
記住我


KEY POINTS
Question: Is a higher opioid dose during anesthesia for acute trauma patients associated with lower mortality or organ injury rates?
Findings: Opioid administration is associated with a lower mortality in severely injured trauma patients.
Meaning: Anesthesia practice of higher dose opioids in acute trauma patients appears reasonable, given simultaneous resuscitation priorities.
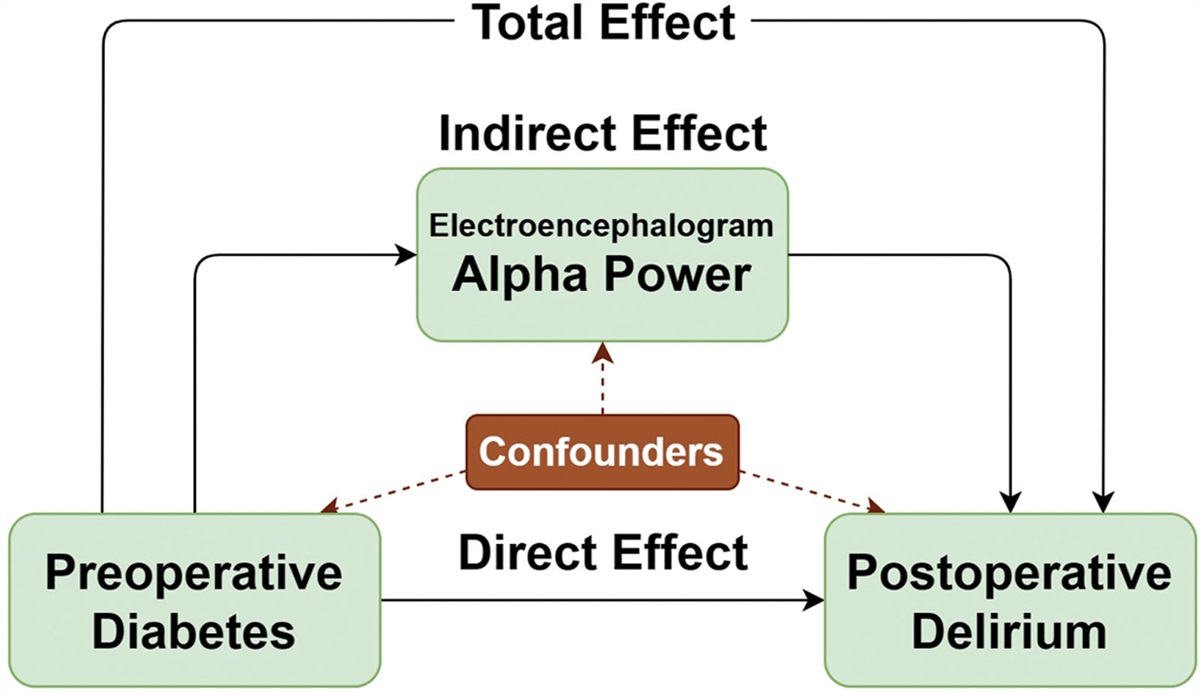
Complex trauma patients require balancing of analgesia with hemodynamic, hemostatic, and metabolic resuscitation requirements in the dynamic pathophysiology of severe injury.1,2 Use of opioid analgesia in the anesthetic management of acute trauma patients is not well described, and opioid-sparing strategies used in elective surgery do not correlate to the severely injured trauma population. Hypotension is frequent, and may be permissive, in acute trauma patients until the source of bleeding is controlled,3 which may limit opportunities for opioid administration. However, there are theoretical advantages when using higher dose opioids in severely injured trauma patients: preclinical studies demonstrating preservation of microcirculatory flow and endothelial homeostasis support the use of higher dose opioids in at least 1 major trauma center.4 Potential physiologic benefits must be weighed against risks of opioid tolerance and persistent postinjury opioid use.5 Given the limited available data, a contemporary analysis of opioid use during general anesthesia for severely injured trauma patients would be useful to better understand outcomes associated with their use.
 Figure.:
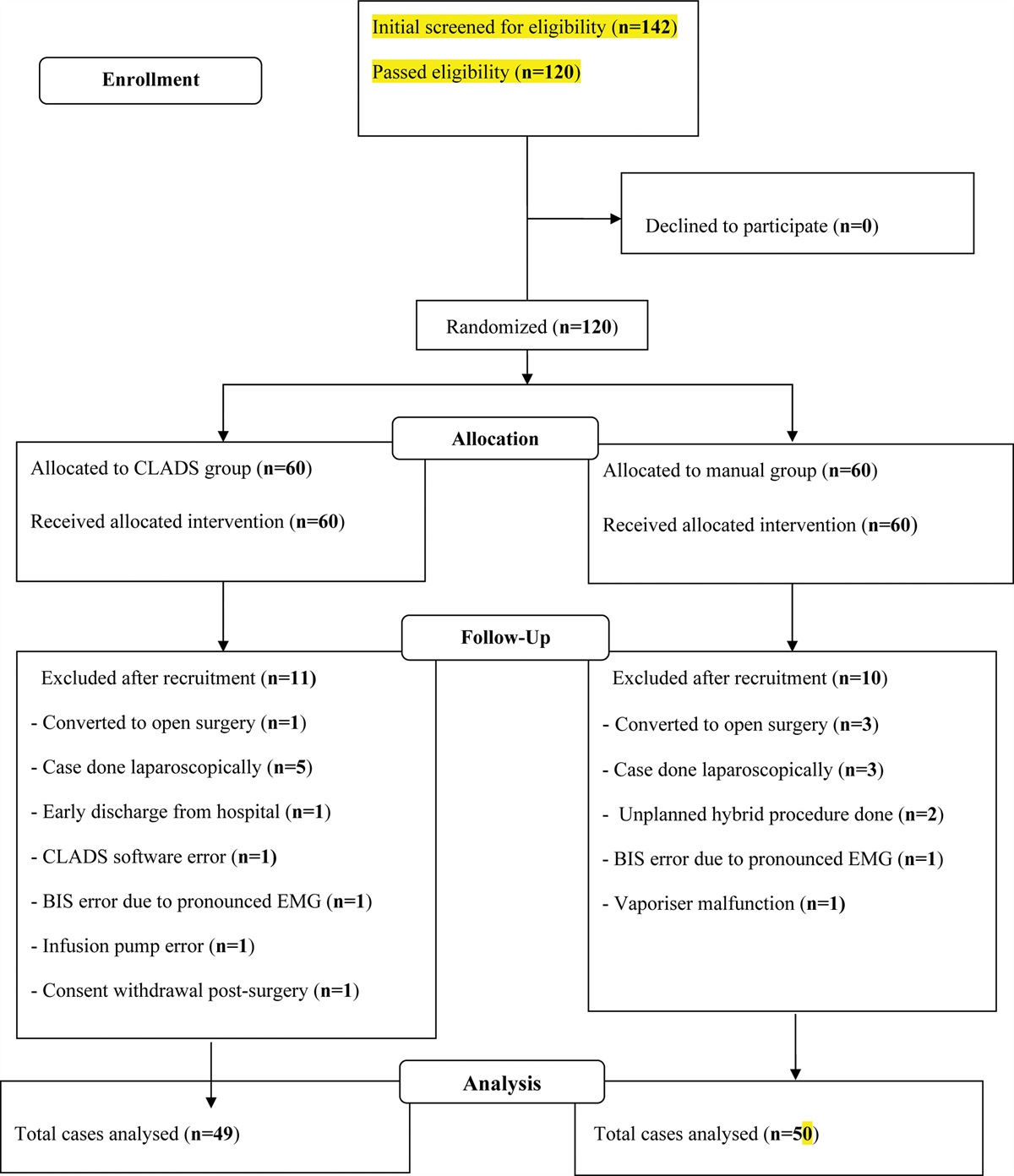
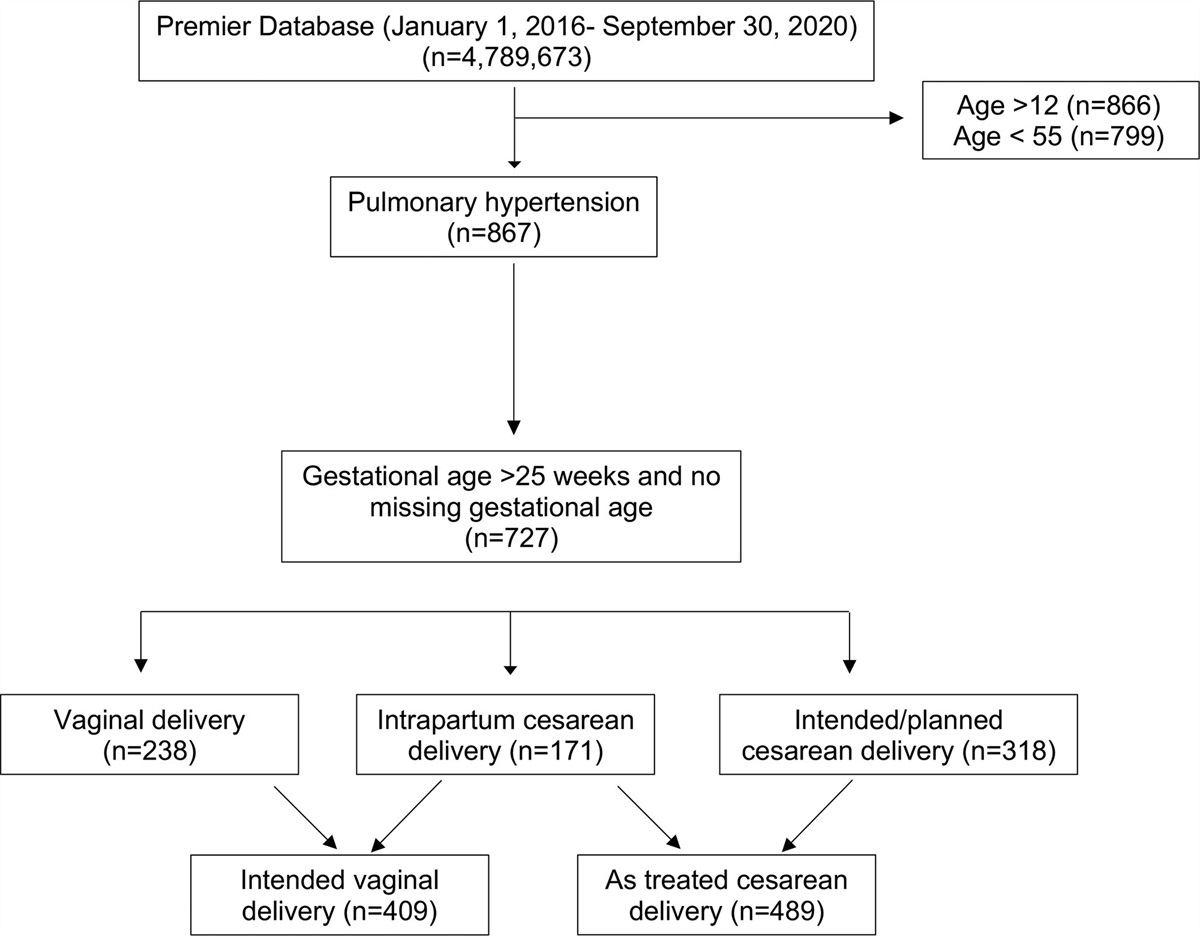
Figure.: CONSORT flow diagram. CONSORT indicates Consolidated Standards of Reporting Trials; IR, infusion room; OR, operating room.
This is a preplanned, secondary analysis of data from the Pragmatic, Randomized, Optimal Platelet and Plasma Ratios (PROPPR) study6 to examine the impact of opioid dose on mortality in severely injured patients. Limited anesthetic data were collected during PROPPR, although anesthesia and analgesia were not protocolized. Based on clinical experience, we hypothesized that an anesthetic with higher opioid doses would be associated with a lower likelihood of death in severely injured trauma patients.
METHODS Data RegistryThe PROPPR database was used to access deidentified subject information, including demographics, mechanism of injury (blunt or penetrating), organ injury patterns, study site, injury severity scores (ISSs), shock index (heart rate, systolic blood pressure), PROPPR treatment arm, mortality at 6 hours, 24 hours, and 30 days following the initial surgical procedure as well as secondary outcomes related to infection, renal, and pulmonary function. The PROPPR study was registered on clinicaltrials.gov (https://clinicaltrials.gov/ct2/show/NCT01545232) on March 5, 2012,6 before any enrollment activity. For patients requiring an initial anesthetic, opioid dose was reviewed from prospectively collected electronic and paper anesthesia records. This article follows the Consolidated Standards of Reporting Trials (CONSORT) guidelines. The PROPPR study was conducted with exception from informed consent, including community consultation with delayed patient or legally authorized representative consent. This secondary analysis (as for all secondary analyses of PROPPR data) with subjects identified only by study number was approved by the Committee for the Protection of Human Subjects at UTHealth Houston with waiver of requirement for informed consent.
Study Population and Outcome MeasuresPROPPR subjects met the highest trauma level activation, were estimated 15 years or older, received directly from the scene of injury, acquired initial transfusion within the first hour of arrival or during prehospital transport, were predicted to require a massive transfusion, and randomized to 1 of 2 transfusion ratio groups.6 The study group for this secondary analysis included all subjects undergoing an emergency surgical or radiological procedure with a general anesthetic. Subjects with missing observations for opioid dose, pertinent demographic variables, and procedure times were excluded (Figure).
Primary and Secondary Outcome VariablesPrimary outcomes for this study mirrored PROPPR outcomes: mortality at 6 hours, 24 hours, and 30 days for subjects undergoing an emergent surgical procedure requiring general anesthesia. Twenty-three secondary outcomes were defined a priori in PROPPR, and this secondary analysis included those relevant to acute anesthesia care:
Acute lung complications (acute lung injury and adult respiratory distress syndrome [ARDS], occurring in 29.1% of PROPPR cohort) Systemic inflammatory response syndrome (SIRS, overwhelming systemic response to infection, occurring in 65.7% of PROPPR cohort) Acute kidney injury (occurring in 23.4% of PROPPR cohort) Ventilator-associated pneumonia (VAP, occurring in 17.7% of PROPPR cohort) Multiple organ failure (MOF, altered organ function in at least 2 organ systems, progressive or profound organ dysfunction incompatible with life, occurring in 5.1% of PROPPR cohort).7Prior secondary analysis of PROPPR data affirmed the low incidence of ARDS with the only modifiable predictor being initial crystalloid exposure.8
Exposure VariableOpioid dose was the primary exposure variable, and in subjects who received opioids, the dose was calculated as morphine milligram equivalents (MMEs)/h using anesthesia start and end times or procedure start and end times if anesthesia times were unavailable.9 Opioid dose/h was collated as a continuous variable. After separation of those who received no opioid (group 1), remaining subjects were divided into 4 equal-sized quartiles with distinct clinically relevant ranges of opioid doses.
Statistical AnalysisDescriptive statistics were used to evaluate patient characteristics and primary and secondary outcomes across opioid groups. Categorical variables are reported as frequencies and percentages. Since the distribution of continuous variables was skewed, median and interquartile range (IQR) are reported. Chi-square and Kruskal-Wallis tests were used to assess unadjusted association of categorical and continuous variables with opioid dose groups. Since there were multiple groups and outcome variables, we did not perform univariable pairwise comparisons among all opioid groups to minimize type I error inflation due to multiple comparisons. Generalized linear mixed models with logit link and binomial distribution assumptions were used to assess the impact of opioid dose on primary and secondary outcomes. Since opioid dose was not randomized, covariates, including age, sex, race (white, black, and other), PROPPR treatment arm, mechanism of injury, shock index, injury mechanism, and ISS that were associated with opioid dose (P ≤ .15), were assessed as potential confounders and kept in the final adjusted model as fixed effect factors when they remained significant in the model or changed the effect estimate of opioid dose by >10%. Since the hemodynamic status of patients could affect clinical management and opioid use, admission shock index as a marker of hemodynamic status was included in the adjusted model as a fixed effect factor a priori. Study site was included in the adjusted models as a random effect factor. Additional sensitivity analysis was conducted with removal of those that died within 24 hours to remove the effect of survivor bias. All statistical tests were interpreted at a 0.05 significance level and conducted using SAS 9.4 program (SAS Institute Inc, 2013).
RESULTSSix hundred eighty patients enrolled in the PROPPR study with median ISS of 26, identifying severe injury.6 After excluding subjects who received no anesthetic or did not have complete anesthesia records (n = 154, 22.6% of initial cohort), the sample size was 526 (Figure). Eighty-three subjects received no opioid, identified as group 1. Those receiving opioids were divided into 4 equal-sized quartiles with a range of clinically relevant low- to high-dose opioids (Figure):
Quartile 1: 0.1 <dose ≤4.61 mme/hr (n = 110) Quartile 2: 4.62 < dose ≤8.95 mme/hr (n = 111) Quartile 3: 8.96 <dose ≤15.44 mme/hr (n = 111) Quartile 4: > 15.45 mme/hr (n = 111) Table 1. - Patients’ Demographics by Opioid Doses Variable No opioid Dose quartile 1 (0 < dose ≤ 4.61) Dose quartile 2 (4.61 < dose ≤ 8.95) Dose quartile 3 (8.95 < dose ≤ 15.45) Dose quartile 4 (dose > 15.45) P value n 83 110 111 111 111 Age, median (IQR) 35.0 (26.0–53.0) 41.5 (25.0–55.0) 29.0 (24.0–43.0) 31.0 (23.0–45.0) 33.0 (23.0–45.0) .06 Male sex, n (%) 67 (80.7) 79 (71.8) 90 (81.1) 92 (82.9) 98 (88.3) .04 Race, n (%) .14 White 52 (62.7) 78 (70.9) 61 (54.9) 64 (57.7) 65 (58.6) Black 26 (31.3) 23 (21.9) 38 (34.2) 35 (31.5) 41 (36.9) Other 5 (6.0) 9 (8.2) 12 (10.8) 12 (10.8) 5 (4.5) Hispanic ethnicity, n (%) 15 (18.1) 23 (20.9) 21 (18.9) 24 (21.6) 11 (9.9) .16 Treatment group, n (%) .07 1:1:1 33 (39.8) 65 (59.1) 62 (55.9) 53 (47.7) 57 (51.3) 1:1:2 50 (60.2) 45 (40.9) 49 (44.1) 58 (52.3) 54 (48.7) Shock index, median (IQR) 1.4 (1.1–1.9) 1.1 (0.8–1.3) 1.1 (0.9–1.4) 1.1 (0.9–1.4) 1.1 (0.8–1.3) <.01 Injury severity score, median (IQR) 34 (25.0–45.0) 29.0 (20.0–43.0) 25.0 (14.0–34.0) 25.0 (16.0–34.0) 26.0 (16.0–38.0) <.01 Injury mechanism, n (%) .04 Blunt 44 (53.7) 62 (56.4) 42 (38.5) 44 (40.7) 50 (45.4) Penetrating 38 (46.3) 48 (43.6) 67 (61.5) 64 (59.3) 60 (54.6) Anesthesia time (h), median (IQR) 2.45 (1.6–3.6) 3.5 (2.8–5.1) 3.8 (2.8–5.2) 3.1 (2.1–4.1) 2.9 (2.1–3.95) <.01Abbreviation: IQR, interquartile range.
Comparison of subject characteristics across all 5 groups is summarized in Table 1. There were differences in ISS (P < .01) and shock index (P < .01) across opioid dose groups, with the highest ISS (median = 34) and shock index (median = 1.4) in the no-opioid dose group. There were differences in procedure duration across all opioid groups (P < .01), with the shortest duration (median 2.45 hours) in the no opioid dose. There were differences in mechanism of injury across all opioid groups (P = .04) with higher incidence of blunt injuries in the no-opioid and lowest opioid dose groups. There were no differences in age, ethnicity, race, or PROPPR treatment group. There were differences in sex across all opioid groups (P = .04) with a lower incidence of male subjects in the lowest dose opioid group (71.8%) although this is less clinically relevant given the male preponderance in all groups (remainder 80.7%–88.3%) (Table 1).
MortalityIn unadjusted univariable analysis, there were differences in mortality across all opioid groups (P < .01) with higher mortality in the no-opioid group at 6 hours, 24 hours, and 30 days (Table 2). Sensitivity analysis with subjects remaining alive at 24 hours resulted in removal of 50.6% of subjects in the no-opioid group and only minor attrition in the opioid dose quartiles (removal of 3, 3, 4, and 5 subjects, respectively) (Table 3). In the group alive at 24 hours, there were differences in mortality (P < .001), with higher mortality at 30 days persisting in the no-opioid group (Table 3).
Table 2. - Univariable Associations of Opioid Dose Quartiles With Mortality and Morbidity as the Primary and Secondary Outcomes, Respectively Variable No opioid Dose quartile 1 (0 < dose ≤ 4.61) Dose quartile 2 (4.61 < dose ≤ 8.95) Dose quartile 3 (8.95 < dose ≤ 15.45) Dose quartile 4 (dose > 15.45) P value n 83 110 111 111 111 Primary outcomes Mortality at 6 h (%) 37 (44.6) 2 (1.8) 2 (1.8) 4 (3.6) 3 (2.7) <.001 Mortality at 24 h 42 (50.6) 3 (2.7) 3 (2.7) 4 (3.6) 5 (4.5) <.001 Mortality at 30 d 52 (62.6) 19 (17.3) 12 (10.8) 8 (7.2) 12 (10.8) <.001 Secondary outcomes Lung complications (ALI or ARDS) 16 (19.3) 27 (24.5) 23 (20.7) 14 (12.6) 16 (14.4) .14 Systemic inflammatory response syndrome 36 (43.4) 83 (75.4) 77 (69.4) 81 (73.0) 87 (78.4) <.001 Acute kidney injury 18 (21.7) 24 (24.5) 25 (22.5) 26 (23.4) 31 (27.9) .85 Ventilator-associated pneumonia 14 (16.9) 30 (27.3) 16 (14.4) 21 (18.9) 19 (17.1) .14 Multiple organ failure 5 (6.0) 6 (5.4) 5 (4.5) 4 (3.6) 8 (7.2) .80Data presented as n (%); P values are based on χ2 test.
Abbreviations: ALI, acute lung injury; ARDS, acute respiratory distress syndrome.
Data presented as n (%); P values are based on χ2 test.
Abbreviations: ALI, acute lung injury; ARDS, acute respiratory distress syndrome.
P values based on generalized linear mixed model that accounts for ISS, the type of injury, and shock index as fixed effect, as well as study site as a random effect.
Abbreviations: ALI, acute lung injury; ARDS, acute respiratory distress syndrome; CI, confidence interval; ISS, injury severity score; OR, odds ratio.
Survival benefit for subjects receiving any opioid persisted for all 3 time periods after adjusted analysis with the linear mixed model (all odds ratios [ORs], 0.01–0.06; [confidence interval , 0.004–0.13], all P < .001) (Table 4).
MorbidityIn unadjusted univariable analysis, there were differences in the incidence of SIRS across all opioid groups (P < .001) with lowest incidence in the no opioid group (Table 2). This signal persisted after adjusted analysis (all ORs, 5.18–6.11 [CIs, 2.45–13.43]; all P < .001) (Table 4). However, after sensitivity analysis with subjects remaining alive at 24 hours, difference in SIRS disappeared (Table 3) and remained absent in adjusted analysis of those alive at 24 hours (Table 5).
Table 5. - Adjusted Associations of Opioid Dose With Morbidity as the Secondary Outcomes in Patients Who Survived the First 24 Hours Dose quartile 1 vs 0 Dose quartile 2 vs 0 Dose quartile 3 vs 0 Dose quartile 4 vs 0 Secondary outcomes OR (95% CI) P value OR (95% CI) P value OR (95% CI) P value OR (95% CI) P value Lung complications (ALI or ARDS) 0.58 (0.23–1.44) .24 0.73 (0.29–1.88) .52 0.33 (0.12–0.90) .03 0.47 (0.17–1.34) .16 Systemic inflammatory response syndrome 1.13 (0.41–3.15) .81 1.12 (0.40–3.12) .83 1.46 (0.51–4.22) .48 1.35 (0.42–4.29) .61 Acute kidney injury 0.44 (0.19–1.02) .06 0.54 (0.23–1.26) .15 0.52 (0.22–1.23) .14 0.59 (0.24–1.47) .26 Ventilator-associated pneumonia 0.99 (0.41–2.40) .99 0.61 (0.24–1.57) .30 0.80 (0.32–2.02) .64 1.01 (0.38–2.71) .98P values based on generalized linear mixed model that accounts for ISS, the type of injury, and shock index as fixed effect, as well as study site as a random effect.
Abbreviations: ALI, acute lung injury; ARDS, acute respiratory distress syndrome; CI, confidence interval; ISS, injury severity score; OR, odds ratio.
There were no consistent differences in other secondary outcomes in univariable analysis. After sensitivity analysis with subjects remaining alive at 24 hours, there were differences in the incidence of lung complications (P = .02) and VAP (P = .03), with a higher incidence in the no opioid group (Table 3). In the adjusted model, VAP incidence remained higher in the no opioid group only compared to the lowest opioid dose group (OR, 2.52 [CI, 1.15–5.52]; P = .02) (Table 4), but there was no increased incidence in VAP for those surviving 24 hours. In adjusted analysis of those surviving 24 hours, there was a lower incidence of pulmonary complications only in opioid dose quartile 3 compared to no opioid (OR, 0.33 [CI, 0.12–0.90]; P = .03) (Table 5).
MOF analysis was limited due to the small number of site observations. Nonetheless, there was no association between opioid dose and MOF after adjusting for all other covariates (all P ≥ .43, results not shown).
Despite unequal enrollment across the 11 study sites, a site effect was not identified in the mixed-effect regression models.
DISCUSSIONIntraoperative opioid use in the severely injured trauma patient population has not been as widely studied as in elective procedures, and putative benefits have not been proven. Historically, recommendations for acute trauma patients have primarily focused on postoperative treatment for analgesia and sedation.4,10 In the current study, after adjusting for age, sex, injury severity, race, ethnicity, study site, and PROPPR treatment arm, administration of any opioid was associated with lower mortality in severely injured trauma patients compared to no opioids. This effect was present over broad opioid dose ranges with no differences between opioid dose groups. The opioid dose groups were clinically relevant and discriminated sequentially between low (<5 MME/h) and high (>16 MME/h) doses. For secondary outcomes, univariable and adjusted analysis association with a higher incidence of SIRS in any opioid dose group disappeared in univariable and adjusted analysis of those surviving >24 hours, and there was no consistent association found for other secondary outcomes.
Reduction of anesthetic and analgesic dose is a technique to help maintain hemodynamic stability in a severely injured trauma patient requiring resuscitation, while opioid reduction techniques are considered a current standard in elective surgical procedures.11 Thus, our finding of a potential survival benefit associated with opioid administration is intriguing and supports the clinical intuition of experienced trauma anesthesiologists. In some trauma centers, anesthesiologists begin opioid titration once hemodynamic stability is achieved and surgical hemostasis obtained.12 Fentanyl and morphine have been shown to potentially dilate the microcirculation, thereby facilitating blood flow in vasoconstricted vascular beds13,14 which supports the higher opioid doses used at some trauma centers. This requires further study given the complex changes in vascular tone after injury, during resuscitation and vasopressor use.3 The outcomes reported in this study suggest that future controlled clinical trials are necessary to study the potential physiological mechanisms and clinical outcomes.
The PROPPR database is one of the largest, most comprehensive controlled trials performed for adults with severe trauma and included prospectively collected anesthesia data. Thus, a strength of this secondary analysis is the sample size, allowing for adjustments for potential confounders, although a priori power analysis was not based on opioid administration. Study sites were established, experienced level-1 trauma centers in the United States, and represent contemporary anesthetic strategies for acute trauma patients.
Given that opioid dose was not a randomized intervention and was at the anesthesiologist’s discretion, reasons for using or limiting opioid administration could not be determined. Greater injury burden and hemodynamic instability are likely with a higher ISS,15 and a significant proportion who did not survive 24 hours did not receive any opioid. The higher ISS and shock index in the no-opioid group suggests that there was greater hemodynamic instability at the start of the anesthetic and was adjusted for in the fixed effects model. Additionally, details of preinjury opioid use (prescription or illicit substance abuse) and morbidity were not available, and prior use or abuse represents a potential confounder.
These findings suggest that opioid administration during initial anesthesia for acutely injured patients is associated with lower mortality, with no consistent effect on secondary morbidity after removal of nonsurvivors, and no signal of harm. However, there are several limitations of the study. This was a post hoc analysis, and since opioid dose was not randomized, the presence of potential confounding unmeasured variables cannot be excluded. Without prospective control of variables, the association of early, finite opioid administration on longer term outcomes remains descriptive and not causal. Secondly, 9% of the cohort were excluded from analysis due to missing data for opioid dose or study outcomes. We assumed that missing observations occurred at random. Third, our associated mortality findings were with wide 95% CIs in the adjusted model due to the small number of events in patients who received any opioid dose. We also acknowledge that we have not made any adjustment for multiple comparisons. Fourth, initial anesthetic care for patients in this cohort occurred over a relatively short time, with most cases lasting <4 hours. Although physiological stabilization during the index operation is a critical aspect of care for severely injured trauma patients, other factors may be associated with mortality, including intensive care, complications, comorbidities, and variables not measured in this study. Therefore, our findings should be cautiously interpreted and require replication in future prospective studies along with analysis of biochemical markers to elucidate mechanisms that may be associated with clinical outcomes.
Univariable and adjusted association of increased rate of SIRS in any opioid dose group may reflect survivor bias and longer time to develop a secondary complication. This is supported by the absence of any consistent inflammatory signal after sensitivity analysis with removal of subjects who died in the first 24 hours.
These findings in a secondary analysis of a large, prospective multi-institutional level 1 trauma study show an association of opioid administration during anesthesia for initial surgical or radiological intervention with decreased mortality. This supports the clinical practice of intentional opioid dosing in this cohort and serves as a foundation for future prospective examination.
DISCLOSURESName: Dominique T. Levy, BS.
Contribution: This author helped with data collection, preparation, and manuscript writing.
Conflicts of Interest: None.
Name: Colleen E. Livingston, BS.
Contribution: This author helped with data collection, preparation, and manuscript review.
Conflicts of Interest: None.
Name: Sepideh Saroukhani, MD, PhD.
Contribution: This author helped with data collection, preparation, and manuscript review.
Conflicts of Interest: None.
Name: Erin E. Fox, PhD.
Contribution: This author helped with data preparation and statistical analysis.
Conflicts of Interest: None.
Name: Charles E. Wade, PhD.
Contribution: This author helped with manuscript review.
Conflicts of Interest: None.
留言 (0)