During the study period, the World Health Organization (WHO) declared an international emergency (23 July 2022) due to a rapid increase in the number of newly reported cases of MP. By August 2022, a total of 11,536 cases of MP had been diagnosed in Europe. Madrid was one of the most affected regions, with 1817 of the total of 4942 confirmed cases of MP reported in Spain by 1 August 2022.
This rapid increase in the number of newly reported cases over a short time period intensified public awareness and prompted the implementation of preventive measures, including vaccination for vulnerable populations. These measures likely played a role in slowing the spread of the MP outbreak. As a result, there was a progressive decrease in the number of MP cases, with a total of 7498 cases reported in Spain by 27 December. There have been no new cases reported in our center since October 2022.
Up to 95% of patients with MP are men [5, 6, 11]. While many of these men identify as MSM, MP transmission is not exclusive to this group and has also been reported in women and in men who have sex with women [12]. All patients with MP proctitis in our study reported practicing receptive anal sex prior to diagnosis and typically had genital or anal lesions that expand centrifugally [5, 7, 13].
In all suspected cases of MP, PCR testing of both skin lesions and rectal samples (when proctitis symptoms are present) is necessary for confirmation of the diagnosis. Upon initial contact with possible cases, healthcare workers should take precautions to prevent direct contact and transmission through respiratory droplets, such as wearing surgical masks and gloves [2, 9, 14,15,16]. A study by Nörz et al. found viral deoxyribonucleic acid (DNA) on surfaces in hospital rooms, as well as on linen and personal protective equipment (PPE) worn by healthcare workers after contact with an patient positive for MP. While the presence of the virus on these surfaces may not always lead to transmission, direct contact with mucosa, damaged skin, or high virus loads could result in the spread of the infection [16].
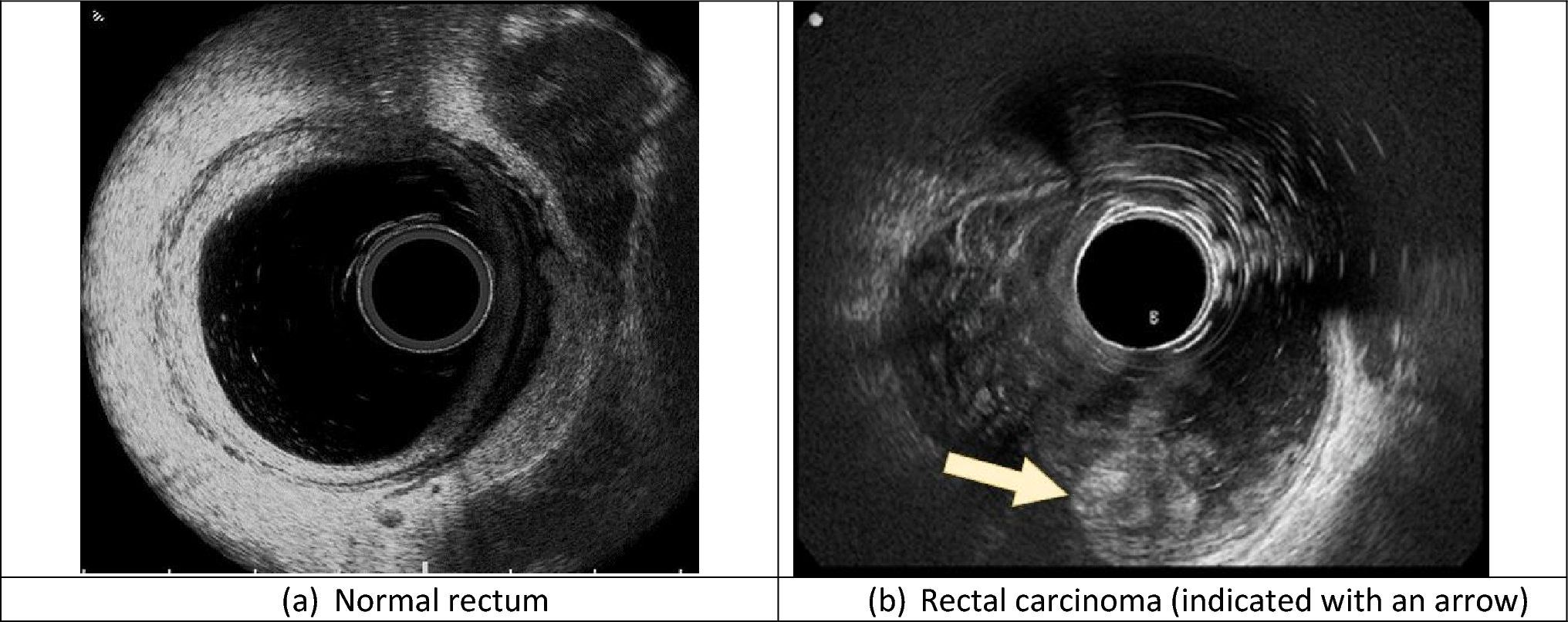
Proctitis has been reported in approximately 22–25% of patients with MP in previous studies, with common symptoms being rectal mucosal swelling and a mucopurulent discharge [5, 17]. A majority of patients also experience painful skin ulcers or papules around the anus [18]. In cases of proctitis where the patient has a history of receptive anal sex, it is important to test for and exclude MP and other STDs, as these infections may occur simultaneously and should be treated together. Other anorectal pathogens that can cause proctitis include Neisseria gonorrhoeae, Chlamydia trachomatis, Treponema pallidum, and herpes simplex virus, which are among the most common causes [8]. STDs such as chlamydia, lymphogranuloma venereum, and syphilis are typically associated with rectal symptoms including mucosal swelling, discharge that is mucopurulent and may be bloody, and ulcers in cases of infection with the latter two pathogens [8, 11]. These symptoms are similar to what was observed in MP proctitis cases without any additional STDs. Therefore, rectoscopy is not considered mandatory for diagnosis but it may provide useful information in cases of severe pain, and a general surgeon should be consulted to rule out the presence of an abscess.
One limitation of our study is that a patient who required surgery was not tested for MP or other STDs with rectal swab PCR and had rectal symptoms for 25 days after a diagnosis of MP was made, so abscess formation cannot be solely attributed to the presence of MP or other STDs. The severe swelling of the rectal mucosal and discharge seen during rectoscopy ruled out a typical cryptoglandular abscess. Another limitation was that we only obtained rectal PCR from those patients with proctitis and not from all MP cases; therefore, we cannot confirm that rectal samples are negative for virus detection in those patients without rectal symptoms. This mechanism could play a role in its transmission during early stages of the disease or in those patients with mild symptoms. PCR was always obtained from rectal/oral mucosa or skin blisters, but we cannot confirm that there were patients with mild skin lesions who required surgical drainage without being tested nor suspected for MP infection. Furthermore, all patients with proctitis are routinely tested for STDs (and MP virus since the beginning of the outbreak) during the first contact as previously described; therefore, it is unlikely that we missed proctitis cases without abscess, considering the range of days with rectal symptoms (range 1–25 days) before MP diagnosis.
Due to the severe rectal mucosa edema, physical exploration may wrongly suggest the presence of a rectal abscess. If rectal findings are inconclusive, CT scan is recommended. Severe circumferential anorectal mural thickening with hypoattenuated zones is the most common radiological finding, indicating mucosal edema and rectal ulcers [19]. As in the previously described rectoscopy findings, these must be accompanied by a compatible epidemiological context, typical skin lesions, and PCR study for diagnosis, since they are typical of proctitis due to either MP, STDs, or other causes such as radiation or ischemia [19].
If an abscess is diagnosed, surgical drainage should be made with the donning of full personal protective equipment to avoid contact with droplets [14, 15]. The surgical drainage and postoperative follow-up by the general surgeon is similar to treatment for a cryptoglandular abscess, with a consultation around 1 month after surgery. Internal medicine and dermatology departments continue follow-up, as was the case for all the patients with MP diagnosed in our center. Our patients were advised to seek medical assistance in our center if their condition worsened. Many patients had direct medical access through their HIV consultation, which may permit early diagnosis and limit disease spread, although it has been reported that patients with well-controlled HIV infections with an undetectable viral load and a high CD4 count are less likely to have a severe course [20]. In our study, we did not prescribe oral antibiotics after discharge and we did not have any readmissions or reoperations.
In observational studies, a cross-immunity for monkeypox infection using the smallpox vaccine has been described by the WHO, although most of the population under 40–50 years of age probably will not benefit from the protection provided by this vaccine applied during childhood [21]. On 12 July 2022, the Spanish Health Council recommended the administration of a single dose of IMVANEX in pre-exposure, high-risk populations (including patients with HIV with follow-up who are not previously vaccinated nor infected by smallpox). A dose of vaccine in the first 4 days post-exposure is recommended for immunocompromised patients, pregnant women, and children. This vaccination is also recommended for health personnel with direct MP exposure with patients or samples, and for direct contact with positive cases [22, 23]. Since our cohort was diagnosed and treated between 20 and 31 May 2022, vaccination was not generalized, and its protective effect against MP proctitis cannot be determined since we did not have any vaccinated patients in our proctitis cohort. A drastic decrease in the number of new MP cases may be attributed to the implementation of a vaccination campaign by the Health Ministry.
The current treatments for anal and rectal lesions include NSAIDs, prevention, and surveillance. Antivirals such as the VP37 assembly protein inhibitor tecovirimat have been registered by the European Medicine Agency for treating MP and cowpox since January 2022 [1, 2]. The oral drug brincidofovir (oral route) and its intravenous analog cidofovir inhibit the DNA polymerase [24, 25]. Both drugs have been shown to be effective against orthopoxvirus infections in vitro and in animal models, but with considerable toxicity [9]. Cidofovir may be most effective when administered early after MP exposure but it is also useful in diminishing MP manifestations in later stages of the infection.

留言 (0)