Since intestinal volvulus in utero with torsion of the dilated bowel in patients with ileal atresia is rare, surgical treatments and their outcomes are uncertain. Our patient was treated with emergency interventions, which preserved the growth and development of intestinal autonomy.
Intestinal volvulus in utero is reported as a rare neonatal surgical emergency [1, 5,6,7]. Prenatal diagnosis and sonographic findings include dilated bowel loops, the whirlpool, coffee bean, kinked loop signs, and polyhydramnios [2, 8]. The sensitivity and specificity of the whirlpool sign after birth are 45.4% and 99%, respectively [9]. Similarly, the specificity in utero may be high. In a literature review by Ohuoba et al., it was reported that of the fourteen in utero intestinal volvulus cases, nine were born by vaginal delivery and five by cesarean section, with all cases surviving [1]. However, the relationship between the length of the remaining intestinal tract and the delivery method is unclear. In the present case, despite the absence of severe distress during fetal monitoring, we elected to perform an emergency cesarean section due to fetal indication. Almost the entire small intestine was twisted around the axis of the dilated intestine. Our choice of delivery method might explain the good outcome for our patient.
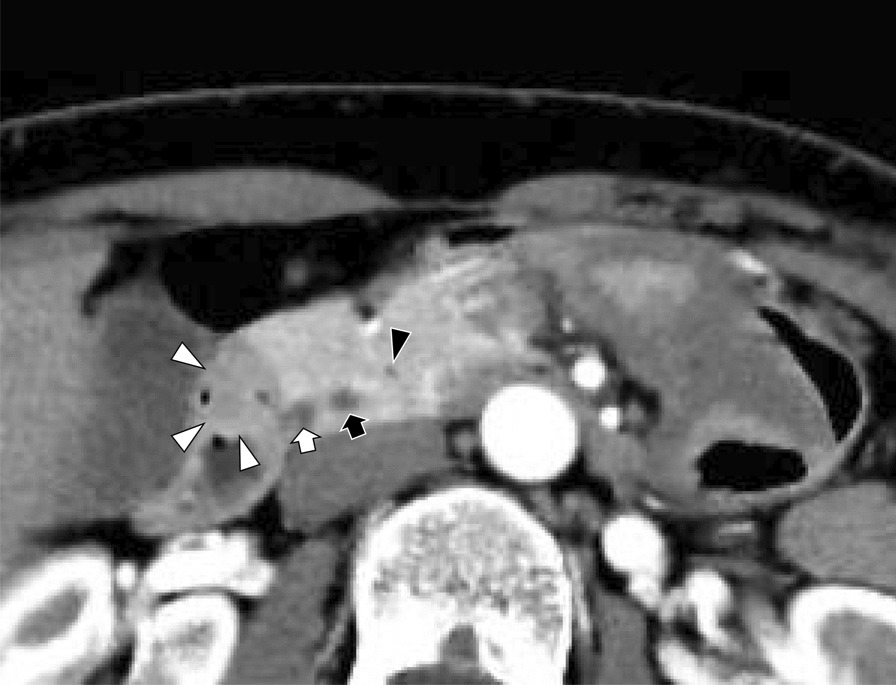
Midgut malrotation is the most common cause of intestinal volvulus in utero [5]. We found four cases of intestinal volvulus with intestinal atresia [1, 10,11,12]. Reported cases include intestinal atresia with volvulus, and meconium peritonitis and intestinal atresia with volvulus and intussusception [13]. The whirlpool sign was detected in two cases (50%). Unlike volvulus with malrotation, the whirlpool sign might be difficult to detect because the degree and mechanisms of torsion vary. In our case, we made a diagnosis with sufficient ultrasonographic evidence, which enabled us to treat the patient promptly.
Dilated bowel torsion in intestinal atresia after birth necessitates emergency surgery [3, 14], requires various technically challenging surgical techniques, and long-term outcomes should be considered. Thus, to prevent short bowel syndrome, it is essential to resect necrotic areas or malfunctioning bowel, and also plicate the intestine and evaluate the need for an ileostomy. The same principle applies in utero, and we believe emergency procedures should be mandatory protocol. We performed immediate laparotomy while being careful not to resect uncertain intestinal segments. Although the bowel was not entirely healthy, we performed intestinal anastomosis during the second-look surgery. It is difficult to preserve the ileocecal valve if an ileostomy is created. We believe immediate and appropriate interventions, such as intestinal autonomy without needing home parenteral nutrition, are crucial for a good prognosis.
A prenatal diagnosis of intestinal atresia, characterized by bowel distension, is common, and most cases are delivered electively. However, an emergency cesarean section might be required if an intestinal volvulus is present. Obstetricians, neonatologists, anesthesiologists, surgeons, and other physicians involved in perinatal care should be aware of this disease and be prepared for emergency intervention.









留言 (0)