
記住我


Chronic hepatitis leads to cirrhosis and liver cancer, which are the final stages of the liver disease process. Hepatitis B virus (HBV) infection is one of the most common causes of chronic viral hepatitis, especially in developing countries. It was reported that HBV infection alters the expression profiles of BA metabolism genes [7], suggesting that HBV infection alters BA metabolism. Comparison of the BA profiles of CHB patients and healthy controls (HCs) using liquid chromatography tandem mass spectrometry (LC‒MS/MS) revealed that CHB patients have significantly higher serum levels of conjugated Bas, including taurocholic acid (TCA), taurodeoxycholic acid, glycocholic acid, glycochenodeoxycholic acid, and glycodeoxycholic acid, than HCs, but there is not a significant difference in unconjugated BA levels [4]. Among conjugated BAs, TCA is the most increased in CHB patients compared with HCs [4]. In these patients, TCA upregulates the expression of programmed death-1 (PD1) in CD8+ T cells and downregulates the expression of NKG2D in natural killer (NK) cells, impairing the effector functions of CD8+ T and NK cells, which in turn promotes HBV replication [4]. Furthermore, serum BAs, particularly TCA, inhibit the response of CHB patients to interferon-alpha therapy by impairing CD8+ T-cell and NK cell functions [4]. It is worth noting that only one BA, ursodeoxycholic acid (UDCA), is detected at lower levels in CHB patients [4]. Recently, UDCA-mediated downregulation of angiotensin converting enzyme 2 by suppressing farnesoid X receptor (FXR) signaling was found to reduce susceptibility to SARS-CoV-2 infection in vitro, in vivo, and in human lungs and livers perfused ex situ [8]. FXR, a liver-enriched nuclear receptor that is also a known BA receptor, plays a pivotal role in the regulation of the HBV transcriptional program by binding to both EnhI and EnhII via the nuclear receptor-response element [9]. UDCA, an FXR antagonist [1], may inhibit HBV replication by suppressing FXR signaling. UDCA also exerts cytoprotective effects in hepatocytes, and treatment with UDCA can improve serum liver biochemistry [10]. These findings suggest that UDCA can inhibit HBV replication and improve liver function and may be a good treatment for CHB.
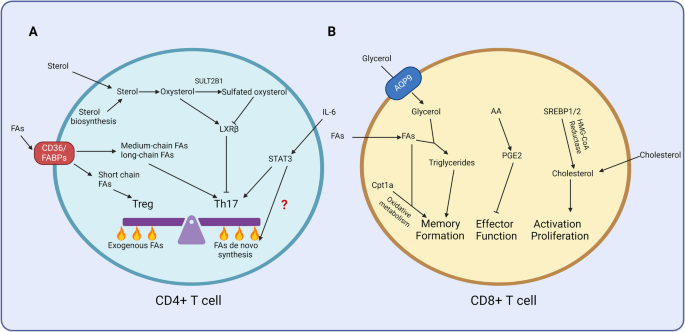
In summary, the abnormal accumulation of BAs, especially TCA, promotes HBV replication by impairing the effector functions of CD8+ T and NK cells in CHB patients (Fig. 1A). Using UDCA in combination with existing first-line drugs could be a promising clinical strategy for achieving a more desirable therapy endpoint for patients with CHB.
Fig. 1
A model illustrating the role of bile acids in chronic hepatitis B, liver cirrhosis, and hepatocellular carcinoma pathogenesis. A Abnormal accumulation of bile acids (BAs), especially taurocholic acid (TCA), promotes HBV replication by impairing CD8+ T and NK cell function in patients with chronic hepatitis B (CHB). B TCA-mediated activation of hepatic stellate cells (HSCs) promotes the progression of liver cirrhosis (LC). C Abnormal accumulation of BAs (including TCA) in hepatocytes skews macrophage polarization and induces an immunosuppressive tumor microenvironment favorable for hepatocarcinogenesis
留言 (0)