
記住我
The treatment of HCC is challenging due to two main reasons. Firstly, HCC has a high recurrence rate despite improved treatment methods. Secondly, many cases of HCC quickly develop resistance to treatment; thus, combined therapy is often required, increasing the treatment burden on the patient. Despite these challenges, extensive research is underway to improve current treatment modalities and introduce new treatment options to overcome these obstacles [24].
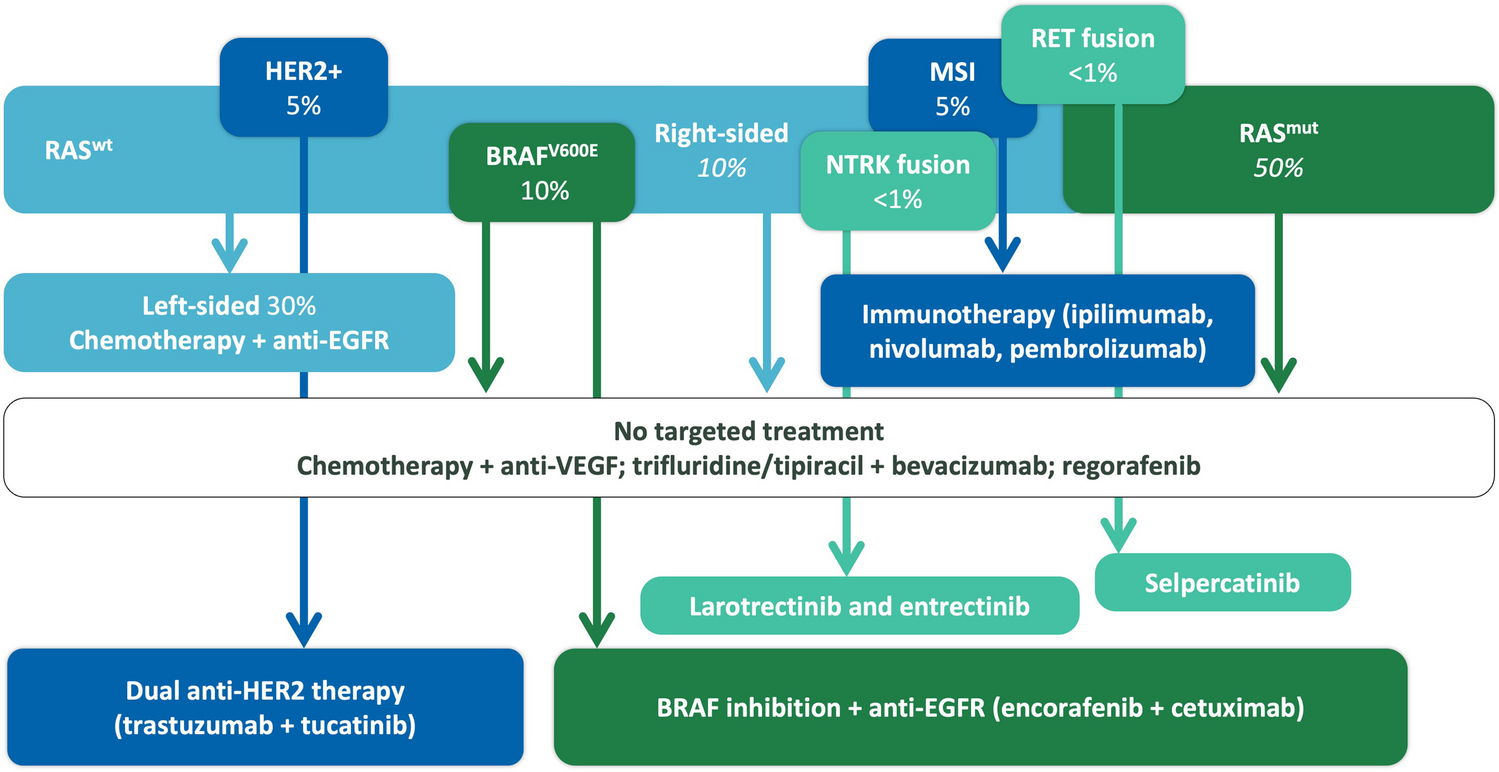
Many guidelines have been established to aid the medical team in determining the most suitable treatment option for the patient. These guidelines consider liver staging, state of liver function, and overall clinical presentation of the patient. Such guidelines include those published by the American Association for the Study of Liver Disease (AASLD) and the European Society for Medical Oncology (ESMO). Figure 1 provides a summary of the main types of treatment implemented in the management of HCC and Table 1 provides an overview of ongoing clinical trials for the management of HCC.
Fig. 1
Overview of the main types of treatment implemented in the management of HCC
Table 1 Overview of ongoing clinical trials for the management of hepatocellular carcinoma (HCC)Surgical strategiesSurgical treatments are usually designated for patients in the early stages of liver cancer, and these treatments tend to be curative. Hepatic resection is the recommended treatment option for patients with good liver function, small masses, and no vascular invasion. Furthermore, liver transplantation is the ideal curative treatment in many early cases of liver cancer, as it removes the tumor and prevents any future cirrhosis. However, due to the few donors, liver transplantation is not always feasible, and other treatment options have to be considered [25]. Patients who present with intermediate-stage liver cancer may be candidates for transarterial chemoembolization (TACE). This method involves inserting a chemotherapeutic agent such as cisplatin mixed with iodized oil into the tumor, followed by embolization of tumor arteries using an embolizing agent. The combined effect of the chemotherapeutic agent and ischemia leads to significant damage to tumor tissue [26].
ChemotherapyHCC is considered a drug-resistant tumor, and most chemotherapeutic agents have shown to be largely ineffective in its treatment. This remained the case until 2007 when the FDA approved sorafenib as a chemotherapeutic agent for HCC. Since then, sorafenib has been recommended as the first-line treatment for advanced stages of HCC. The initial clinical trial involving sorafenib showed an increase of 3 to 5 months in survival time compared to a placebo group. This outcome is far below the established therapeutic goal; however, it paved the way for future developments [27].
Sorafenib is a multi-kinase inhibitor that exerts a powerful anti-tumor and anti-angiogenic effect by blocking cell signaling pathways such as Raf, MEK, and ERK that promote cellular proliferation. In addition, it blocks the vascular endothelial growth factor receptor (VEGFR) and the platelet-derived growth factor receptor (PDGFR), inhibiting angiogenesis, which disrupts tumor cell growth. Despite its wide use, sorafenib has various adverse effects, such as skin rash, diarrhea, increased blood pressure, and redness of soles or palms [28••]. HCC cells that do not use the pathways mentioned above for their proliferation develop resistance to sorafenib, and it has been shown that HCC patients that are on long-term administration of sorafenib develop resistance as well [24].
Several drugs are currently in clinical trials in an attempt to be used as second-line or sequential therapy in patients that are being treated with first-line agents such as sorafenib and develop resistance. These drugs would be given in an attempt to overcome drug resistance that usually develops during the treatment course. One such drug is regorafenib, a multi-kinase inhibitor. The RESORCE trial (NCT01774344) is a randomized, double-blind, placebo-controlled, and phase III clinical trial that was completed in 2019. The study showed regorafenib as an effective second-line therapy in patients that were on sorafenib treatment. Regorafenib provided a significant survival benefit to patients on sorafenib treatment compared to placebo [29•].
Several other chemotherapeutic drugs have been developed recently and are undergoing extensive clinical trials. One drug that has shown potential is lenvatinib. This drug exhibits anti-tumor activity in multiple ways. Firstly, lenvatinib inhibits the vascular endothelial growth factor (VEGF)/vascular endothelial growth factor receptor (VEGFR) pathway, which is responsible for tumor angiogenesis, a process that is essential for tumor growth and metastasis. This is achieved by the binding of lenvatinib on the VEGFR found on tumor cells, thereby preventing the binding of VEGF to its receptor. Secondly, the fibroblast growth factor (FGF)/fibroblast growth factor receptor (FGFR) pathway is abnormally activated in HCC. Tumor cells secrete a large amount of FGF and express an aberrantly high number of FGFR on their outer membranes. The binding of FGF to FGFR activates multiple different signaling pathways, such as RAS/MAPK and PI3K/AKT pathways that play a role in tumor growth and progression. Lenvatinib binds to and blocks FGFR, inhibiting this aberrant pathway. Finally, the RET signaling pathway is responsible for abnormal cell proliferation seen in HCC. This pathway involves the autophosphorylation of tyrosine kinase residues after ligand binding. Lenvatinib blocks the autophosphorylation of the various tyrosine kinase receptors found on tumor cells thereby directly inhibiting cell proliferation [30••].
The REFLECT clinical trial (NCT01761266) compared the clinical outcomes of lenvatinib with those of sorafenib and revealed that lenvatinib had a slightly higher overall survival than sorafenib. Specifically, lenvatinib had an overall survival of 13.6 months, while sorafenib had an overall survival of 12.2 months. In addition, lenvatinib had a significantly higher progression-free survival than sorafenib, with 7.4 months and 3.7 months, respectively. The results of the REFLECT clinical trial are considered the first breakthrough in the chemotherapy treatment of liver cancer since 2007. Lenvatinib is the first drug to show a beneficial effect on overall survival compared to sorafenib. Previously, many drugs, such as sunitinib and linifanib, had been compared to sorafenib; however, they all failed to have any comparable beneficial effect. Based on the results of the REFLECT trial, in 2018, the FDA approved the use of lenvatinib as a first-line treatment for advanced HCC. Additionally, the EU, China, and Japan have also approved the use lenvatinib [30••].
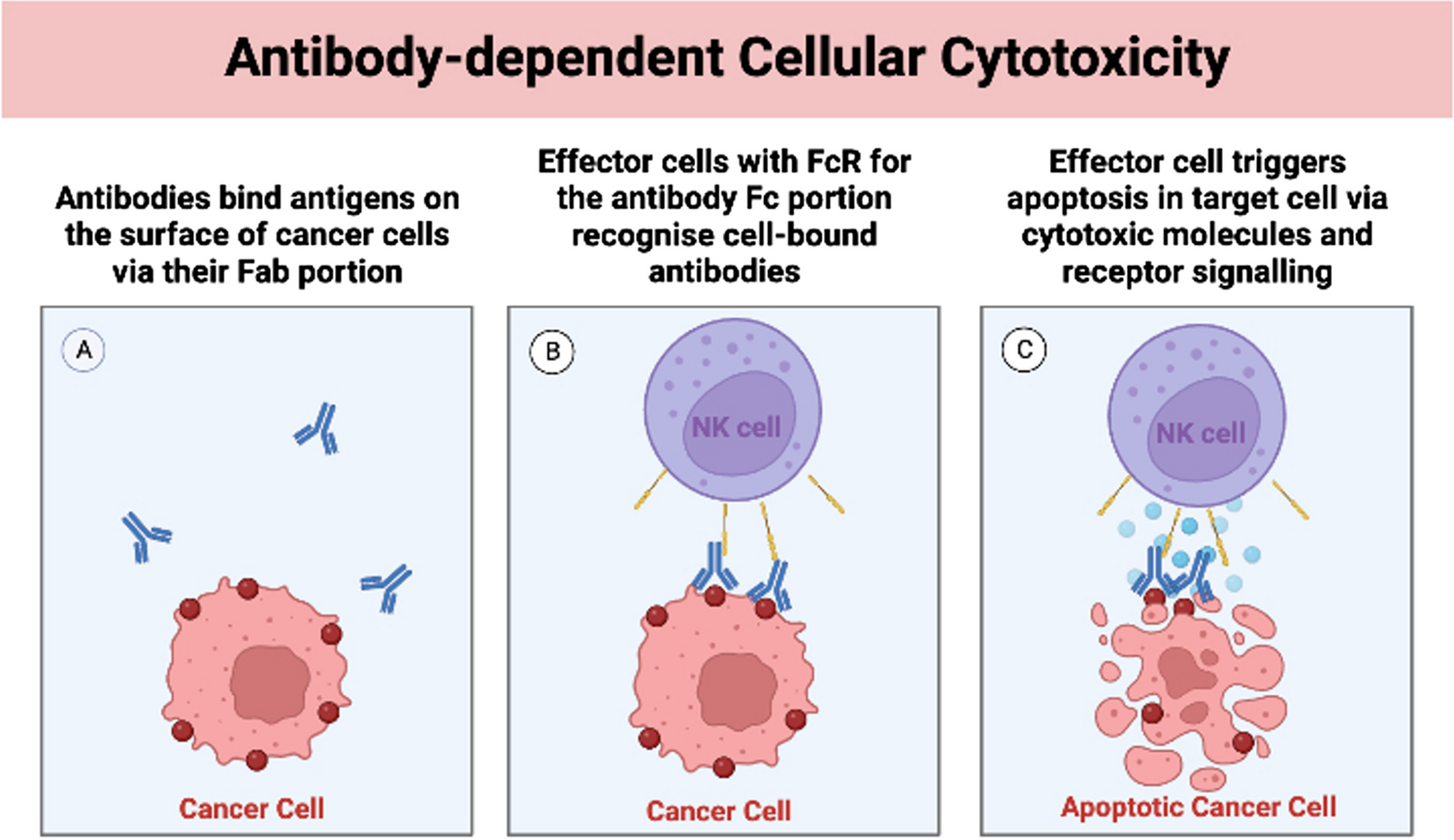
ImmunotherapyIn cases of liver cancer where surgical resection or liver transplantation is not feasible, attention is turned toward other treatment options, such as immunotherapy. This treatment modulates the immune system and enhances its ability to detect and kill cancer cells. One method of achieving this involves inhibiting immune checkpoints. For example, the PDL-1 pathway inhibits T cell activation, and this pathway is highly active in tumor tissue. The anti-PDL-1 antibody pembrolizumab, inhibits this pathway, resulting in increased immune system activity against tumor cells [31]. The KEYNOTE 224 clinical trial (NCT02702414) demonstrated that pembrolizumab had a promising response and reasonable adverse effects. According to the trial’s results, the median overall survival in patients that took pembrolizumab was 12.9 months, and 54% of patients were alive after 12 months. However, the trial lacked a randomized control group, one of its main limitations. These promising results led to larger studies being conducted, i.e., the KEYNOTE-240 (NCT02702401) and the KEYNOTE-394 (NCT03062358) clinical trials which showed promising results regarding the efficacy of pembrolizumab in the treatment of HCC [32••].
The CTLA-4 pathway inhibits T cell responses and has also been shown to be excessively activated in tumor cells. Drugs such as ipilimumab inhibit this pathway by blocking the activity of CTLA-4. These drugs have been FDA approved in the treatment of other cancers, such as melanoma and Hodgkin lymphoma, and clinical trials are underway to determine their efficacy in the treatment of liver cancer [33]. In addition to targeting immune checkpoints, tumor cells’ surface markers such as CD133, CD13, and CD44 are being used to target and destroy cancer stem cells via monoclonal antibodies. Since HCC originates from these stem cells, destroying them would significantly reduce the risk of recurrence, one of the main challenges in liver cancer treatment [34].
Combination of chemotherapy and immunotherapyCombinations of chemotherapy and immunotherapy are in development as a means to combat resistance and improve efficacy. Recently, a clinical trial (An Open-Label Phase 1b Trial of Lenvatinib Plus Pembrolizumab in Subjects With Hepatocellular Carcinoma—NCT03006926) assessed the efficacy of combining lenvatinib with pembrolizumab. The clinical trial was an interventional study that assessed a single group of patients that suffered from HCC but lacked a control group. This study provided evidence that the overall response rate (ORR) was 46% in 100 patients that were evaluated and reported that the tumor completely disappeared in 11% of the patients [30••]. When comparing these results with results from other clinical trials where lenvatinib and pembrolizumab were used as monotherapy, it is evident that combination treatment has much higher efficacy than monotherapy. To illustrate this, lenvatinib in the REFLECT trial (NCT01761266) showed an ORR of 24.1%, and pembrolizumab in the KEYNOTE-224 trial (NCT02702414) showed an ORR of 17%. These results demonstrate the superiority of a combined regimen compared to monotherapy [30••].
The recently published results of the IMbrave150 clinical trial (NCT03434379) revealed that the combination treatment of bevacizumab, an anti-VGEF antibody, and atezolizumab, an anti-PD-L1 antibody, had a higher overall survival when compared with sorafenib monotherapy. Specifically, the combination therapy involving bevacizumab and atezolizumab increased overall survival by 12.6% at 12 months and prolonged the progression-free survival interval by 2.5 months compared to the use of sorafenib. Specifically, overall mean survival with atezolizumab plus bevacizumab was 19.2 months on average, while overall mean survival with sorafenib was 13.4 months. Additionally, progression-free survival was 6.9 months with atezolizumab plus bevacizumab and 4.3 months with sorafenib. Based on these results, in 2020, the FDA approved the use of bevacizumab plus atezolizumab in patients with unresectable HCC [32••].
The evolving role of nanotechnologyIn order to overcome drug resistance, it is important to enhance drug delivery to cancer cells. Nanoparticles that can help achieve a highly accurate and precise drug delivery are currently under development. Nanoparticles are highly stable and have a variable structural design, low immunogenicity, and specific tissue/cell targeting abilities, making them a highly attractive modality for medical application and research [35].
The materials that constitute the nanoparticles affect their ability to deliver the drug. The most widely used material is polylactic acid (PLA) because of its ability to actively target tumor tissue as well as its biodegradability allowing it to be administered orally. Another factor contributing to the efficacy of drug delivery via nanoparticles is the method by which these drugs are delivered. One method is targeted delivery, which is split into passive and active targeted delivery systems. Passive targeting involves the leakage of the drug continuously from the nanoparticles into the tumor. On the other hand, active targeting involves an interaction between a specific receptor on the tumor cells and the nanoparticle, which results in drug release into tumor cells. Furthermore, researchers took advantage of the physiological differences in pH between tumor tissue and normal tissue, and designed nanoparticles that release their content in the setting of pathological pH, sparing healthy tissue. Overall, nanoparticles can help resolve the resistance issue by improving drug specificity and targeting. Additionally, nanoparticles limit the amount of healthy tissue exposed to the drug, which helps minimize side effects [28••].
Oncolytic virusesWith the advancements in technology and genetic engineering, a new therapeutic approach to liver cancer has started to emerge, which involves the use of oncolytic viruses which are genetically modified viruses that aim to infect and destroy cancer cells. These viruses exhibit their antitumor effects through two mechanisms. Firstly, they selectively replicate in cancer cells resulting in subsequent cell lysis. Secondly, they induce a systemic immune response that exhibits antitumor effects [36]. For example, ONYX-015 is a genetically engineered adenovirus in which the E1B gene has been deleted. This deletion prevents the virus from replicating in healthy tissue and allows it to replicate only in p53-deficient cells. Another example is the vaccinia virus which is derived from a poxvirus strain similar to smallpox. Initial research suggests that this oncolytic virus might be part of the treatment of liver cancer in the future; however, it is currently in clinical trials involving animal models and would require further extensive research before determining its efficacy [37].
Herpes simplex viruses (HSVs) are another group of viruses being investigated for their efficacy in the treatment of HCC. Given their strong replication ability and their large genome size that can accommodate multiple exogenous genes, HSVs have a promising potential as a treatment agent. Currently, a phase 1 clinical trial (Study of RP2 Monotherapy and RP2 in Combination With Nivolumab in Patients With Solid Tumours (NCT04336241)) is ongoing to assess the efficacy of genetically modified HSV1 in the treatment of HCC. As of now, no results have been published yet [38].
留言 (0)