
記住我
This study protocol is written in accordance with the SPIRIT guidelines [16, 17]. The SPIRIT checklist is provided in the Appendix I in the supplementary material.
Study designThe design of this trial is a national multicentre prospective interventional sequential cohort study including 43 participating centres (Appendix II in the supplementary material). Current local practice has been prospectively evaluated (and regarded/utilised as the first, control cohort) and subsequently compared to the intervention cohorts, after implementation of the optimal standardised surgical technique during a proctoring phase and then without intervening anymore in the consolidation phase (the second and third cohort respectively). A transition period is scheduled following the control cohort, in which consensus will be reached about the standardised MIRH using the Delphi method and education and hands-on training of the standardised technique is performed, before the technique will be implemented.
Study objectivesThe primary objective of this study is to safely implement a standardised technique of MIRH without increasing the 90-day postoperative complication rate, and to ultimately improve long-term outcomes for patients with right-sided colon cancer in the Netherlands. It is hypothesized that this will translate into a reduction of local and distant disease recurrence and thereby an improved 5-year overall survival (OS) and 3-year disease-free survival (DFS).
Secondary objectives are (1) to evaluate current national surgical variations of MIRH and their impact to clinical outcomes (already finished, namely phase 1); (2) to reach consensus concerning the standardised stepwise surgical technique for MIRH using the most recent insights from literature and guidelines and using the Delphi method (already finished) [18]; (3) to design and validate a CAT for the MIRH reflecting all the steps from the Delphi consensus; (4) to evaluate the effect of training and proctoring of the standardised MIRH (comparing control, implementation and consolidation cohorts) on surgical quality and (5) on short- and long-term clinical outcomes.
Ethical considerationThe trial will be conducted according to Good Clinical Practice guidelines and the principles of the declaration of Helsinki (2013, [19]) and in accordance with the Medical Research Involving Human Subjects Act (WMO) and other guidelines, regulations and acts. This study is approved by the Medical Ethical Committee (METC) of the Amsterdam UMC, location VUmc (2021.0273). The protocol is registered by ClinicalTrials.gov (NCT04889456).
Study populationEligibility criteria for study participation include (1) patients with planned laparoscopic or robot-assisted (extended) right hemicolectomy for colon cancer of the caecum, ascending colon, hepatic flexure or proximal transverse colon, (2) age above 18 years and (3) signed informed consent.
A patient will not be eligible for inclusion in case of the presence of one or more of the following exclusion criteria: (1) cT4b/multivisceral resection, (2) cTNM stage 4 (M1), (3) ASA 4, (4) immune-modulating medication, (5) prior midline or transverse laparotomy larger than 10 cm (not including Pfannenstiel and McBurney’s incision), (6) perforated disease/peritumoral abscess/fistula, (7) acute obstruction, (8) emergency surgery, (9) neuroendocrine neoplasm (NEN), (10) other primary malignancy treated within 5 years from diagnosis of colon cancer, except for curatively treated prostate, breast, skin and cervical cancer.
Informed consent procedureEligible patients will be approached for entry into the study at the first outpatient visit at the surgical department. The informed consent procedure includes study explanation, a written patient information sheet and adequate time for questions before signing the study consent form prior to the surgical procedure. Written informed consent is given by the patient to a participating surgeon, resident or research nurse at the outpatient clinic. Every included patient will be assigned a four-digit study number and only the local investigation sites have access to a decryption code.
Study outlineThis study consists of five phases as is schematically displayed in Fig. 1.
Fig. 1
Schematic of the five-step approach of the Right study
Phase 1: the variation of current surgical techniques amongst surgeons and centres for right-sided colon cancer was evaluated by prospective inclusion of consecutive patients into the control cohort. The first patient was included in October 2021, and currently all patients for this phase of the study have already been included. The preoperative CT imaging, full-length surgical video, pictures of the front and the back of the specimen and clinicopathological outcomes, as well as the CT imaging 1 year postoperatively (which is part of the routine oncological follow-up regimen in the Netherlands) were collected. The patients were treated according to the surgeon’s preference of surgical technique and local hospital perioperative care protocols. In this phase, anonymised video analysis of all the cases will be performed to evaluate variability and surgical quality.
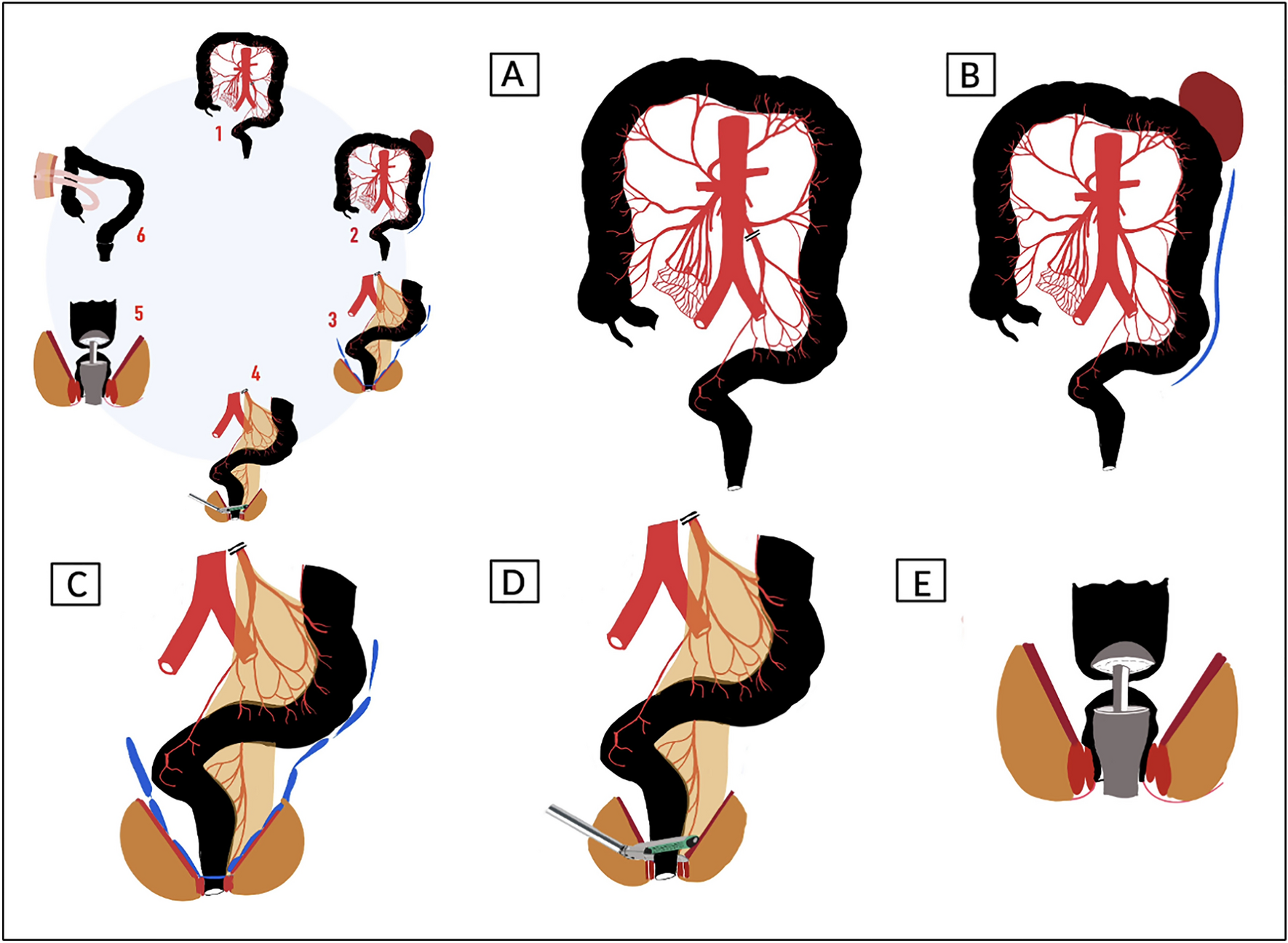
Phase 2: a Delphi method was applied with two colorectal surgeons from each participating institution (n = 43) after the inclusion period of the control cohort was closed, to establish a detailed standardised technique of MIRH for colon cancer. The consented standardised technique includes essential elements that could potentially improve outcomes such as setup, surgical approach, mesocolic plane dissection, level of vascular ligation with the extent of vertical lymphadenectomy, the technique of the anastomosis and the extraction site.
Phase 3: the consented standardised technique was taught to all participating colorectal surgeons (n = 86) during a 1-day hands-on surgical training course. The standardised MIRH was trained in several skills centres in the Netherlands. The same two surgeons from each participating centre who contributed in the second phase participated in this phase. The courses consisted of a theory session with several presentations about the best evidence, anatomy and the optimal standardised surgical technique, followed by a hands-on training on human cadavers in the afternoon to apply and practise the technique. All proctors of the Right study first participated in a teach the teacher MIRH CME training in the presence of ESCP faculty before training the participating surgeons.
Phase 4: the new standardised MIRH technique will be implemented in a controlled fashion by proctoring the surgeons of the participating centres. The same two surgeons who were trained during phase 3 will consecutively include all eligible patients. This phase is referred to as the implementation phase and, similar to the control cohort, the preoperative CT imaging, full-length surgical videos, pictures of the front and the back of the specimen and clinicopathological outcomes as well as the CT imaging 1 year postoperatively will be collected. A total of 11 proctors throughout the Netherlands are selected on the basis of their experience in performing MIRH and in proctoring as well. They will be physically present within the operating room the first time the standardised technique is applied, after which teleproctoring will be used for the following sessions. Teleproctoring entails monitoring of the procedure by the proctor from a distance with the means of immediate communication between proctor and surgeon. After each proctor session, an evaluation (global assessment score, GAS) form will be completed in which the surgical procedure itself will be assessed on certain points and the specimen quality is rated. In addition, on that GAS form, both the proctor and the surgeon will each decide on the necessity to proctor/be proctored again. In phase 4, prospective anonymised video analysis of all the cases will be included with feedback to participating surgeons to stimulate the learning curve and to evaluate surgical quality.
Phase 5, the final phase: a third consecutive group of patients will be included to observe consolidation of the standardised technique after the learning curve without proctoring (consolidation phase). Again, the same preoperative CT imaging, full-length surgical videos, pictures of the front and the back of the specimen and clinicopathological outcomes as well as the CT imaging 1 year postoperatively will be collected and analysed, in order to be able to compare the performance with the control cohort and implementation period. This phase will involve a prospective and anonymous video analysis of every case to assess the surgical quality.
OutcomesThe primary outcome of the current study is safety based on the overall 90-day postoperative morbidity rate, analysed and classified according to Clavien–Dindo [20]. Secondary outcomes include (1) intraoperative complications (i.e. vascular injury, injury to other organs), (2) 90-day mortality, (3) conversion rate, (4) operative time (minutes), (5) blood loss (millilitres), (6) validated assessment of the whole procedure using a CAT, (7) grading of the resection specimen according to Benz et al. [21], (8) total lymph node count in the specimen by the pathologist, (9) number of resected tumour-positive lymph nodes, (10) resection margins, (11) completeness of mesocolic excision based on the postoperative CT imaging (as performed 1 year postoperatively in regular oncological follow-up), (12) frequency of locoregional recurrence, (13) occurrence of distant metastasis, (14) 3-year DFS, (15) 5-year OS and (16) long-term surgical morbidity such as incisional hernia and adhesion-related small bowel obstruction.
Sample size calculationThe sample size calculation is based on safety with non-inferiority for the primary endpoint, the overall 90-day morbidity. In the Dutch national colon cancer audit, the overall postoperative complication rate after MIRH was 26% [22]. As all contributing hospitals within this study are represented in the national database, it can be assumed that the control cohort of the Right study has the same percentage of postoperative complications, i.e. 26%. A non-inferiority margin of 7% was defined. Therefore, introducing the new standardised technique will still be considered safe if the overall postoperative complication rate does not exceed 33%. A total of 1095 patients (365 patient in each of the three prospective cohorts) will be needed to show that there is no difference between the control and experimental (i.e. standardised surgical technique) treatment. With this number of included patients, it can be demonstrated with 80% certainty that the lower limit of the one-sided 95% confidence interval (or equivalently a 90% two-sided confidence interval) will be above the non-inferiority limit of 7%.
Statistical analysisBaseline patient and procedure characteristics and perioperative outcome parameters are categorical, continuous and dichotomous variables, and will be presented accordingly. The chi-square test will be used to compare dichotomous and categorical data among patient groups. Descriptive outcomes will be reported as median with interquartile range (IQR) or mean with standard deviation (SD). According to their distribution, the Mann–Whitney U test will be used to evaluate intergroup variation.
Oncological outcomes will be determined using Kaplan–Meier analyses, with comparison of relevant patient groups using the log-rank test. Predictors of main outcome parameters will be determined by selecting relevant variables based on expected association with subsequent univariate analysis. Alongside the stratified comparisons as described above, multivariate analysis will be performed to determine the independent association of factors with a specific outcome parameter using logistic and Cox regression analyses. A p value of less than 0.05 will be considered to be statistically significant. All analyses will be performed with IBM SPSS statistics, version 23.00 (IBM Corp Amonk, NY, USA). Design of the CAT will be assessed to test reliability using generalizability theory. The outcome parameters of the CAT will be compared with clinical outcomes using univariate analysis and multivariate analysis to determine the independent association of factors with a specific outcome parameter using logistic and Cox regression analyses.
Before data is locked for analysis, the statistical analysis plan will be completed, and decisions will be made on stratification criteria, planned subgroup analysis, and how to handle baseline imbalance.
Safety reportingOwing to implementation of established surgical techniques within a controlled setting, the Right study is considered a low-risk study. As the patients in the control cohort will receive the standard of care, serious adverse events (SAEs) will not be reported. For the implementation and consolidation phases, SAEs will be documented up to 90 days following the operation.
The sponsor will immediately suspend the study if it is suspected, on the basis of sufficient signals, that continuation will jeopardise the health and/or safety of the subjects. The sponsor will notify the accredited METC without undue delay of a temporary halt including its reason. The study will be suspended pending a further positive decision by the accredited METC prior to continuation. The investigator will guarantee that all subjects are informed.
Data handling and monitoringEvery included patient has been and will be assigned a four-digit study number. Communication occurs only with this number. The full name and date of birth of the patient have only been and will only be recorded on the informed consent form and these will be kept in a secure place in the participating hospitals, which is only accessible to anyone being officially involved in the Right study in that particular hospital.
In all participating hospitals, one of the surgeons acts as local principal investigator who is primarily responsible for execution of study interventions and for accuracy and completeness of the case report form (CRF). Data has been and will be digitally collected and stored using the electronic data management system Alea (https://www.aleaclinical.eu/). The digital platform has been specifically built for the purpose of the study by FormsVision, a privately owned business, which delivers clinical information technology solutions. This digital platform enables storage of full-length videos of surgical procedures, pictures of the specimen and CT imaging, and data entry for clinicopathological variables with all safety requirements concerning the privacy regulations. The design allows for secure worldwide online access to upload unlimited data 10 GB+ full-length videos and automatic consignments to reviewers by email with the ability to blindly assess the quality of surgery with a reviewer account.
Public disclosure and publication policyThe Right study was registered at ClinicalTrials.gov (NCT04889456). Patients are entitled to public disclosure of the results of the study on the basis of their participation in it. The results of the study will be submitted for publication to peer-reviewed scientific journals regardless of the study outcomes, presented at international conferences and disseminated to relevant surgical and oncological associations. Participation agreements with respect to publication were completed prior to the start of the study. Authorship will be granted to all participants of the study group, and every other subject who made a substantial contribution to this study will be added to the collaborator list.
留言 (0)