
記住我

What Is Known
Iron deficiency (ID) is the most common nutritional deficiency in children undergoing intestinal rehabilitation (IR). The diagnosis of ID can be difficult due to other coexisting nutritional deficiencies and/or other conditions that mimic ID. The unique needs of children undergoing IR may require modification of the approach to iron supplementation and treatment of iron deficiency anemia (IDA). What Is New Children undergoing IR should be routinely screened for iron deficiency prior to the onset of anemia. Parenteral iron is recommended in children undergoing IR with IDA or in those with iron deficiency without anemia and poor enteral tolerance. Multicenter collaboration is required to optimize screening and management strategies.Iron deficiency (ID) is common in general pediatrics and in children undergoing intestinal rehabilitation (IR), specifically those with intestinal failure (IF) and short bowel syndrome (SBS) (1,2). The documented prevalence of ID in this population ranges from 20% to 87%; Table 1 summarizes the estimated burden (3–8). Low serum iron concentration can be a sign of ID, acute or chronic infection, or systemic inflammation; therefore, using a low serum iron concentration alone to diagnose ID may lack specificity (9). Iron deficiency anemia (IDA) is an anemia resulting from insufficient iron to maintain erythropoiesis. Prevention, diagnosis, and treatment of IDA in children undergoing IR is important, because IDA is associated with the symptoms of decreased energy and quality of life, as well as signs of diminished oxygen delivery to tissues and possibly impaired neurodevelopment (10–12). Thus, the evaluation for and management of IDA is an essential component of IR (13–16). Yet, consensus among IR programs on laboratory diagnosis, screening interval, and optimal route for treatment is lacking. In this position paper, we review iron physiology and IR-specific pathophysiology, then provide recommendations for the diagnosis and management of IDA in this nutritionally vulnerable population.
TABLE 1. - Prevalence of iron deficiency in children undergoing intestinal rehabilitation Study Study type Population Sample size Prevalence Study definition of iron deficiency Smith et al(3) Prospective cohort Patients aged 0–18 yr requiring home PN for at least 3 mo 15 87% Unclear Ubesie et al(4) Retrospective cohort Children with pediatric intestinal failure 178 84% in PNEN = enteral nutrition; ID = iron deficiency; IDA = iron deficiency anemia; IF= intestinal failure; PN = parenteral nutrition; SBS = short bowel syndrome.
We reviewed relevant literature using PubMed/MEDLINE databases with the following Medical Subject Headings terms: IF, SBS, IDA, nutritional deficiency, parenteral nutrition (PN), IR, and micronutrient. Non-English language articles were excluded, and literature was evaluated through December 31, 2021. A grading method was not used due to the limited quantity and quality of pediatric IF-specific data. Individual authors completed relevant sections, which were reviewed and edited by coauthors. Available literature and expert opinion were used to discuss current practice for sections including screening, diagnosis, and treatment. In the case of disagreement, topics were discussed among the authors via conference calls/virtual meetings, and an iterative consensus was reached. For the specific recommendations, a survey was sent to all the authors and a 75% agreement among the authors was used to determine consensus. The author manuscript was reviewed, modified, and agreed upon by the executive committee of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) Intestinal Rehabilitation Special Interest Group using electronic and phone communication.
PHYSIOLOGY OF IRON ABSORPTION IN IR Gastric Digestion and Duodenal AbsorptionDissociation of enterally ingested iron from food begins in the stomach and continues through the proximal duodenum. Ferric iron (Fe3+) is released from food and converted by duodenal cytochrome b reductase (Dcytb) to ferrous iron (Fe2+), allowing transport across divalent metal transport protein 1 (DMT1) on the apical surface of the enterocyte. DMT1 has a low affinity for copper, lead, and manganese, which may lead to competitive inhibition of iron absorption, for example, during accidental ingestion or metal co-supplementation. The food matrix and pH may impact absorption at DMT1, especially in children with SBS on acid blockade or with pancreatic dysfunction. An acidic pH dissociates Fe2+ from protein in the stomach and may prevent Fe3+ from precipitating in the duodenum. Notably absent in SBS diets low in fruit, vitamin C is a reducing agent which enhances Dcytb function (17). For most children with SBS, the duodenum commonly remains anatomically intact, making enteral absorption feasible if transit time is supportive. Congenital diarrheas and enteropathies have not been associated directly with mucosal defects in DMT1 function. There is also no existing evidence that children with pediatric intestinal pseudo-obstruction (PIPO) have malabsorption of iron at DMT1 without the pathophysiology outlined in the sections below.
Mucosal Transport and Delivery to the LiverIron is stored on ferritin, an iron carrier protein, in the cytoplasm of the enterocyte upon absorption across the apical surface of the enterocyte. Some iron is sloughed off into the intestinal lumen with enterocyte turnover, and a portion is delivered to basolaterally located ferroportin 1 (FPN1), the only known iron exporter in humans (18,19). Iron is transported by FPN1 to the extracellular fluid where, with the assistance of hephaestin, it is re-oxidized, binds to plasma transferrin, and is transported with transferrin through portal circulation to the liver (20,21). When transferrin saturation (TSAT) rises above 75%, free iron spills into serum as non-transferrin bound iron, increasing susceptibility to gram-negative infections (20,22). This is especially important for children with IF and central venous catheters or ascites who are susceptible to infection.
Iron Recycling and Hepatic StorageUnder normal circumstances, iron is not excreted. This is a critically important message for the IR provider to consider when dosing and re-dosing iron. A negligible loss occurs in feces and in urine. Only menstruation, phlebotomy, hemorrhage, and epithelial turnover allow for iron loss from the body. In iron-sufficient individuals, roughly two thirds of total body iron is in red blood cells (RBC) and marrow, almost one third is stored in the hepatocytes and splenic and hepatic macrophages with relatively smaller but functionally important amounts of iron distributed in other tissues (21,23–25). The hepatic reserve is of interest to IR specialists as there is a correlation between iron overload and hepatic fibrosis, infection, and liver transplant waitlist mortality and other liver-related complications (26–33).
Regulation of Absorption by HepcidinIn the setting of negligible iron excretion, iron homeostasis depends on controlling the transfer of dietary iron to the blood plasma by FPN1 and distribution to tissues and body iron stores. To do this, the liver secretes the hormone hepcidin, reducing iron import in the intestine in response to hepatocyte and hepatic sinusoidal endothelial cell iron loading, thus preventing hepatic iron overload. Hepcidin binds to FPN1 in the intestine, causing occlusion, internalization, and degradation of this critical receptor (18,23). Just as insulin clears blood glucose, hepcidin clears iron from the bloodstream for about 24 hours. Hepcidin is appropriately low in ID, hemorrhage, and hemolysis and is high in chronic kidney disease, rheumatologic disease, infection, and iron refractory iron deficiency anemia. It is inappropriately low in thalassemia and hemochromatosis (18,23,34,35). All of these disease states can be seen in children undergoing IR, calling for a thoughtful assessment of serum iron concentration.
A low serum iron concentration alone does not indicate total body iron depletion that defines ID, requiring nuanced interpretation of common laboratory assessment based on physiology and anticipated pathophysiology. One study in children with IF failed to associate low iron concentration with anemia (6). Subsequent studies showed that while 1 of 3 of people with IF and anemia did have IDA, about 1 of 3 had anemia of inflammation (26). Of note, when TSAT was above 50% in this population, hemoglobin (Hb) did not increase with parenteral iron loading. Additionally, there was an association between increasing TSAT and hyperbilirubinemia as well as culture positivity (defined as a viral, urine, or blood culture obtained within 6 months of parenteral iron loading) (26).
In a research setting, serum hepcidin is being studied as a potential marker to differentiate ID from these conditions, but is known to be affected by certain factors, including age and circadian rhythm with lowest levels seen during the morning time. In an adult study of 2998 individuals, median serum hepcidin concentration was approximately 7.8 nM/L (22 ng/mL) in men, 4.1 nM/L (11.5 mg/mL) in premenopausal women, and 8.5 nM/L in postmenopausal women (36). Similarly, various assays yield variable reference ranges for serum hepcidin levels, ranging from 1 to 55 ng/mL in healthy individuals (37). In a pediatric study from Korea including 59 children between 5 months to 17 years, serum hepcidin correlated with iron status, with lowest levels seen in children with IDA (2 ng/mL) followed by those with ID without anemia (7.7 ng/mL) followed by those with normal iron levels (16 ng/mL) (38). This study further proposed cut-off points to differentiate IDA (serum hepcidin ≤2.735 ng/mL) from ID (serum hepcidin ≤6.895 ng/mL). In another study of adults with renal dysfunction, the hepcidin index (log[hepcidin]:log[ferritin] ratio) was noted to better predict ID (39).
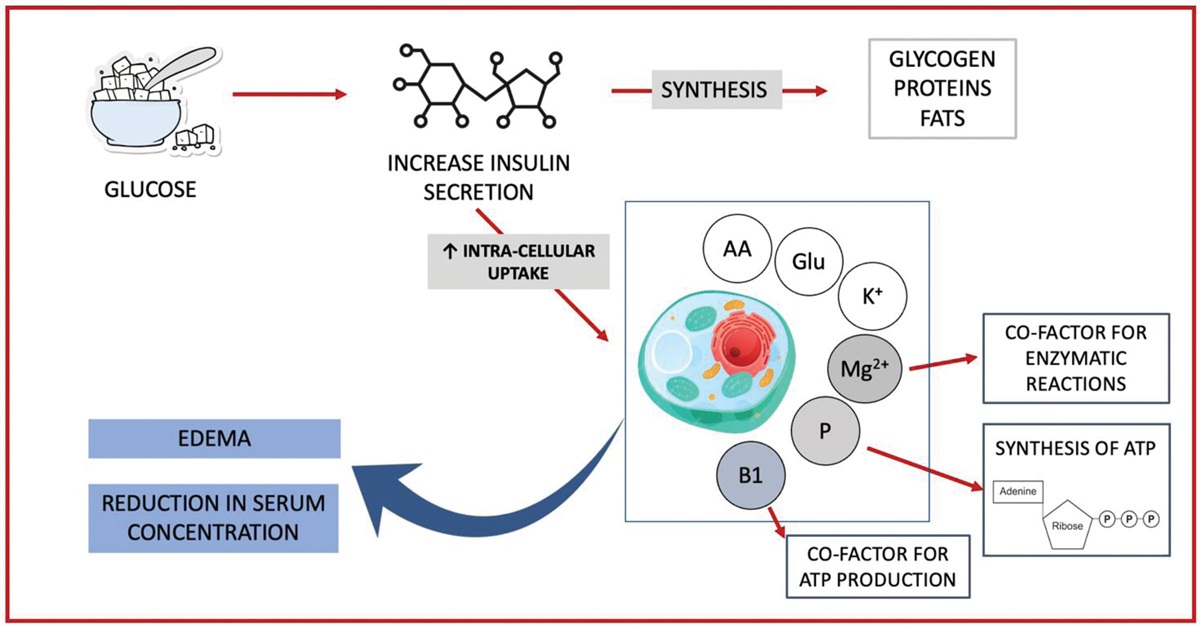
PATHOPHYSIOLOGY OF IRON DEFICIENCY IN IRIn theory and in practice, ID in children undergoing IR can result from inadequate intake, insufficient absorption at the mucosal surface (heme transporter or DMT1), altered motility, or elevated hepcidin, blocking import at FPN1. It may also occur due to blood loss or turnover through phlebotomy, gastrointestinal (GI) bleeding, or hematologic disease. The circumstances in which these occur in children undergoing IR are illustrated in Figure 1 and described below.
 FIGURE 1.:
FIGURE 1.: Physiology of iron metabolism and pathophysiology of iron deficiency in children undergoing intestinal rehabilitation.
1. Absorption at DMT1: Some children undergoing IR are at risk for IDA due to insufficient intake of iron-rich food. The transition period between weaning PN to a fully enteral diet is an especially high-risk time requiring the monitoring of the intake of iron-rich foods and appropriate use of enteral iron supplementation to prevent or correct IDA. If enteral supplementation or formula is tolerated during this vulnerable time, iron absorption in the duodenum is possible. However, as iron is not routinely present in PN solutions in North America (see iron added to PN below), low daily volumes of oral and enteral feedings and/or intolerance of enteral supplementation can easily result in mismatch of iron availability and need. Rarely, in children who have undergone antrectomy and proximal duodenectomy, iron is unlikely to be absorbed, a situation that would be expected to result in ID (40). It is not known if DMT1 or FPN1 are inducible outside of the proximal duodenum with iron loading. pH-induced reductions in iron solubility in the setting of pancreatic insufficiency or gastric acid suppression could contribute to ID, though this has not been demonstrated in a controlled manner.Pediatric feeding disorder is common in children with IF (41). Some children are limited in their tolerance of meat, iron-rich green vegetables, and seeds. Limited oral acceptance of iron-rich foods increases IDA risk, especially when feeding tubes are not used. Lastly, if high doses of copper, zinc, or calcium are supplemented with iron, there may be competitive absorption at DMT1 among some of these micronutrients (42).
2. Altered motility: If a child has significant gastroparesis, PIPO, or gastrojejunal bypass, with a persistently draining gastroenteric tube, enteral iron might escape into the gastric output (43). Clamping the gastric tube for 30 minutes after enteral iron administration into the gastric port may allow passage into the proximal duodenum for absorption. Likewise, if bowel transit time in a child with SBS is fast, or when the site of maximal iron absorption is bypassed as can be seen with gastrojejunal tubes, enterally supplemented iron may escape into feces. In a case series of children exclusively fed on jejunal feeds, a significant reduction in serum iron and transferrin levels was observed a year after commencing jejunal feeds (44). Another pediatric study of 150 children fed via tube feeding diet reported a 25% reduction in serum ferritin in 25% of children (45). A position paper by the European Society of Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) expert group on the use of jejunal tube feeding in children recommends that ID should be assessed in children on jejunal feeds every 6–12 months (46). Enteral iron should not be administered by jejunal route given low evidence for inducible FPN1 expression in the distal small intestine. 3. Decreased iron import at FPN1: Decreased iron import at FPN1 may occur because of high hepcidin concentrations due to a systemic inflammatory state from bowel inflammation, chronic kidney disease, or enteric or systemic infection. Children with dysmotility, bowel transplant rejection, or intestinal graft versus host disease may also have an element of bowel inflammation, leading to elevated hepcidin. Whether or not small bowel bacterial overgrowth (SBBO) leads to increased hepcidin transcription and decreased iron import at FPN1 has yet to be explored. These illnesses characteristically will show the attributes of anemia of inflammation (23,47). 4. Hemorrhage: Bleeding in children undergoing IR occurs with anastomotic ulcers, bowel inflammation, varices, gastric ulcers, serial transverse enteroplasty due to bleeding from staple line, or phlebotomy—as seen in adult as well as neonatal studies (48–53). Anticoagulation used for deep venous thrombosis prophylaxis may also exacerbate hematochezia (54). In these circumstances, in the absence of inflammation, iron is readily absorbed from the GI tract but lost in excess of intake. Hemorrhage may be obvious or, commonly, iron losses may be subclinical, such as in situations of frequent phlebotomy through infancy and early childhood or occult losses from anastomotic ulceration. 5. Prematurity: Healthy term infants are born with sufficient iron stores to meet their iron needs until approximately 6 months of age. From 6 to 24 months of age, iron requirements per kilogram of body weight are higher than during any other period of life because of rapid growth (55). Preterm infants are at increased risk for IDA as iron accumulation is highest in the third trimester (50,56,57). After birth, iron stores in premature infants are depleted in 6–8 weeks, and infants with higher growth velocity deplete tissue iron stores quickly. It is noted that the Hb nadir is lower and occurs earlier in infants with gestational age 28–32 weeks compared to term infants (58). Other conditions such as maternal ID, intrauterine growth restriction, and neonatal or placental blood loss during gestation can increase risk of postnatal IDA. This is exacerbated by surgery or prolonged absence of feeding in children undergoing IR. 6. Adolescence: In adolescence, iron requirements increase due to blood volume expansion, menstruation, and muscle mass increase (42). Iron status in children with SBS and IF should be monitored closely during this time. No recommendation could be provided about the optimal screening interval in adolescents undergoing IR due to lack of supporting evidence and significant variability among author practices. RECOMMENDED IRON INTAKE AND PREVENTION OF IRON DEFICIENCY IN IRThe U.S. Dietary Reference Intakes include a Recommended Dietary Allowance (RDA) for iron. This refers to the average daily iron intake level sufficient to meet the needs of most healthy individuals in a particular life stage and does not account for pathology-related deficits. Table 2 provides the RDA for iron for term infants and throughout the life cycle. A preterm infant requires a daily iron intake of 5–6 mg/kg enterally (56–58). In children with gastroparesis, clamping the gastric tube for 30 minutes after enteral iron administration should be considered. It has been suggested that children with IF require more iron than the RDA; maintenance enteral iron doses in IF range between 4 and 6 mg/kg/day and significant IDA with ongoing losses may require doses higher than 10 mg/kg/day of enteral elemental iron (59).
TABLE 2. - Recommended Dietary Allowance (RDA) for iron (mg/day) RDA for enteral iron Age Male Female Birth to 6 mo 0.27 mg* 0.27 mg* 7–12 mo 11 mg 11 mg 1–3 yr 7 mg 7 mg 4–8 yr 10 mg 10 mg 9–13 yr 8 mg 8 mg 14–18 yr 11 mg 15 mg Estimated parenteral requirements of iron Age Requirement (µg/kg/day) Preterm 200–250 0–18 yr 50–100 Maximum dose 5 mg/day*Adequate intake – intake at this level is assumed to ensure nutritional adequacy; established when evidence is insufficient to develop an RDA.
In children receiving long-term PN, who cannot maintain adequate iron status using enteral iron supplements, intravenous (IV) supplementation may be needed (59). Parenteral iron can be given daily when added to PN solution or as intermittent infusions. If parenteral iron is given in PN daily, and assuming no enteral iron supplementation, recommendations for routine parenteral iron maintenance dose is 200–250 µg/kg/day in preterm infants and 50–100 µg/kg per day up to a maximum dose of 5 mg/day in infants and children (Table 2) (59).
There is a wide range of practices when providing IV iron with associated risks and benefits. Some concerns regarding the use of iron in PN have been raised, specifically regarding the potential stability of the PN formulation and the formation of reactive oxidants potentially increasing the risk of precipitation, iron overload, and DNA adducts (60,61). The addition of iron to PN solutions is further described below. Episodic parenteral iron infusion is associated with a risk of infusion reaction, which may be life threatening but remains very rare. Infants/children who receive erythropoietin treatment and infants who have had significant, uncompensated blood losses may initially need a higher iron dose (62). Iron supplementation after blood transfusion may be indicated in the setting of a large iron deficit.
Recommendation: In children with suspected altered GI motility (gastroparesis, PIPO) or a history of gastrojejunal bypass, persistently draining G tube, we recommend clamping the G tube for 30 minutes after enteral iron administration into the gastric port for improved absorption into the duodenum. (8 authors in favor)
ASSESSMENT OF IRON STATUS IN IR Testing for IDThe gold standard to diagnose IDA is bone marrow biopsy, which is impractical for diagnosis and monitoring. The available options for laboratory testing include measurement of Hb, TSAT, RBC count, serum iron concentration, total iron-binding capacity (TIBC), hematocrit and RBC indices, serum ferritin (SF), soluble transferrin receptor, reticulocyte count, serum hepcidin (in a research setting), zinc protoporphyrin, and a reticulocyte Hb content (1,63). In a survey of almost 400 pediatric hematologists evaluating IDA, more than half obtained a serum iron and TIBC, whereas 30% obtained TSAT, and 70% obtained SF (63). Careful selection of the available tests is important in IR because serum iron and SF are both strongly affected by inflammation, and can be poor indicators of ID in cases of infection or inflammation. Obtaining a C-reactive protein (CRP) when assessing iron status in these children may help distinguish true abnormalities from an acute phase response. Serum iron and TIBC have also been shown to have a diurnal variation, peaking in the morning (64).
Recommendation: Screening for ID/IDA in children undergoing IR should not be based on a Hb and mean corpuscular volume (MCV) alone. We recommend screening for IDA based on a complete blood count (CBC), SF, TSAT, serum iron concentration, and TIBC. (8 authors in favor)
Recommendation: A CRP should be obtained while screening for ID as SF is an acute phase reactant. (8 authors in favor)
The frequency of iron status monitoring in IR programs varies from every 3 months to annually and may depend on whether it is routine screening versus assessment of response to therapy (65). Other nutrition screening varies from every 3–6 months depending on factors including ID risk, nutritional status, enteral tolerance, and stage of rehabilitation. The practice of phlebotomy itself should be re-evaluated in IR, as 1 mL of packed RBC blood loss results in approximately 1 mg of iron loss, so a child with a hematocrit of 40% loses 0.4 mg of iron with each 1 mL of whole blood, or up to 10 mL and 10 mg of iron loss for a basic metabolic panel, magnesium, and phosphorus level depending on the center’s draw technique (66).
Recommendation: Children undergoing IR should be screened for ID/IDA. We recommend screening every 3–6 months. (7 authors in favor, 1 opposed)
Table 3 describes a set of laboratory assessments that can be used to differentiate ID from commonly encountered conditions in children undergoing IR. Patients may have IDA, vitamin B12, and/or folate deficiency with resulting normal MCV. MCV can also be elevated in liver disease, making it an unreliable marker for ID assessment in children with IF-associated liver disease (IFALD). Deficiencies of copper or zinc, or preexisting hemoglobinopathies can lead to microcytosis. Figure 2 describes an algorithm for determining IDA in children undergoing IR based on TSAT and SF. We propose 3 distinct categories: 1. Children without ID; 2. Children with ID without anemia; and 3. Children with IDA (Table 3). Caution should be taken in the assessment of IDA in cases of a suspected infection or inflammation such as central line-associated bloodstream infections, SBBO, childhood viral infections, and other inflammatory conditions.
TABLE 3. - Laboratory markers commonly used to differentiate ID/IDA from commonly encountered conditions in children undergoing IR Lab test No ID ID IDA IRIDA Anemia of inflammation Vitamin B12 deficiency or folate deficiency anemia Hemoglobin N N Low Low Low Low MCV N/elevated N/low Low Very low Low to N Elevated Serum iron N Low Low Very low N N TIBC N N/elevated Elevated Elevated Variable N TSAT N N Low Very low Low to N N SF N Low Low N/elevated N/elevated N STR* N Elevated Elevated N N N Hepcidin N Low Low Elevated Elevated NID = iron deficiency; IDA = iron deficiency anemia; IR = intestinal rehabilitation; IRIDA = iron-refractory iron deficiency anemia; MCV = mean corpuscular volume; N = normal; SF = serum ferritin; STR = soluble transferrin receptor; TIBC = total iron binding capacity; TSAT = transferrin saturation.
*Soluble transferrin receptor can be elevated in patients with hemolysis or with administration of erythropoiesis-stimulating agents.
 FIGURE 2.:
FIGURE 2.: Proposed algorithm for determining iron status in children undergoing intestinal rehabilitation based on transferrin saturation (TSAT) and serum ferritin levels (SF).
Recommendation: Vitamin B12, zinc, and copper deficiency should be evaluated based on anatomic risk and in children not responding to conventional treatment. (7 authors in favor, 1 opposed)
Recommendation: While assessing iron status in children undergoing IR, we recommend categorizing children into 3 categories: 1. Children without ID; 2. Children with ID without anemia; and 3. Children with IDA. This will enable IR providers to make an informed decision regarding treatment. (8 authors in favor)
Screening for Other Conditions Including ThalassemiaMicrocytosis is a common finding in carriers of alpha or beta thalassemia. However, anemia is not generally profound in people with thalassemia, and iron parameters are often normal or increased. Screening for thalassemia should be considered in children undergoing IR with features similar to IDA refractory to conventional iron therapy to avoid dangerous hepatic overload (59). This may be especially important in patients with Pacific Islander, Southeast Asian, South Asian, Southwest Asian, or North African ancestry.
Recommendation: Screening for thalassemia should be considered in children not responding to conventional treatment in certain patient populations. (6 authors in favor, 1 opposed and 1 abstained from commenting)
Role of EndoscopySince inadequate intake or frequent blood draw are common causes of IDA in the IR population, endoscopy is not routinely required. However, it is appropriate to consider an endoscopy in cases of persistent IDA, or IDA associated with low albumin, low zinc, low vitamin D, elevated CRP, or IDA not responding to enteral treatment. Other conditions that increase the risk of IDA and may require an endoscopy are anastomotic ulcers, and intestinal inflammation.
Recommendation: In the assessment of ID in children undergoing IR, endoscopy is not routinely recommended. It can be considered if there is a poor response to enteral iron or if concerning signs and symptoms suggest GI bleeding, or intestinal inflammation. (6 authors in favor, 1 opposed and 1 abstained)
Referral to a HematologistReferral to pediatric hematology involves institution-specific considerations and is often reserved for select cases, such as unresponsiveness to oral and/or parenteral iron therapy, the need for multiple blood transfusions in the absence of a GI cause, or pancytopenia without portal hypertension.
Recommendations: Referral to a hematologist can be reserved for lack of recovery of Hb with iron supplementation, presence of pancytopenia, or difficulty distinguishing between multiple micronutrient deficiencies, portal hypertension, cancer, or other marrow insufficiency. (8 authors in favor)
TREATMENT OF ID IN IRSeveral factors must be considered in determining the appropriate route of treatment for each child. In this section, we discuss the available methods of iron supplementation (Table 4) and unique considerations for children undergoing IR.
TABLE 4. - Iron formulations available in the United States Iron type Standard dosing Formulation(s) Cost* Oral/enteral Ferrous sulfate 3–6 mg/kg/day 75 mg/mL (15 mg elemental iron)*Based on the Federal Supply Schedule.
With many families looking to reduce medication burden, iron-rich food offers an alluring treatment option. No studies have examined the contribution of iron-rich foods to ID treatment in children undergoing IR. However, iron-rich food supplementation has been attempted in other clinical settings. In adult women with celiac disease, oral iron supplementation was superior to iron-rich diet; no participant in the iron-rich diet group successfully achieved goal iron intake (67). ID is less common in children who eat meat than in children who are vegetarian, perhaps due to absorption of iron through heme (68). In children undergoing IR, dietary treatments may have limited appeal as the high prevalence of feeding disorders and restricted diets may limit intake (41). However, in qualitative studies, some families whose children do have enteral tolerance have expressed a desire to pursue this option (69).
Recommendations: There is insufficient evidence to recommend a trial of dietary enrichment alone for the treatment of ID. Dietary enrichment may be used as an adjunct to supplementation. (8 authors in favor)
Enteral SupplementationOral and enteral iron supplementation carry many of the same benefits and challenges as dietary enrichment. Oral supplements are most commonly available as iron salts which can be administered in tablet or liquid suspension. The liquid formulations can be administered via gastrostomy tube. Oral supplementation traditionally occurs via the administration of ferrous sulfate, ferrous gluconate (FG), or ferrous fumarate. These formulations present low-cost, readily available options. The usual recommended dosing for prevention of ID is 3 mg/kg/day and for treatment of IDA is 4–6 mg/kg/day. As mentioned above, children undergoing IR may require higher than the generally recommended dosing (4–6 mg/kg/day for prevention and as high as 10 mg/kg/day elemental iron for treatment). Some children undergoing IR have feeding difficulties or avoidant restrictive feeding disorders and experience symptom exacerbation with enteral iron. Issues with intolerance may be overcome by starting with a lower dose and gradually increasing the dose or diluting the dose with a diluent like water or oral rehydration solution before administration. Studies in adults have shown that increasing the dose of oral iron supplementation and dividing the dose into 2–3 doses increased serum hepcidin levels and reduced fractional iron absorption (70). This is hypothesized to worsen GI discomfort or tolerance through iron accumulation in the intestine. Therefore,
留言 (0)