
記住我









A single-center randomized controlled prospective clinical study was conducted for TLE. This study was approved by the ethics committee of the First Affiliated Hospital of the University of Science and Technology of China and registered on the Chinese Clinical Trial Registry (ChiCTR, http://www.chictr.org.cn) by Zhang Min (registration number, ChiCTR-2000033617). The study inclusion criteria were patients undergoing TLE. Each participant provided written informed consent before initiating any study-related procedures. Patients of either sex, with physical status of II–III on the American Society of Anesthesiologists classification, age ≥ 60 years, and with no history of mental illness, hearing and language disorders, volunteered to participate in the study and signed informed consent.
PatientsThe authors enrolled 80 patients in this prospective study, after patient selection using the inclusion and exclusion criteria, who were scheduled for elective TLE from May 2020 to May 2021. Patients were randomized to the nerve block group (group N) or the control group (group C) (n = 40 per group) using the sealed-envelope method. Exclusion criteria included the following: allergic history of local anesthetics, infection at the puncture site, coagulation dysfunction, patients with paresthesia dysfunction, refusal of nerve block by patients or family members, intraoperative blood loss greater than 600 mL, reoperation, or patients admitted to intensive care unit (ICU) after surgery.
Anesthesia ProcedurePatients were sent to the surgical room and received standard monitoring, which consisted of five-lead electrocardiography (ECG), oxygen saturation (SpO2), non-invasive blood pressure measurements, and bispectral index monitoring (BIS). Then we monitored the radial artery pressure by radial artery puncture under local anesthesia. Midazolam 0.02–0.04 mg/kg, etomidate 0.2–0.4 mg/kg, sufentanil 0.4–0.5 μg/kg, and rocuronium 0.6–1 mg/kg were given for anesthesia induction. Manual face mask ventilation was continued for no less than 3 min until the jaw relaxed and the value of BIS was less than 50, to allow endotracheal intubation. The appropriate type of endotracheal tube was inserted, an occluder was inserted, and the bronchoscopy was used to assess its correct placement. Then, the patients were connected to a mechanical ventilator and the SpO2 and end-tidal carbon dioxide pressure (PetCO2) were maintained in the normal range. Propofol, remifentanil, sufentanil, and cisatracurium were used to maintain the BIS value between 40 and 60 and to ensure that the mean arterial pressure (MAP) and heart rate (HR) variation did not exceed 20% from the baseline values in the two groups. The same surgical team, comprising three thoracic surgeons, performed all the surgeries.
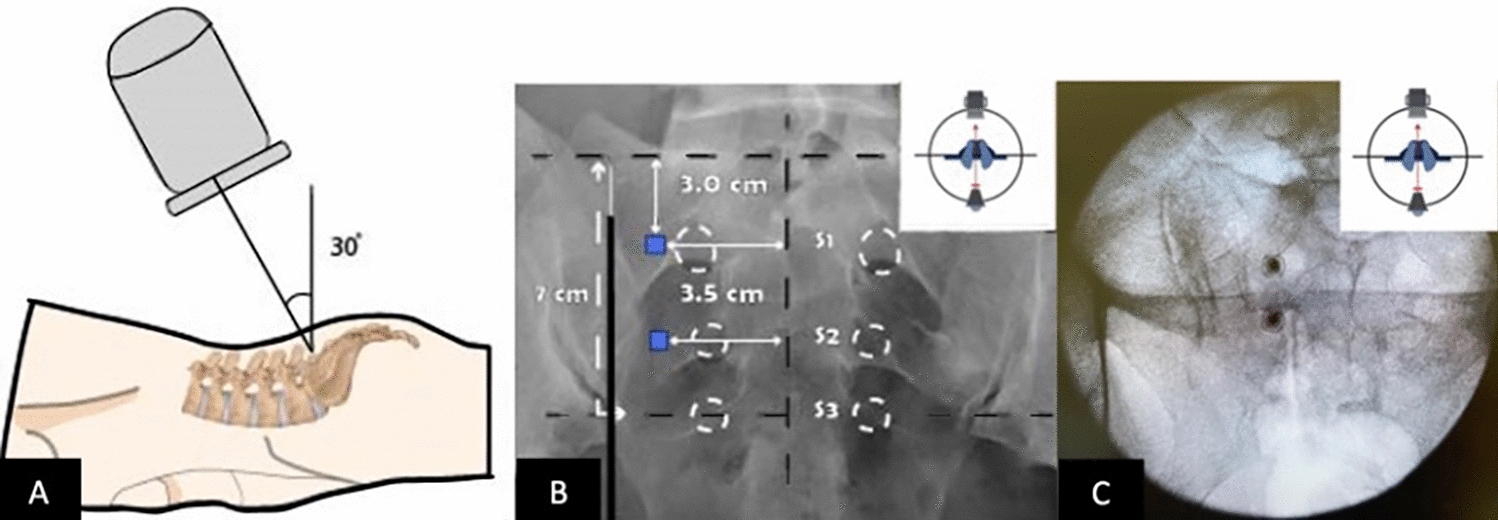
After induction of anesthesia, group N received an ultrasound-guided right SAP block. The ultrasound probe was placed at the level of the fourth and fifth rib of the right axillary midline [9]. SABP was given 20 mL of local anesthetics in the serratus anterior deep fascia space, including 0.375% ropivacaine plus 2.5 mg dexamethasone (Fig. 1A). Then, after the chest operation, the patient was transferred to the supine position to perform a bilateral TAP block before the abdominal operation. In this study, bilateral TAP blocks were performed by a subcostal approach, which targets the transversus abdominis plane compartment in the anterior abdominal wall [14]. Both sides received 20 mL of local anesthetics, including 0.375% ropivacaine plus 2.5 mg dexamethasone in the transverse abdominal fascia space (Fig. 1B). Group C did not accept the above two nerve block methods. The patients were transferred to the anesthesia recovery room (PACU) after the surgery and sent back to the ward when they were fully awake.
Fig. 1
Sonographic image of the serratus anterior plane block (A) and the subcostal transversus abdominis plane block (B). The asterisk indicates needle target. SA serratus anterior, RA rectus abdominis muscle, TA transversus abdominis muscle
After extubation, A PCA pump (ZZB-IB, Nantong AIPU Medical Inc., China) was connected to the intravenous line and administered the analgesic drugs (1-μg demand dose, 10-min lockout period without background infusion). A 150 mL solution was prepared in the PCA reservoir bag containing 1 μg/mL of sufentanil alone. When sufficiently awake, patients were instructed to assess their pain level on visual analog scale (VAS). If VAS scores > 4 in any patient, parecoxib 40 mg was immediately administered as rescue analgesia.
Observation IndexThe perioperative data and postoperative assessments were performed by the anesthesiologist who was blind to each patient’s group. All patients who were drowsy, on mechanical ventilation, and did not respond appropriately to oral commands were excluded from the study. The systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR) were recorded at baseline, 30 min, 60 min, and 2 h after the thoracoscopic incision. Blood glucose was recorded at baseline, 30 min, 60 min, and 2 h after the thoracoscopic incision. Intraoperative consumption of propofol, remifentanil, and cisatracurium, number of local anesthetic toxicity, the time of respiratory recovery, the first opening of eyes, extubation after the end of anesthesia, and time in PACU were recorded. The time to first rescue analgesic, the number of patients who required rescue analgesic, and the total postoperative use of sufentanil were also recorded within 48 h after returning to the ward. Postoperative VAS scores (0–10 points) at rest and cough at 2, 6, 12, 24, and 48 h were recorded after returning to the hospital. Adverse reactions that occurred 48 h after the surgery: postoperative nausea and vomiting (PONV), drowsiness, and chronic pain at 3 and 6 months were recorded.
Sample SizeThe purpose of the study was to test the hypothesis that the multipoint fascial plane block and total intravenous anesthesia would result in better postoperative control of pain compared with simple total intravenous anesthesia alone in elderly patients undergoing TLE. After a pilot study (5 patients per group), the authors detected a difference of 25% reduction in postoperative VAS scores. The authors estimated that the required sample size would be 40 patients per group with a significance level of 0.05 and a power of 90% [15]. Finally, 80 patients were then enrolled to allow for dropout.
Statistical AnalysisStatistical analyses were conducted using SPSS Statistics 22.0 software (SPSS, Inc., Chicago, IL, USA). Continuous (numerical) data were expressed as mean ± standard deviation (SD) with normally distributed data, or as the median and quartiles for skewed data distributions. Repeated measurements were used to analyze differences in the interaction effects between groups and timepoints. The Pearson chi-squared (χ2) test and Fisher’s exact test were used to analyze categorical variables. Confidence intervals (95% CI) are reported for the specific aims (VAS); P value < 0.05 was considered to indicate statistical significance.
留言 (0)