
記住我

A previously healthy 34-year-old man presented with progressive neurological symptoms of gait and speech difficulties, and blurred vision within 2 weeks of a mild viral prodrome. He had close contact with a COVID-19-infected family member. On admission, he was alert and oriented. Neurological examination revealed direction-changed nystagmus, and gait and bilateral limb ataxia, accompanied with dysarthria and increased deep tendon reflexes but no sensory deficits. Chest CT scan was normal. Brain MRI showed bilateral non-enhancing confluent T2/FLAIR hyperintensities in the periventricular white matter and corticospinal tracts (Fig. 1A–C). Cerebrospinal fluid (CSF) analysis revealed 1/µL leukocytes, 6 erythrocytes/µL, protein 73 mg/dL, glucose 67 mg/dL, IgG 172.1 mg/dL, and CSF IgG index of 1.18. Using Neuro 9 multiplex real-time PCR, cytomegalovirus (CMV), adenovirus, herpes virus (HSV) 1 and 2, varicella zoster virus (VZV), enterovirus, parechovirus, human herpes virus (HHV) 6 and 7, and parvovirus B19 were negative in the CSF but Epstein–Barr virus (EBV) DNA came back positive. SARS-CoV-2 RNA was also detected in the CSF using TaqMan probe–based real-time, reverse transcription PCR. During the following weeks, the patient developed multiple cranial nerve palsies (bilateral cranial nerve (CN) VI and left CNs VII, IX, and X), aphasia, and spastic paraparesis with increased deep tendon reflexes in all four limbs. Intravenous immunoglobulin (IVIG) and high-dose steroids led to partial recovery of deficits but symptoms recurred after a few days. Given that the patient had progressive neurological signs and another positive test result for CSF EBV DNA PCR, he was started on a 14-day course of ganciclovir. Four-week follow-up brain MRI showed significant decrease in the aforementioned T2/FLAIR white matter lesions (Fig. 1D–F). The patient was discharged to rehabilitation service for treatment of the remaining neurological sequelae including dysarthria, spastic paraparesis, and urinary incontinence. Four-month follow-up showed significant improvement of the cognitive and motor skills with neurorehabilitation (Table 1).
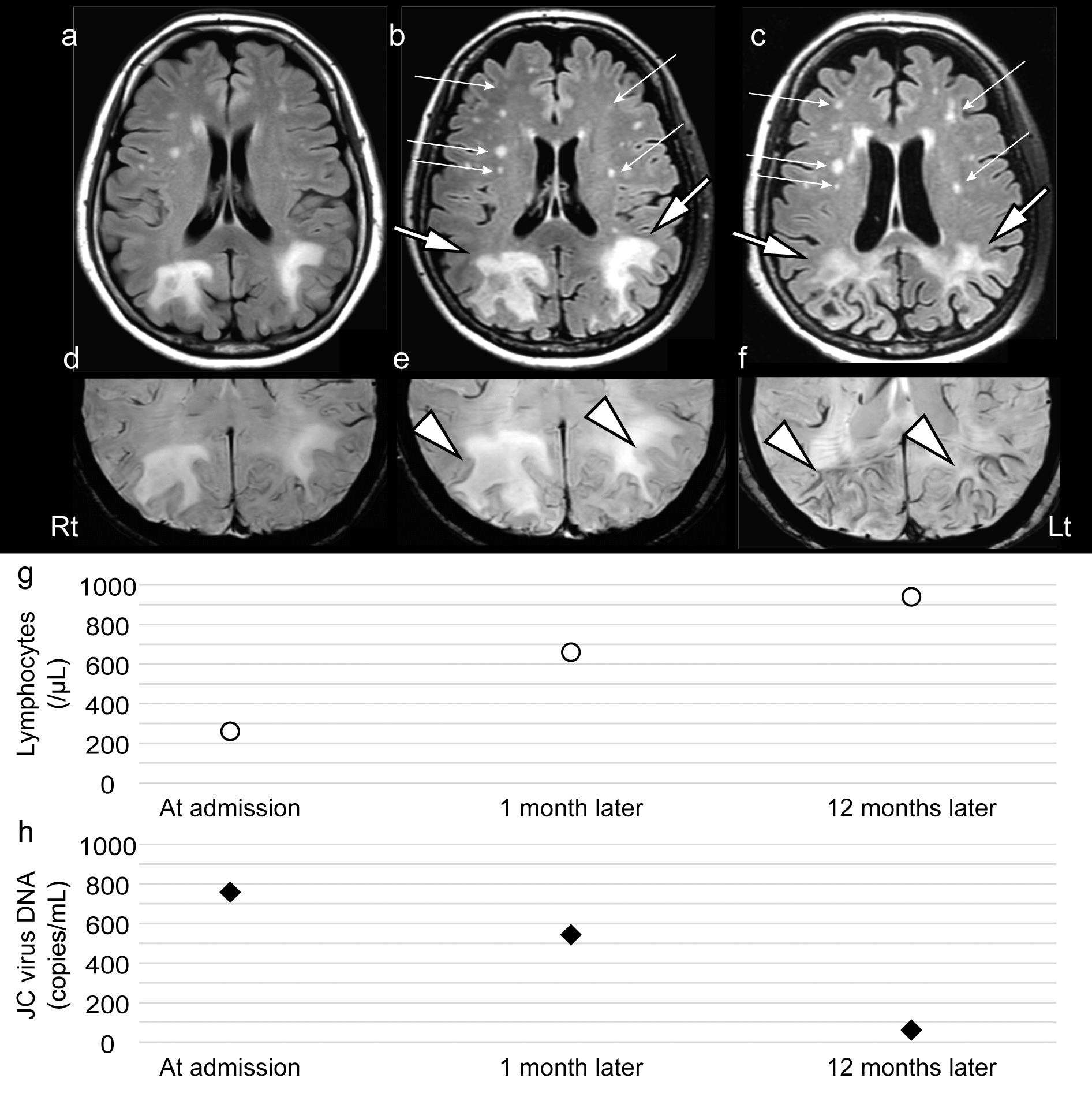
Fig. 1
On admission, brain MRI of patient no. 1 (A–C). FLAIR (A), T2W (B), and T1W with contrast (C) sequences show confluent high signal intensities in the deep white matter of periventricular and corticospinal tracts bilaterally. No evidence of enhancement is seen. Four-week follow-up brain MRI of patient no. 1 (D–F). T2W/FLAIR signal hyperintensities are decreased significantly in the deep white matter of periventricular and corticospinal tracts (A, B) and no enhancement in T1W post contrast (C). Spine MRI of patient no. 2 (G–J). Sagittal T2W (A), STIR (B), T1W post contrast (C), and axial T2W (D) images showed a long segment (C2-T9) central cord hyperintensity on T2/STIR images with no contrast enhancement. Chest CT scan and brain MRI of patient no. 3 (K–L). Chest CT scan shows consolidation in the right lower lobe (red asterisk) with peribronchial thickening (A) and brain MRI shows high signal sulci (red arrow) in the frontoparietal region on axial FLAIR image (B)
Table 1 Patients’ characteristicsCase 2A 19-year-old married woman presented to the emergency department with confusion and fever. Her symptoms started 2 days after her child recovered from a transient episode of fever, myalgia, and symptoms suggestive of gingivostomatitis. Subsequently, she developed fever, sore throat, myalgia, and a few oral ulcers. After 2 days, she noticed weakness in both her legs, numbness up to above the umbilicus, and difficulty in urination. Three days later, she was admitted to the hospital with lethargy and fever. She had a history of paraparesis, with a sensory level, and urinary retention 1 year prior current symptoms that resolved spontaneously after 1 week, before seeking medical attention. On admission, she was febrile and lethargic and had neck stiffness. Neurological examination revealed flaccid paraplegia, bilateral neutral plantar responses, and a sensory level at T6. Chest CT scan was normal. Her brain MRI was unremarkable but spine MRI showed a long segment (C2-T9) non-enhancing central cord hyperintensity on T2/STIR (Fig. 1G–J). CSF analysis revealed leucocytes: 7/µL, erythrocytes: 17,000/µL, protein: 71 mg/dL, and glucose: 50 mg/dL. CSF PCR for CMV and VZV (AmpliSens®, Russia) and SARS-CoV-2 (TaqMan Real-Time PCR Kit for N and RdRp genes) were negative but positive for HSV-1 DNA (AmpliSens®, Russia). SARS-CoV-2 DNA PCR on nasopharyngeal specimen using TaqMan Real-Time PCR Kit for N and RdRp genes also revealed positive results. CSF anti-MOG, CSF anti-AQP4, and ANA profile were negative. Her consciousness returned to normal on day 4 of hospitalization while she was on empirical ceftriaxone, vancomycin, and dexamethasone for a presumed bacterial meningoencephalitis. During the second week of hospitalization, she received high doses of steroids presuming recurrent idiopathic transverse myelitis, before CSF HSV-1 DNA PCR reported positive. Limb motor forces continued to improve on IV Acyclovir which was added to the high-dose steroid in the third week. One-month follow-up showed full recovery of memory and cognitive skills.
Case 3A 54-year-old man presented to the emergency department with fever and behavioral change. Two weeks prior to admission, he developed fever, cough, and myalgia. SARS-CoV-2 RNA PCR on nasopharyngeal secretions using TaqMan Real-Time PCR Kit for N and RdRp genes showed positive results and he was diagnosed with COVID-19. One week later, he started experiencing headache, delusions, and hallucinations as well as fever. On physical exam, he was febrile, awake but agitated, inattentive, and disoriented. Motor system examination was normal and no focal neurological deficit was evident. CSF analysis was significant for leukocyte 580 cells/µL, 95% lymphocytes, 5% polymorphonuclears, protein 139 mg/dL, and glucose 41 mg/dL. Other laboratory examinations showed serum interleukin-6 134 pg/mL, CRP 16 mg/dL, ESR 24, procalcitonin 1.7 ng/mL, WBC 12,400/µL, polymorphonuclears 88%, lymphocytes 9%, Hb 11.9 mg/dL, platelets 211,000/µL, AST 30 U/L, ALT 34 U/L, and LDH 1019 U/L. Brain MRI showed high signal sulci in the frontoparietal region on T2/FLAIR images. HSV-1 DNA PCR on CSF using a commercial HSV 1 and 2 real-time PCR kit (®Novingene, Iran) was positive but SARS-CoV-2 RNA PCR using TaqMan Real-Time PCR Kit for N and RdRp genes and M. tuberculosis complex DNA PCR using AmpliSens® MTC-diff-FRT PCR kit revealed negative results. Since the result of HSV-1 DNA PCR on CSF found positive, CSF was not tested for other viruses. CSF culture was negative for bacterial and fungal pathogens. SARS-CoV-2 RNA PCR on nasopharyngeal secretions was repeatedly positive. The chest CT scan on admission revealed consolidation in superior segments of bilateral lower lobes suggestive of an aspiration pneumonia instead of pneumonia caused by SARS-CoV-2. He received intravenous acyclovir, ceftriaxone, and dexamethasone. During admission, he developed respiratory distress and underwent mechanical ventilation. At that time, the chest radiography showed progression of pulmonary infiltrates to bilateral airspace lesions on middle and lower lung zones. Intravenous piperacillin-tazobactam and remdesivir were started and ceftriaxone discontinued. Multidrug-resistant Klebsiella pneumoniae was isolated from respiratory secretions. Over the following days, his admission was complicated with multiorgan dysfunction eventually leading to death on the 14th day of hospitalization.
Case 4The last case was a 24-year-old 37-week pregnant woman who presented with fever, behavioral change, and unintelligible speech 1 week after a febrile prodrome. On admission, she was febrile (38 °C) and tachypneic (20/min) with oxygen saturation of 92% in room air. On neurological examination, she was confused and agitated with a Glasgow coma scale (GCS) score of 10/15. Laboratory examinations revealed white blood cell count of 6600/µL (neutrophils, 77% and lymphocytes, 16%), hemoglobin of 15.4 mg/dL, platelets of 304,000/µL, ALT of 228 U/L, AST of 532 U/L, ALP of 471 U/L, LDH of 1187 U/L, d-dimer of 3530 ng/mL, CRP of 41 mg/L, and ESR of 43 mm. Serum and urine toxicology screen were negative. Chest CT scan showed diffuse bilateral peripheral ground glass opacities involving about 30% of the lungs. Since the pattern of involvement on chest images was classic for COVID-19 and SARS-CoV-2 was detected on nasopharyngeal secretions using real-time RT PCR for N and RdRp genes, no test was performed for other respiratory viral pathogens on her respiratory secretions. She underwent an emergency cesarean section under general anesthesia due to the development of fetal distress and delivered a healthy baby. Brain MRI was normal and CSF analysis was unremarkable. CSF was negative for VZV, EBV, CMV DNA, and SARS-CoV-2 RNA but positive for HSV-1 DNA (AmpliSens®, Russia). She received intravenous acyclovir and steroids. On the 14th day of hospitalization, she was fully conscious but had some recent memory difficulties. Five-month follow-up showed full recovery of neurologic symptoms without any sequelae.
留言 (0)