
記住我
Mycoplasma hominis (M. hominis) is one of the main opportunistic mycoplasmas in humans capable of causing disease. M. hominis mainly resides in the genitourinary tract and sometimes causes upper genitourinary tract infection [1, 2]. It can also cause epididymitis, cervicitis, pelvic inflammatory disease and puerperal fever. However, M. hominis is rarely detected in bloodstream infections or isolated from blood cultures [3]. The growth of the mycoplasma requires special growth medium, and the lack of cell wall makes it difficult to culture and identify by ordinary methods. Next-generation sequencing (NGS) is a powerful new technology to identify pathogens which were difficult by traditional methods. Here, we reported a case of M. hominis bloodstream infection in an ANCA-associated vasculitis patient with the help of NGS making a rapid diagnosis of M. hominis infection. Following the use of NGS, we extended the incubation time for the strain, successfully isolating the bacteria from anaerobic blood culture bottle, and further verified Mycoplasma hominis by of MALDI-TOF MS. Finally, the patient was treated successfully with a combination of levofloxacin, polymyxin B and meropenem.
Case presentationA 63-year old male was admitted to the hospital (the First Affiliated Hospital of Sun Yat sen University, Guangzhou, China) due to facial edema for 4 months and oral and nasal bleeding for 2 days. Laboratory examinations showed that creatinine 590 µmol/L (normal range 44–133 umol/L), autoantibody the neutrophil proteins leukocyte proteinase 3 (PR3-ANCA) positive, myeloperoxidase (MPO) positive, antinuclear antibody 1:320, and anti-double-stranded DNA (dsDNA) 42 IU/ml. Chest CT showed multiple lymph node enlargement and calcification in mediastinum and bilateral hilum, multiple bullae in the upper lobe of both lungs, bronchial mucus plug formation and swelling incomplete in bilateral lower lobes, pleural effusion in bilateral pleural and bilateral pleura slightly thickened. The patient was diagnosed as ANCA-associated vasculitis. ANCA-associated vasculitis (AAV) is a group of autoimmune diseases that involve inflammation and necrosis of small blood vessels, including microscopic polyangiitis, granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis), and eosinophilic granulomatosis with polyangiitis (formerly known as Churg-Strauss syndrome). These diseases can cause damage to multiple organs and tissues.The production of ANCA, which are autoantibodies targeting neutrophil cytoplasmic components such as PR3 and MPO [4].
On day 16 after admission, he developed hyperthermia (38 ℃) and left epistaxis. Laboratory examinations revealed leukocytosis (5.22 × 109/L, neutrophils 98.8%) with high serum C-reactive protein (44.21 mg/L,normal range 0–10 mg/L) and high procalcitonin level (2.25 ng/mL, normal range 0-0.5 ng/L). Haemoglobin (49 g/L, normal range 120–160 g/L)and platelet count (48 × 109/L, normal range 100-300 × 109/L) was decreased. Elevate IL-6 level was 21.43 pg/mL (normal range 0–5.3 pg/mL). Chest CT showed right bilateral pulmonary inflammation with significantly increased pleural effusion progression (Fig. 1). Blood cultures were obtained then and empirical antibiotics treatment with voriconazole (350 m g iv.drip Q12h), sulbactam (1 g iv Q8h) and imipenem (1000 m g iv.drip Q8h). Subsequently, both sets of anaerobic bottles for blood culture reported positive after 135 h, but the growth curves appeared flat. After Gram staining of blood smears, no bacteria were found (Fig. 2). After 24 h of incubation, no bacterial growth was found on the blood agar plate, and it was initially suspected to be false positive. However, after the next 7 days of antibiotics treatment, the patient’s body temperature did not decrease significantly. Antibiotics were adjusted to polymyxin B (1 million u iv.drip QD) and cefoperazone-sulbactam (1.5 g iv.drip Q12h).
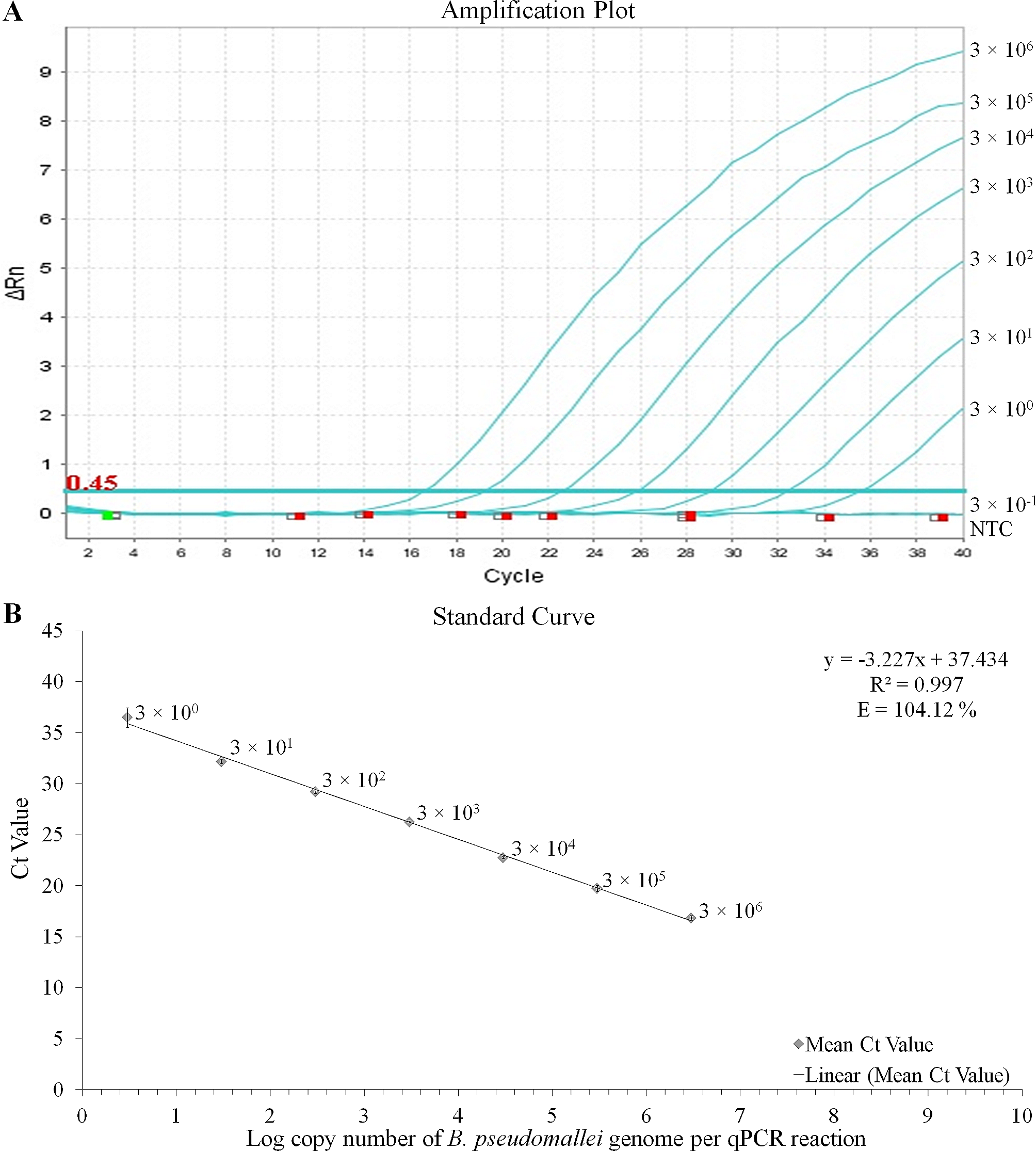
On Day 30, the patient suffered from epistaxis again. He displayed recurrent fever with the maximum temperature 38.3℃. Blood cultures were obtained again and metagenomic next generation sequencing (mNGS) for the peripheral blood specimen was performed. After sample processing and DNA extraction [QIAamp® UCP Pathogen DNA Kit (Qiagen)] for mNGS, libraries were constructed for the DNA samples using a Nextera XT DNA Library Prep Kit (Illumina, San Diego, America), sequencing was performed using Nextseq 550Dx sequencer (Illumina, San Diego, America). The rules of bioinformatic analysis for mNGS result and threshold criteria for interpretation of metagenomic analysis were referred to our previous process [5]. Within 48 h, the mNGS detected 19 total reads corresponding to Mycoplasma hominis, with 0.2% coverage and 4.6% relative abundance in bacteria (Table 1). Specifically, the total sequencing output was 32,513,857 reads, and 31,079,967 of them were valid sequences for analysis, with the host rate 98.13%. The accession number used for mapping of the reference genome is NZ_JRWZ01000004. The 0.2% mapping was covered by the sequence-specific to M. hominis and the confidence level was 99%. Meanwhile, both sets of anaerobic bottles for blood culture reported positive after 125.9 h, but the growth curves were still flat. After Gram staining of blood smears, no bacteria were found also. Based on the results of mNGS, we suspected that the pathogen of bloodstream infection was most likely Mycoplasma hominis, since it lacked cell wall and no bacteria was found under Gram staining. Therefore, we deliberately extended the incubation time of the strain. 48 h after incubation, needle—like colonies appeared on the blood-agar plate (Fig. 3). It was identified as Mycoplasma hominis by matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) (bio-Merieux, Durham, NC) (Fig. 4). To confirm the diagnosis, we performed qPCR analysis and Mycoplasma hominis was further confirmed (Fig. 5).
Based on these results, combination therapy with levofloxacin (500 mg P.O QD), polymyxin B (500 million u iv.drip Q12h), and meropenem (0.5 g iv Q8h) were used (Fig. 6). After treatment for 9 days, the patient’s infection was gradually controlled and body temperature returned to normal. The patient was discharged without further complications. During the three-month outpatient follow-up, no recurrence of symptoms or signs was reported.
Table 1 The micro-organisms were detected by NGS Fig. 1
The chest computed tomography imaging during disease progression. Compared with the chest computed tomography on admission day and Day 10 (A and B), the inflammation on Day 17 progressed significantly (C)
Fig. 2
(A) Anaerobic bottles of blood culture reported positive after 135 h, while the growth curves were flat. (B) No bacteria were found in Gram staining under microscope
Fig. 3
Needle-tip colonies appeared on the blood-agar plate 48 h after incubation
Fig. 4
It was identified as Mycoplasma hominis by matrix-assisted laser desorption ionization time-of-flight mass spectrometry
Fig. 5
qPCR analysis of the Mycoplasma hominiss. We have detected blood of the patient by quantitative polymerase chain reaction with specific primers (Forward primer: CCGTTCAAGCTACCCGAACA, reverse primer: AATGCAAGCCCTCAAGGAAA) for Mycoplasma hominis we designed, which indicated infection of Mycoplasma hominis. (The yellow and red line represented two replicate for blood of the patient. The green lines represented two replicate for negative template control.)
Fig. 6
Treatment timeline including changes of CRP, PCT, WBC, and etiology detection timepoints. (CRP, c-reactive protein; PCT, procalcitonin; WBC, white blood cell)
留言 (0)