
記住我
The diagnosis of mucosal melanoma of the head and neck region (MM-H&N) is challenging due to the peculiar anatomic, histologic, and genetic features of these melanocytic tumors.1–6 MM-H&N are exceedingly rare and even experienced head and neck pathologists struggle to confidently diagnose this entity.1–6 Besides, in this site it is difficult to benefit from clinical-dermatoscopic correlation (as in the cutaneous counterpart), the samples are often poorly cellular incisional biopsies and/or highly fragmented samples, and some atypical histologic features (epidermal effacement and pagetoid spread of melanocytes in suprabasal layers) are rarely found in the early stage of disease.5,6 In recent years, several molecular tools, such as fluorescence in situ hybridization (FISH), comparative genomic hybridization, and next-generation sequencing have been implemented to aid in improving the diagnosis of melanocytic tumors.7–10 Unfortunately, the rarity of MM-H&N and the limited literature data on specific genetic mutations (as TERT promoter mutations) and molecular tests (FISH) distinguishing MM-H&N from benign mucosal melanocytic lesions of the head and neck region (MBML-H&N), limits their adoption in this diagnostic field.1–6,11–15 The recent introduction of PRAME (PReferentially expressed Antigen in MElanoma) has again shifted interest to using immunohistochemistry for the diagnosis of melanocytic lesions.16PRAME is a cancer-testis antigen isolated in 1997 from autologous T-lymphocytes and direct against the tumor in a patient with metastatic cutaneous melanoma.17 In recent years, PRAME was found to be expressed in normal and neoplastic tissues (mainly germ cell tumors of the testis, ovarian cancer, sarcomas, and hematologic tumors), with functions in oncogenesis, immune response evasion, apoptosis, acquisition of metastatic phenotype, and drug resistance.18–24PRAME became of great interest for the diagnosis of melanocytic tumors, as it proved to be expressed in melanomas but not in nevi, therefore an immunohistochemical marker of great help in one of the most challenging issues of surgical pathology.16,24–41 However, the majority of previous studies on PRAME did not enroll MM-H&N and the available data on the diagnostic value of PRAME are mainly on skin melanocytic tumors; a few studies only evaluated a limited number of MM-H&N.16,24–28,40–42 Toyama et al40 tested PRAME on a series of differently-sited mucosal melanomas (head and neck region, gastrointestinal, and genitourinary) and obtained promising results. Hovander et al41 confirmed these results on a small case series of oral cavity melanomas, and recently Scheurleer et al42 found PRAME expression in a cohort of sinonsal melanoma. The present study aims to test and validate PRAME stain as a reliable diagnostic tool in a retrospective case series of MM-H&N, comparing MM-H&N with MBML-H&N.
MATERIALS AND METHODS Case Series (Patients and Specimens) SelectionAll MM-H&N and MBML-H&N excised between 2004 and 2022 were retrieved from the database of 3 pathology units: Bellaria Hospital of Bologna (37 cases), Maggiore Hospital of Bologna (9 cases), and IRCCS Azienda Ospedaliero-Universitaria Policlinico di Sant’Orsola, Bologna (8 cases). The patients were selected according to the following inclusion criteria: (1) primary mucosal melanocytic lesion (each case was reviewed to verify its site and exclude metastases and cases more appropriately classifiable as cutaneous, especially for lips); (2) availability of formalin-fixed and paraffin-embedded samples with enough material to perform immunohistochemical analysis; (3) availability of clinical data. By contrast, cases judged as nonprimitive of the mucous membranes, and with no availability of formalin-fixed and paraffin-embedded samples for immunohistochemical analyses and/or clinical data were excluded. For each patient, the following clinical data were recorded: age at first diagnosis and sex. For each MM-H&N sample, the following pathologic features were recorded: type of histologic specimen (excision of the primary tumor, excision of residual tumor/relapse, incisional biopsy), site, histologic subtype, pigmentation, prevalent cytotype, ulceration, bone and/or cartilage infiltration, number of mitoses/mm2, lymphovascular invasion, perineural infiltration, and pT stage. For each MBML-H&N, only the following pathologic features were recorded: type of histologic specimen, site, and histologic diagnosis. All cases were reviewed and diagnosed according to the World Health Organization Blue Book on Classification of Head and Neck Tumours (fifth edition, 2022) by a panel of 4 pathologists with specific expertise in melanocytic pathology and/or head and neck pathology (C.R., B.C., T.B., and M.P.F.); all MM-H&N were staged according to the eighth edition of the American Joint Committee on Cancer (AJCC) Cancer Staging Manual.43,44
Immunohistochemistry and PRAME ScoringFor each case, a representative slide was selected, and from the corresponding paraffin-embedded tissue block one 3-μm-thick section was cut and stained with Melan A/PRAME (BenchMark ULTRA automated immunostainer; Ventana Medical Systems-Roche Diagnostics; Melan A: clone A103, PRAME: clone EPR20330) according to the previously described and published protocol.35,36 Cytoplasmatic Melan A stain was identified with the Red detection kit (red cytoplasmatic stain), whereas nuclear PRAME stain with the 3,3′-diaminobenzidine detection kit (brown nuclear stain).35,36 The double stain Melan A/PRAME was here adopted as it allows to better score PRAME in melanocytic cells and differentiate them from keratinocytes and the background of inflammatory cells.35,36 In MM-H&N with <76% of PRAME-positive cells (negative according to Lezcan et al16) an additional section was stained with single stain for PRAME to evaluate potential discrepancies with Melan A/PRAME.35,36 To identify the cutoff of PRAME-positive cells more suitable to discriminate MM-H&N and MBML-H&N, 3 different scores utilized in routine practice and/or proposed in the recent literature were tested: (1) score according to Lezcano et al16: 0=no expression, 1+=1% to 25%, 2+=26% to 50%, 3+=51% to 75%, 4+= ≥76%, with cases dichotomized in negative (0, 1+, 2+, 3+) and positive (4+); (2) score according to Raghavan et al30: 0=no expression—59%, 1+= ≥60%, with cases dichotomized in negative (0) and positive (1+); (3) score according to Santandrea et al34: adding the quartile of positive tumor cells (0, 1+, 2+, 3+, 4+ sec. Lezcano et al.) to PRAME expression intensity in tumor cells (0 [no expression], 1+ [weak], 2+ [moderate], 3+ [strong]), with cases dichotomized in negative (<5) and positive (≥5).
Statistical AnalysisFor each score sensitivity (SE), specificity (SP), positive predictive value (PPV), negative predictive value (NPV), and accuracy (AC) were evaluated. The score with the highest values of these parameters has been chosen to dichotomize the cases (low and high expression of PRAME) and analyze the association with the other dichotomous/categorical clinicopathologic features using the χ2 test. The statistical tests were performed using the IBM SPSS software, with a P-value <0.05 (2-sided) indicating statistical significance.
Ethical ApprovalThe study has been approved by the Review Board of the Area Vasta Emilia Centro-AVEC (protocol n. 03-2022-OSS-AUSLBO).
RESULTS Case Series (Patients and Specimens)A total of 54 histologic samples from 41 patients were collected. Samples consisted of 37 (68.5%) excisions of the primary tumor, 10 (18.5%) excisions of residual tumor/relapse, and 7 (8.5%) incisional biopsies. Twenty-five (61%) patients were females and 16 (39%) were males; the age at diagnosis ranged from 10 to 96 years (median value: 60 y). Clinicopathologic features of the case series are summarized in Tables 1 and 2. A graphical representation of MM-H&N and MBML-H&N sites is provided in Figure 1.
TABLE 1 - Clinicopathologic Features of the Case Series MM-H&N and MBML-H&N, n (%) MM-H&N, n (%) MBML-H&N, n (%) Patients (N=41) Patients (N=23) Patients (N=18) Clinical features Age, median value (range) 60 (10-96) 69.9 (29-96) 47.4 (10-79) Sex Male 16 (39) 9 (39.1) 7 (38.9) Female 25 (61) 14 (60.9) 11 (61.1) Histologic samples (N=54) Histologic samples (N=36) Histologic samples (N=18) Pathologic features Site Nasal cavity/nasal septum/turbinates 22 (40.7) 22 (61.1) 0 (0) Nasopharynx 2 (3.7) 2 (5.6) 0 (0) Palate (hard and soft) 12 (22.2) 6 (16.7) 6 (33.3) Maxillary sinus 4 (7.4) 4 (11) 0 (0) Tonsil 1 (1.9) 1 (2.8) 0 (0) Gum (upper and lower) 8 (14.8) 0 (0) 8 (44.4) Lip (upper and lower) 3 (5.6) 0 (0) 3 (16.7) Tongue 2 (3.7) 1 (2.8) 1 (5.6) Type of histologic specimen Excision of the primary tumor 37 (68.5) 24 (66.7) 13 (72.2) Excision of residual tumor/relapse 10 (18.5) 10 (27.8) 0 (0) Incisional biopsy 7 (13) 2 (5.5) 5 (27.8)MM-H&N: mucosal melanoma of the head and neck region; MBML-H&N: mucosal benign melanocytic lesions of the head andneck region.
Herein, we reported values for patients and samples because, for the cases of MM-H&N with multiple samples, a global (column: patients) and a single-sample (column: samples) assessment of the histologic features was performed.
LVI indicates lymphovascular invasion; PNI, perineural infiltration.
 FIGURE 1:
FIGURE 1: Graphical representation of MM-H&N (A) and MBML-H&N (B) in our case series.
MBML-H&N (Clinicopathologic Features and PRAME Expression)Eighteen histologic samples from 18 patients were collected: 13 (72.2%) excisions of the primary lesion and 5 (27.8%) incisional biopsies. Eleven (61.1%) patients were females and 7 (38.9%) males; the age at diagnosis ranged from 10 to 79 years (median value: 47.4 y). The most represented sites were gum (8, 44.4%) and palate (6, 33.3%). The cases were diagnosed as follows: 10 (55.6%) melanotic macules, 6 (33.3%) blue nevi, and 2 (11.1%) common nevi. All MBML-H&N resulted negative for nuclear PRAME expression according to the 3 tested scores. Thirteen (72.2%) cases were completely negative, 5 (27.8%) showed focal and weak immunoreactivity in a low percentage of cells (5% to 15%) with a random distribution and no intralesional intensity variation (defined as at least 2 adjacent high-power fields with >75% stain in a tumor with an overall uniform stain <75%) (Fig. 2).27
 FIGURE 2:
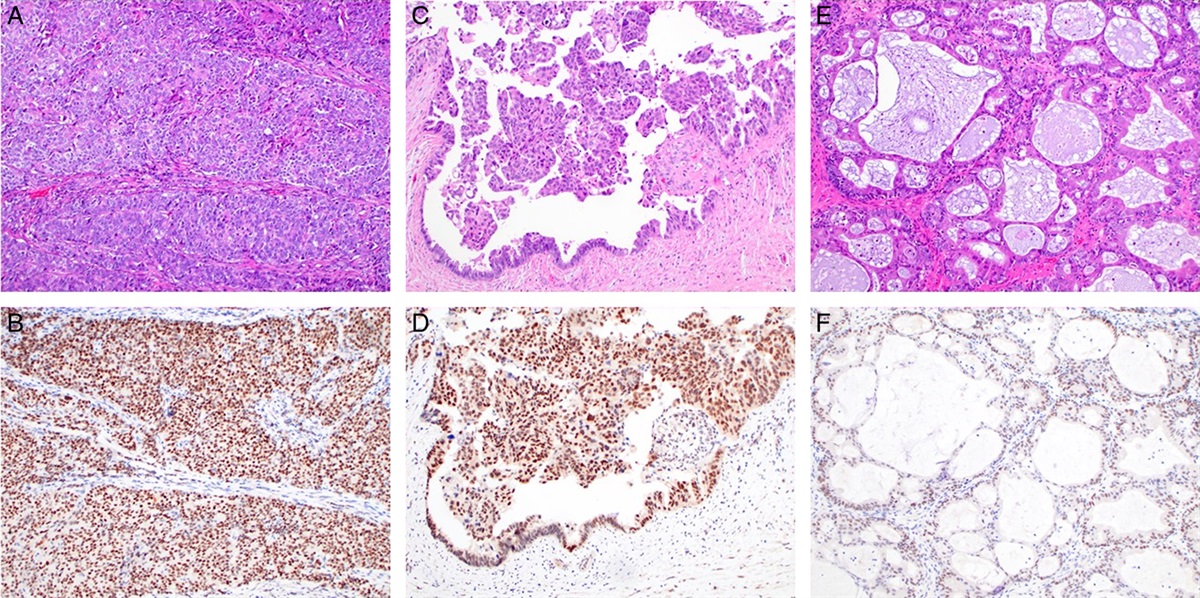
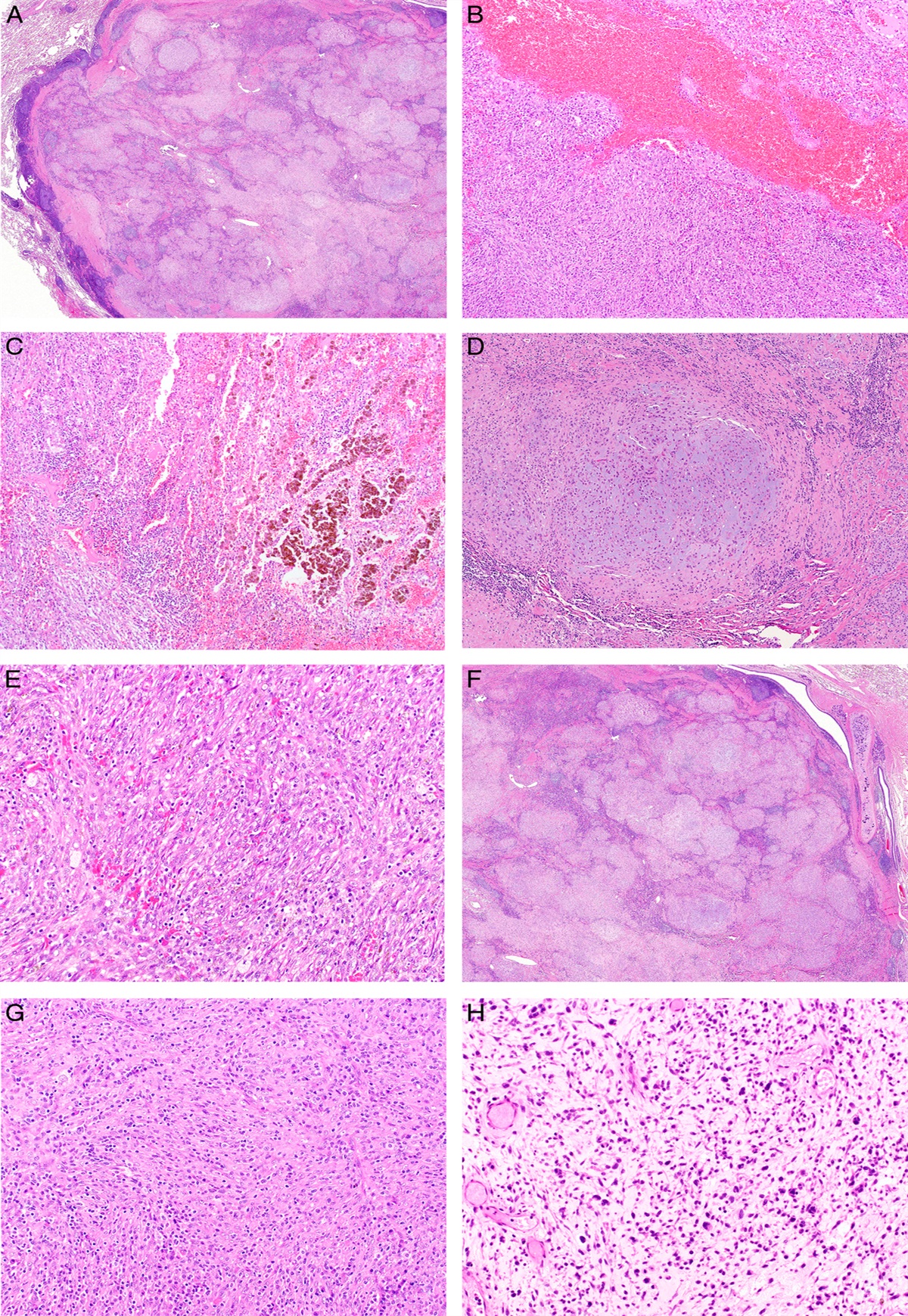
FIGURE 2: MBML-H&N: mucosal benign melanocytic lesions of the head and neck region; PRAME expression in MBML-H&N. Three cases of histologically straightforward MBML-H&N: common nevus (A: hematoxylin and eosin), melanotic macula (C: hematoxylin and eosin), and blue nevus (E: hematoxylin and eosin), respectively. Immunohistochemistry for Melan A/PRAME shows no or focal PRAME expression in the nuclei of melanocytes (B, D, F: PRAME).
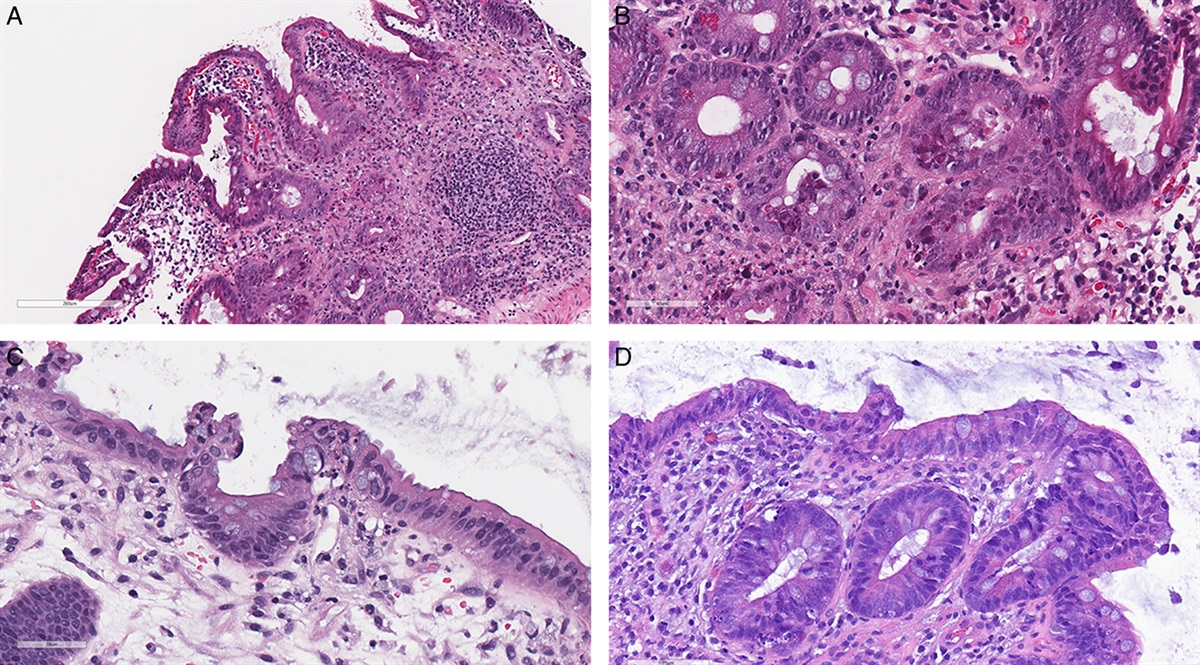
MM-H&N (Clinicopathologic Features and PRAME Expression)Thirty-six histologic samples from 23 patients were collected: 24 (66.72%) excisions of the primary tumor, 10 (27.8%) excisions of residual tumor/relapse, and 2 (5.5%) incisional biopsies, both followed by the surgical excision of the primary tumor. Fourteen (60.9%) patients were females and 9 (39.1%) males; the age at diagnosis ranged from 29 to 96 years (median value: 69.9 y). The most represented sites were the nasal cavity/nasal septum/turbinates (22, 40.7%) and palate (6, 16.7%). The most frequent histologic subtype was the nodular one (14, 60.9%), with a high percentage of cases showing ulceration (18, 78.3%) and prevalent epithelioid cytology (14, 60.9%). According to the eighth edition of the AJCC Cancer Staging Manual, the pT stages included 18 (78.3%) pT3, 4 (17.4%) pT4a, and 1 (4.3%) pT4b. MM-H&N were characterized by a diffuse (≥60% of neoplastic cells) nuclear expression of PRAME in 28 (77.8%) cases, and with a moderate/intense expression (intensity 2+ and 3+) in 20 (55.6%) (Figs. 3, 4). A single stain for PRAME was additionally performed in all cases of MM-H&N with <76% of PRAME-positive cells (negative according to Lezcano et al16) and the results were superimposable to those observed with double stain for Melan A/PRAME.35 The two incisional biopsies of MM-H&N were both positive only adopting the score of Raghavan et al30 (PRAME-positive cells: 70% and 65%, respectively). Noteworthy, both patients showed higher expression of PRAME (percentage of positive cells and/or intensity) in the subsequent surgical excisions resulting positive with all 3 tested scores.16,30,34 Two cases of MM-H&N were completely negative (0% of positive cells) for PRAME (Fig. 5), and both were located in the palate. In one of them, the negativity was probably related to the quality of the histologic sample (extensive necrosis and poor fixation).
 FIGURE 3:
FIGURE 3: PRAME expression in a case of mucosal lentiginous MM-H&N. The histologic examination shows the intraepithelial component (A, B: hematoxylin and eosin) nicely highlighted by nuclear PRAME stain (brown) (C: hematoxylin and eosin; D: PRAME), and so being potentially useful for the assessment of mucosal resection margins.
 FIGURE 4:
FIGURE 4: Two cases of nodular MM-H&N. Large and polypoid lesion (A: hematoxylin and eosin), with a nodular growth of atypical melanocytes (C: hematoxylin and eosin) diffusely positive for PRAME (brown nuclei) and Melan A (red cytoplasm) (E: PRAME). Highly fragmented sample of an ulcerated MM-H&N (B: hematoxylin and eosin) with a diffuse growth of atypical melanocytes (D: hematoxylin and eosin) diffusely positive for PRAME (brown nuclei) and Melan A (red cytoplasm) (F: PRAME).
 FIGURE 5:
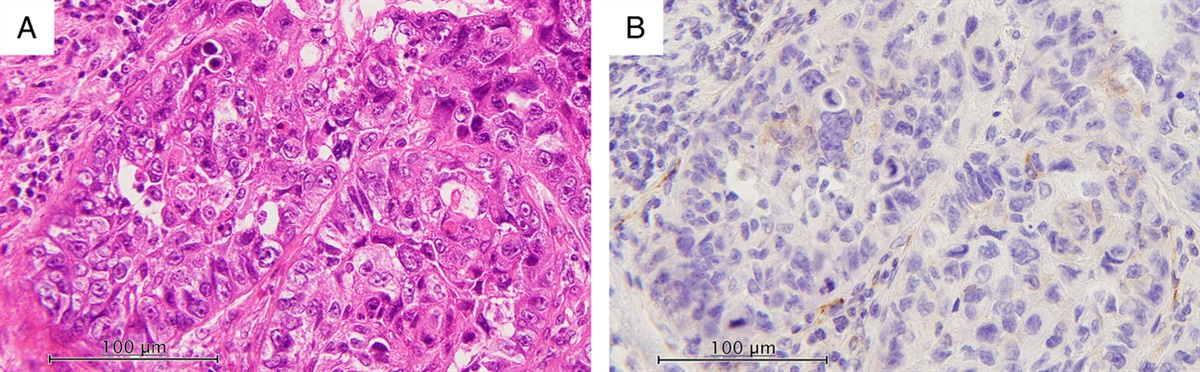
FIGURE 5: MBML-H&N: mucosal benign melanocytic lesions of the head and neck region; Negative PRAME expression in a case of mucosal lentiginous MM-H&N of the palate. The histologic examination shows a contiguous proliferation of atypical non-nested junctional melanocytes and irregular/dyschoesive nests at the dermoepidermal junction and in the superficial portion of the lamina propria, with marked epidermal effacement and diffuse pagetoid spread (A, C: hematoxylin and eosin). Double stain for Melan A/PRAME shows as the entire melanocytic population is PRAME-negative, with scattered positive fibroblasts as a positive control (B, D: hematoxylin and eosin).
Comparison of PRAME Scores for the Diagnosis of MBML-H&N and MM-H&NAll the tested scores16,30,34 showed SP and PPV of 100%, since no MBML-H&N turned out positive with any score. The score of Raghavan et al30 exhibited the highest values of SE, NPV, and AC: 77.8%, 69.2%, and 81.5%, respectively. The values of PRAME (percentage of positive cells and intensity) are summarized in Supplemental Digital Content 1 (https://links.lww.com/PAS/B522). The overview of PRAME results in MM-H&N and MBML-H&N, and the comparison between the 3 different scores are provided in Table 3; a graphical representation of MM-H&N and MBML-H&N cases distribution according to PRAME stain is shown in Figure 6.
TABLE 3 - The Overview of PRAME Results and the Comparison Between the 3 Different Scores for the Diagnosis of MBML-H&N and MM-H&N MBML-H&N, n/N (%) MM-H&N, n/N (%) Common nevus Blue nevus Melanotic macula All Mucosal lentiginous Nodular All Lezcano et al16 0, 1+, 2+, 3+ 2/2 (100) 6/6 (100) 10/10 (100) 18/18 (100) 8/16 (50) 3/20 (15) 11/36 (30.6) SE: 69.4%MM-H&N: mucosal melanoma of the head and neck region; MBML-H&N: mucosal benign melanocytic lesions of the head andneck region.
 FIGURE 6: Graphical representation of PRAME expression (% of positive cells and intensity) in MBML-H&N and MM-H&N. Each case corresponds to 2 bars, one for the % of PRAME-positive cells (green: MBML-H&N, pink: mucosal lentiginous MM-H&N, blue: nodular MM-H&N) and one for the intensity (orange bars). Fifteen cases showed 0% of PRAME-positive cells (13 MBML-H&N and 2 mucosal lentiginous MM-H&N; see the Results section and Fig. 5 for more explanations). Notably, the majority of MM-H&N below the cutoff of 60% of PRAME-positive cells (red dotted line) are mucosal lentiginous (only 1 case was nodular); all MBML-H&N show % of PRAME-positive cells below this threshold.Association Between PRAME Expression and Clinicopathologic Features
FIGURE 6: Graphical representation of PRAME expression (% of positive cells and intensity) in MBML-H&N and MM-H&N. Each case corresponds to 2 bars, one for the % of PRAME-positive cells (green: MBML-H&N, pink: mucosal lentiginous MM-H&N, blue: nodular MM-H&N) and one for the intensity (orange bars). Fifteen cases showed 0% of PRAME-positive cells (13 MBML-H&N and 2 mucosal lentiginous MM-H&N; see the Results section and Fig. 5 for more explanations). Notably, the majority of MM-H&N below the cutoff of 60% of PRAME-positive cells (red dotted line) are mucosal lentiginous (only 1 case was nodular); all MBML-H&N show % of PRAME-positive cells below this threshold.Association Between PRAME Expression and Clinicopathologic Features
Based on the obtained results, the cutoff of 60% of PRAME-positive cells (nuclear stain) was chosen to dichotomize MM-H&N cases in high (≥60%) and low (<60%) expression, and analyze the association of PRAME expression with the other dichotomous/categorical clinicopathologic features. Accordingly, high expression of PRAME was associated with female sex (21/23 [91.3%] vs. 7/13 [53.8%] in male sex, P=0.016) and nodular histologic subtype (19/20 [95%] vs. 9/16 [56.8%] in mucosal lentiginous one, P=0.005). Notably, although the mucosal lentiginous histotype showed lower rates of positivity, PRAME highlighted the intraepithelial component/growth, so being potentially useful for the appropriate evaluation of the mucosal resection margins (Fig. 3). High expression of PRAME was also significantly associated with specific anatomic sites (P<0.001), as follows: MM-H&N of the nasal cavity/nasal septum/turbinates showed high expression of PRAME in 20/22 (90.9%) cases, whereas MM-H&N of the palate in 0/6 (0%). Albeit affected by much fewer cases, all the cases of the nasopharynx (2/2, 100%) and the maxillary sinus (4/4, 100%) exhibited high expression of PRAME. No statistically significant association was found between high expression of PRAME and the other clinicopathologic features (type of histologic specimen, pigmentation, prevalent cytotype, ulceration, bone and/or cartilage infiltration, lymphovascular invasion, perineural infiltration, and pT stage) (Table 4).
TABLE 4 - The Association Between Clinicopathologic Features and PRAME Expression (Low: MM-H&N, samples (N=36), n (%) Low expression of PRAME (<60) High expression of PRAME (≥60) P Type of histologic specimen Excision of the primary tumor 7 (19.4) 17 (47.2) 0.349 Excision of residual tumor/relapse 1 (2.8) 9 (25) Incisional biopsy 0 (0) 2 (5.6) Sex Male 6 (16.7) 7 (19.4) 0.009 Female 2 (5.6) 21 (58.3) Site Nasal cavity/nasal septum/turbinates 2 (5.6) 20 (55.6) <0.001 Nasopharynx 0 (0) 2 (5.6) Palate (hard and soft) 6 (16.7) 0 (0) Maxillary sinus 0 (0) 4 (14.3) Tonsil 0 (0) 1 (2.8) Tongue 0 (0) 1 (2.8) Histologic subtype
留言 (0)