In this national Delphi consensus study, the diagnostic and therapeutic pathways for lumbar facet joint radiofrequency denervation were investigated. Notably, some areas of expert agreement (central illustration), along with some controversies, were identified.
Diagnosis
In the field of diagnosis, expert agreement was high regarding the clinical presentation and physical examination of patients with suspected facet joint syndrome (statement 1: 98% agreement). Conversely, the need to perform a neuroimaging study only to exclude red flags and not make the diagnosis of lumbar facet joint syndrome did not reach an agreement among participants (statement 2: 61% first round agreement, 54% second round agreement). Instrumental examinations are not an essential step for the diagnosis of facet joint syndrome, since there are no effective correlations between clinical symptoms and degenerative spinal changes [14]. Single-photon emission computed tomography (SPECT) was suggested as the best imaging modality to detect potentially painful facet joints since it can identify the presence of active inflammation affecting the facet joint and provides detailed physiological information [15]. In fact, as reported by Jain et al. [16], patients with inflammatory involvement of facet joints confirmed by positive SPECT had a positive facet joint nerve block in 71% of cases compared with 43% of negative SPECT. Unfortunately, SPECT involves the use of a radioactive tracer with possible allergic reactions along with radiation exposure (gamma rays) by radioactive isotopes. Weak evidence exists supporting the routine use of SPECT for identifying painful lumbar facet joints, and further studies are required to assess its cost-effectiveness.
In two previously published studies, no association was found between facet joint involvement on magnetic resonance imaging (MRI) and denervation results [17, 18]. However, our analysis shows that many pain physicians still require lumbar spine imaging for the diagnosis of low back pain without a clear indication, probably with the aim to reassure their patients and themselves or to meet patients’ expectations. In fact, the increased number of MRI investigations is associated with higher rates of spine surgery, without a clear improvement in patient outcome [19, 20].
The number of medial branch (MB) nerve blocks and the technical notes to perform the block did not reach agreement among participants (statement 3: 51% first round agreement, 37% second round agreement). In fact, the panel showed different and conflicting opinions regarding the type of local anesthetic to use, the number of diagnostic MB blocks to perform and the interval between each diagnostic block before the denervation. The accuracy of a diagnostic block depends on several technical and anatomical factors and the aim of the procedure is to provide a selective block of the MB of the dorsal rami [21]. Unfortunately, MB nerve blocks are unlikely to achieve this accuracy due to the proximity of the intermediate and lateral branches of the dorsal rami, resulting in a potential non-selective neural blockade [22]. Since the MB innervates both the multifidus, the interspinal muscle, the ligament and the periosteum of the neural arch [23], a more protective approach would be to offer dual diagnostic MB blocks. This approach is associated with a higher success rate for LFRN and the diagnostic accuracy is improved if lidocaine and bupivacaine are used in two separate blocks [7]. However, it is well known that diagnostic MB blocks are frequently associated with a high false-positive rate [24] and some studies supported the presence of aberrant facet joint innervation [25]. On the contrary, as it was recently proposed, even a single MB block could be sufficient before LFRN [26].
Theoretically, a diagnostic intraarticular (IA) facet joint block could be more specific to avoid other anatomical structures. However, the diagnostic IA facet joint block cannot be suggested since it is less predictive than MB block for the outcome of LRFN, as reported in the Facet Treatment Study (FACTS) [27] and it is characterized by a higher technical failure rate [22, 28]. Some panelists suggested the use of steroids when performing a diagnostic IA facet joint block to increase the pain relief of the block. In our opinion, IA facet joint block is useful only in select populations where inflammation can be considered as a key characteristic of the disease, such as in rheumatoid or psoriatic arthritis. Therefore, the use of steroids is discouraged. On the contrary, some conditions should be treated with IA facet joint blocks since LFRN could be contraindicated. For example, in case of spondylolisthesis, the theoretical paravertebral muscle atrophy after LFRN can adversely impact this condition [29, 30]. Moreover, individuals with implantable cardioverter defibrillators or pacemaker-dependent patients can be at risk for complications during LFRN [31, 32], and a more conservative approach should be considered.
A substantial agreement was obtained for the use of ultrasound or fluoroscopic guidance to perform MB blocks with a small volume (≤ 0.5 ml) of local anesthetic at a maximum of three vertebral levels to reduce the spread to adjacent structures (statement 4: 78% first round agreement). In fact, as it was previously reported, a selective block with a small amount of local anesthetic is mandatory to increase the specificity of the block and to avoid an aberrant spread to adjacent anatomical structures [33]. The panelists suggested a 70% pain reduction to designate the block as “positive” and to increase its specificity (statement 5: 80% first round agreement).
Technical Aspects
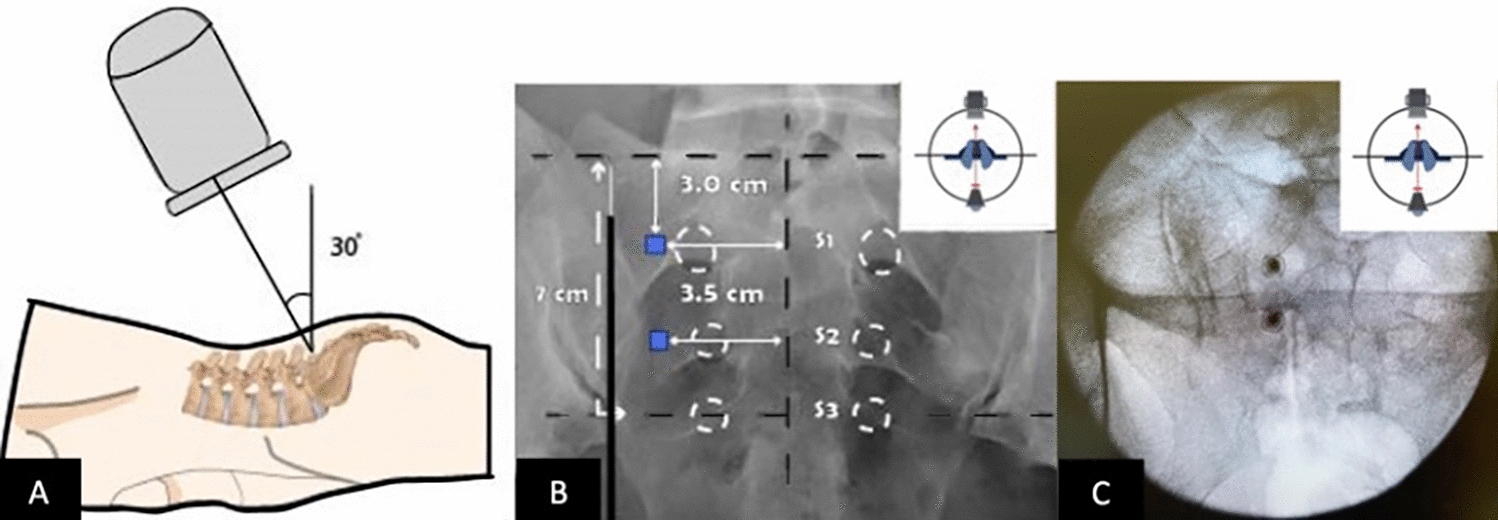
The panelists reached consensus on the technique of placing the needle for LFRN (statement 8: 80% first round agreement). The needle should be inserted tangentially along the course of the MB to allow a longitudinal contact between the cannula and nerve. Moreover, a proper anatomical confirmation should be obtained with cranial, caudal, and lateral fluoroscopic images as it was previously reported [34].
Motor stimulation should be performed to identify multifidus or other paraspinal muscle stimulation, thus indicating the proper placement [35], and to avoid the position of the needle in close proximity to the ventral ramus or spinal nerve (statement 9: 85% first round agreement). Moreover, the presence of paravertebral muscle twitching while performing LFRN may be a reliable predictor of long-term efficacy [36].
An agreement regarding the use of a needle with adequate diameter (18G needle) with 10 mm active tip while performing a LRFN was obtained only in round two (statement 7: 61% first round agreement, 71% second round agreement). Conversely, a great controversy emerged regarding the opportunity of using a curved tip needle. The curved needle has some advantages since it allows to rotate the tip to further increase the lesion size and to hug the base of the superior articular process of the facet joint [37]. Unfortunately, the curved tip is used by only a few pain physicians in Italy and this drawback should be adequately improved.
The importance of needle diameter and the length of active tip is based on electrophysiological principles, along with technical and physical aspects of radiofrequency [21, 38, 39], as it was reported also for knee joint radiofrequency [40]. Moreover, the transverse diameter of lumbar MBs is < 2 mm and even smaller (0.5 mm) at L5 level [41]. Consequently, there is the need to enlarge the lesion size enough to increase the chance of reaching the target and to create a lesion that envelops this structure [42]. For this reason, it is suggested to use an 18G needle with 10 mm active tip, preferably with a curved tip [43].
In case of bilateral low back pain, the simultaneous denervation of both sides offers the theoretical advantage of rapidly reducing the pain. However, this advantage is counterbalanced by the potential atrophy of paravertebral muscles. Dreyfuss et al. [29], in a small observational study, found a diffuse atrophy of the lumbar multifidus when performing a lumbar MRI 17–26 months after the denervation, along with greater disc degeneration. The same findings were confirmed in a subsequent study by Smuck et al. [44], and a significant loss of paravertebral muscles, requiring stabilization, was observed after cervical MB radiofrequency denervation [45]. On the contrary, recently published articles did not confirm these findings [46]. This conflicting evidence seems related to the use of different methods to measure muscular atrophy and does not consider possible catabolic effects of injected steroids on muscle tissue [47]. New studies with adequate sample size, and especially adequate evaluation protocols for the measurement of muscular atrophy, should be developed. Despite the uncertainty of evidence and the absence of agreement among panelists, the bilateral denervation of lumbar facet joints remains an undefined topic and should be explored in appropriate studies.
A strong consensus was obtained for the injection of local anesthetic (2% lidocaine) before LRFN to reduce procedural pain (statement 10: 78% first round agreement). The panelists underlined that a specific volume of local anesthetic to prevent pain from LRFN is not definable since every patient could require a different volume. For this reason, the panelists suggested the use of 0.5 ml 2% lidocaine per level and to increase the volume by a 0.5 ml increment as required to ensure a non-painful LRFN.
No consensus was obtained for the number of lesions to perform for each MB denervation (statement 11: 51% first round agreement, 66% second round agreement). As it was previously reported, two lesions should be performed at each MB [43]. The panelists agreed to use 80 °C for 90 s to perform a LRFN, but no consensus was reached for the 90° rotation of the needle to maximize the chance of producing an effective denervation without significant risk. However, we recognize that this statement needs to be contextualized with the type of needle used (presence/absence of curved tip) and different manufacturers’ machines, which might perform differently.
Outcome Evaluation
A strong consensus was obtained for the outcome evaluation after LRFN (statement 12: 88% first round agreement) and for the 50–60% pain reduction cutoff to define the procedure as “successful” (statement 13: 88% first round agreement). In fact, the panelists agreed to consider that the evaluation of only pain intensity is insufficient to assess the patient’s outcome after LRFN, and a more comprehensive evaluation to explore the physical and social function along with the psychological distress should always be performed [48].
An adequate rehabilitation program should be implemented after LRFN since it improves the neuromuscular control, the endurance, and the strength of many muscles involved in maintenance of dynamic spinal stability [45]. Almost all the panelists considered the importance of rehabilitation programs after LRFN (statement 14: 95% first round agreement). In fact, as previously reported, the rehabilitation program can enhance the results obtained with LRFN [50].
No consensus was obtained for the management of patients with inadequate pain relief after LRFN (statement 15: 66% first round agreement, 68% second round agreement). Regarding this topic, the panelists considered it vital to promptly reconsider the diagnosis looking for other pain generators after an ineffective LRFN. However, if the facet joint pain generator is confirmed, they did not agree whether to wait 3 months before repeating the denervation, or to use a different denervation technique. The 3-month cutoff to define the success of LRFN is based on a study by Cohen et al. [51]. In fact, in that study, the patients who underwent a new LRFN before the 3-months cutoff after the first LRFN, reported a less successful outcome. In another study, Son et al. [52] performed a retrospective analysis in patients who received more than one LRFN. Even if the authors found no difference in the pain reduction of the repeated LRFN; the mean duration of the first LRFN was 10.9 months. Consequently, it is possible to argue that after a successful LRFN lasting at least 3 months it is possible to repeat the LRFN without losing its efficacy. On the contrary, if the pain reduction was insignificant or the duration of the pain relief was limited, and the reevaluation of the patient leads to a decision to repeat the treatment, a new prognostic block is discouraged since it does not play a role in the decision to repeat the LRFN [53]. It is likely that the many panelists did not completely understand statement 15, and therefore uncertainties emerged.










留言 (0)