOOS subscales compared with patients undergoing patellar tendon autograft ACL-R. Less post-operative kneeling pain has been previously reported in the patients undergoing ACL-R with hamstring tendon autograft compared with patients undergoing patellar tendon autograft ACL-R29–31 and thus, could partly explain the differences found in early post-operative outcomes. In addition, a relatively small proportion of patients in our cohort underwent ACL-R using patellar tendon autograft, which could have affected the study results since a small sample size may lead to overestimates of the effect size. Consequently, these findings should be interpreted with caution since use of hamstring tendon and patellar tendon autografts for ACL-R might result in similar short-term and long-term outcomes.
Poorer outcomes have previously been reported following ACL-R with concomitant cartilage injuries,11 12 32 33 and may partly be explained by the more advanced surgical procedures required followed by eventually more restricted post-operative rehabilitation for patients with concomitant cartilage injuries compared those without a cartilage injury.34 In addition, a higher degree of persistent symptoms and pain after ACL-R have been previously reported in patients with concomitant cartilage injuries compared with patients without cartilage injuries,35 which may result in reduced activity and decreased QoL.
Adding to previous studies, this study found that patients with higher pre-operative KOOS Sport/Rec and QoL scores had higher odds of not achieving an MIC for both the Sport/Rec and QoL subscales 1 year after ACL-R compared with patients with lower pre-operative KOOS Sport/Rec and QoL scores. Higher pre-operative PROs have previously been associated with an increased likelihood of better outcome scores after ACL-R.36 37 The higher odds of not achieving the MIC 1 year after ACL-R in patients with higher pre-operative KOOS may be explained by the fact that these patients experience less improvement in KOOS Sports/Rec and QoL scores,37 because pre-operatively they already had good/better knee function and QoL. In addition, patients with lower pre-operative KOOS Sport/Rec and QoL scores in our cohort appeared to benefit more, in terms of improvement in KOOS from undergoing ACL-R compared with patients with higher pre-operative KOOS Sport/Rec and QoL scores. Furthermore, patients with higher pre-operative scores have less room for improvement and achievement of the MIC and as such, the MIC value, which was determined on all patients, may not be an appropriate MIC for patients that have higher pre-operative scores. Hence, it may be necessary to have different MIC values based on the patients baseline PRO score.
The modifiable (graft choice, concomitant cartilage injuries, preoperative KOOS scores) and non-modifiable risk factors (age, patient sex) for not achieving the MIC found in this study should be considered prior to surgery. Importantly, the results suggest that younger patients, females and patients with higher pre-operative KOOS Sport/Rec and QoL scores may benefit less from the surgical treatment compared with older patients, males and patients with lower pre-operative KOOS Sport/Rec and QoL scores. Additionally, the findings of this study suggest that treatment of concomitant cartilage injuries may be necessary to increase the likelihood of achieving a clinically important benefit from surgery. Achievement of the MIC after ACL-R may be multifactorial, and therefore, the identified possible risk factors for the failure to achieve the MIC should be considered in a treatment plan to establish realistic expectations for the patient.
This study had several strengths and limitations. One of the main strengths of this study was the large sample size including both baseline and follow-up data on 16 131 patients undergoing ACL-R. In addition, the SNKLR has previously been reported to cover more than 90% of all ACL-Rs performed in Sweden35 and, therefore, has good generalisability to the Swedish population undergoing ACL-R. One limitation of this study was the relatively poor predictive capacity of the multivariable models leading to some potential limitations when interpretating the study findings. Other variables need to be explored to better understand which patients who do not benefit from ACL-R. However, the multivariable models of this study can help to correctly estimate which individuals will fail to achieve the MIC for both the Sport/Rec and QoL subscales 1 year after ACL-R in approximately 64% of cases in expectation of that the variables included in this current multivariable model are known. Additionally, data in regard to treatment of concomitant injuries was not obtained from the registry and thus, could not be analysed. The response rate for the KOOS at 1-year follow-up has also been relatively low in the SNKLR, varying between 58% and 76%.38 Finally, the MIC values, used in this study, might have not identified all the patients achieving the MIC after ACL-R since the MIC may vary based on the magnitude of the baseline Sport/Rec and QoL scores.
ConclusionOlder patients, males and patients treated with hamstring tendon autograft ACL-R had lower odds of not achieving the MIC for both the Sport/Rec and QoL KOOS subscales 1 year after ACL-R. In addition, patients with concomitant cartilage injuries and higher pre-operative KOOS Sport/Rec and QoL scores had higher odds for not achieving the MIC 1 year after ACL-R. Our study results suggest that younger patients, females and patients with concomitant cartilage injuries and higher pre-operative KOOS Sport/Rec and QoL scores are less likely to benefit from ACL-R, and subsequently, have a lower probability of improved knee function after ACL-R. Furthermore, graft choice may also affect the risk of not achieving the MIC. However, results should be interpreted with caution as the predictive capacity of the multivariable models was relatively poor and thus, validation on a second independent sample is needed before the results can be applied clinically.
Data availability statementData are available on reasonable request.
Ethics statementsPatient consent for publicationEthics approvalThis study was approved by the Regional Ethical Board in Stockholm, Sweden (2011/337-31/3), and the Swedish Ethical Review Authority (2022-00913-01), and was performed in accordance with the Declaration of Helsinki.
AcknowledgmentsThe authors would like to thank statisticians Bengt Bengtsson and Nils-Gunnar Pehrsson from the Statistiska Konsultgruppen for help with performing the statistical analyses and giving advice regarding interpretation of the data.
留言 (0)