
記住我
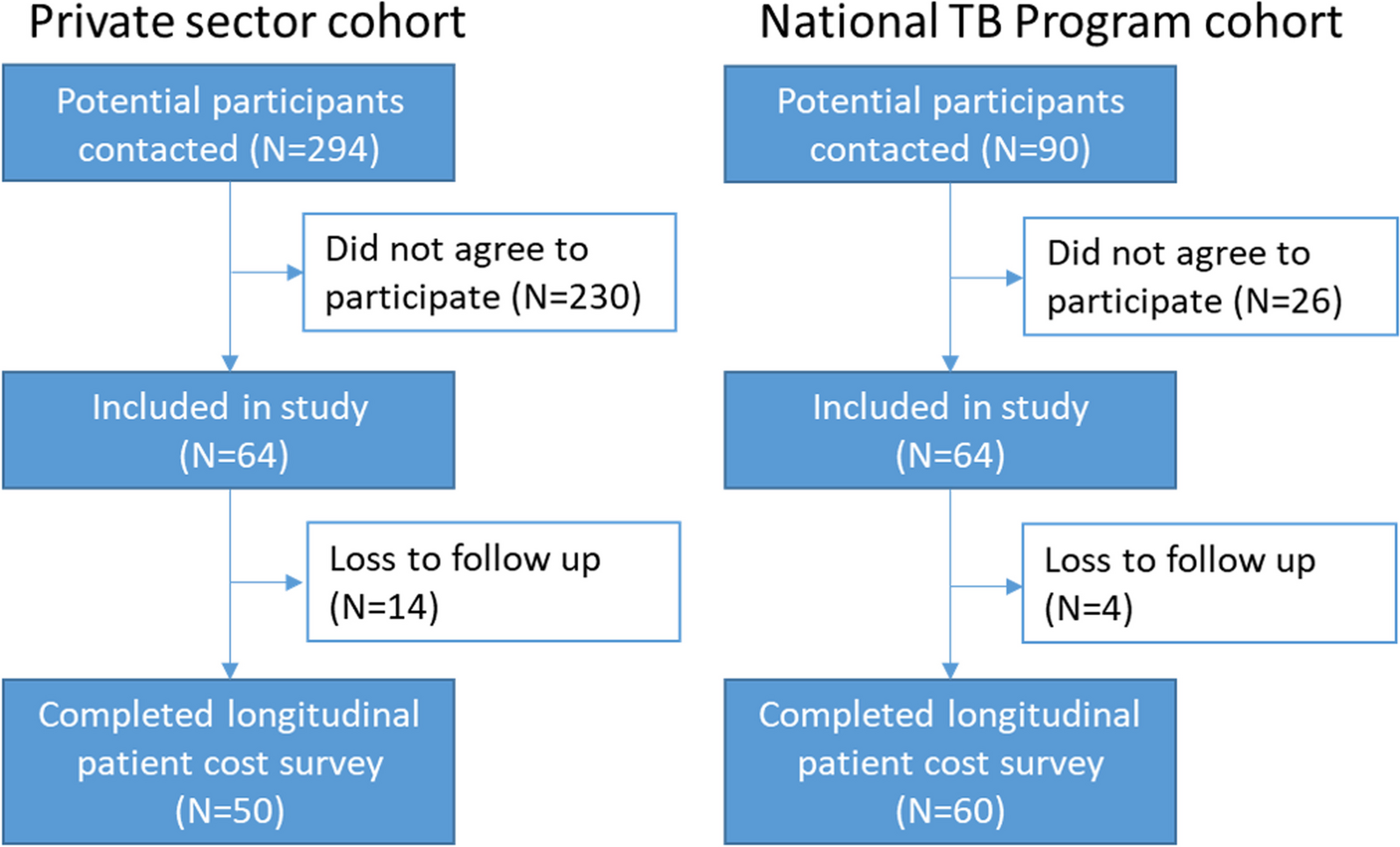


A total of 616 potentially relevant articles were identified, 12 of which met the inclusion criteria. (Fig. 1) [11, 14, 15, 21,22,23,24,25,26,27,28,29]. The characteristics of these studies are described in Table 1. All studies were conducted in high-income countries (eight studies in the USA [11, 14, 21, 24, 25, 27,28,29] and one study in England [26]) except for three studies from upper-middle-income countries (China, South Africa, and Turkey) [15, 22, 23]. Of the 12 articles in this review, one study included cost-effectiveness analysis (CEA) [23], 10 studies included cost-utility analysis (CUA) [11, 14, 15, 21, 22, 24, 26,27,28,29], and two studies included both CEA and CUA [25, 27]. Six studies conducted their economic analysis from the perspective of a health system [11, 21,22,23, 27, 28], five studies from a payer perspective [14, 15, 24,25,26], and three studies from the perspective of a health care provider [24, 25, 29].
Table 1 The characteristics of included studies in the present review Fig. 1
PRISMA flow chart for study selection. PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses
The costing year for three studies was not reported [21, 24, 26]. The time frames or study horizons adopted in the studies ranged from 30 days to a lifetime: three studies less than 1 year [22, 23, 29]; two studies one year [14, 21]; 6 studies a lifetime [11, 24,25,26,27,28]. In addition, one study was conducted in horizon time of a COVID-19 episode [15]. In the studies using discount rates, annual rates ranged from 3 to 5%.
The cost-effectiveness analysis in the US used willingness-to-pay (WTP) thresholds below USD 50,000 and USD 100,000 [11, 14, 22, 24, 25, 28]. The WTP threshold accepted by a Chinese study was USD 10,276 per QALY [22]. In England, Turkey, and South Africa, the WTP thresholds were GBP 20,000 per QALY, USD 8599 and USD 25,797 per QALY, and USD 3015 per DALY avoided and USD 36,000 per death avoided, respectively [15, 23, 26].
Results of quality assessment of economic evaluation studiesThe mean QHES score of the studies was 87.66. The maximum and minimum scores were 96 and 74.5, respectively (Table 2). All studies, except for one study [28], received a high-quality total score (total score < 75). The bar graph in Fig. 2 shows the percentage score for each criterion that all studies obtained. The total score in the criteria of subgroup analysis and the report of the funding source of the study were obtained for 100% of economic evaluations.
Table 2 Result of quality assessment of included studies Fig. 2
Results of quality assessment of the methodology of studies using the QHES checklist. QHES Quality of Health Economic Studies
Cost-effectiveness results of remdesivir compared with the standard of careThe costs and outcomes of the interventions are shown in Table 3. The results of an American study showed that considering the current price of remdesivir (USD 520 per vial) and the hypothesis of no effect of remdesivir on survival, this drug was not cost-effective in mild to severe COVID-19 patients. The incremental cost-effectiveness ratios (ICER) in this study for moderate to severe and mild COVID-19 patients were reported as USD 298,200 and USD 1,847,000 per QALY, respectively. The results of the deterministic sensitivity analysis in this study showed that three variables, including the survival related to remdesivir, the probability of death among patients receiving standard treatment, and the hospitalization cost of COVID-19 patients, affected the results of the study. In addition, the cost-effectiveness results varied with the change in the risk of death among patients treated with the standard of care [28]. The results of a study carried out in the UK showed that the use of remdesivir was cost-effective compared to the standard of care for the treatment of hospitalized patients with COVID-19, assuming the effect of remdesivir on reducing mortality (Cost-effectiveness ratio = GBP 11,881 per QALY). The results of probabilistic sensitivity analysis showed that remdesivir was cost-effective compared to standard treatment with a probability of 0.74. Furthermore, the results of the threshold analysis in this study indicated that when the survival risk ratio of remdesivir is greater than 0.915 (i.e. when no difference in survival between remdesivir and standard treatment is assumed), the price of each 100-mg vial of remdesivir should be less than GBP 18.6 so that remdesivir remains cost-effective. When assumed that remdesivir has no effect on reducing the mortality rate, it will have a small effect on increasing the quality of life. Moreover, 52% of the points of the probability simulation results will be in the northern quadrant (higher cost and greater effectiveness), and remdesivir will not be cost-effective at GBP 20,000 anymore. Furthermore, evidence showed that patients who require low-flow oxygen (LFO) are more likely to benefit from remdesivir compared to patients who require high-flow oxygen (HFO) or noninvasive ventilation (NIV) [26, 30]. Therefore, the administration of remdesivir to patients with LFO is cost-effective [26]. According to a study performed in Turkey, remdesivir use reduces hospitalization by 3 days compared with standard care. Low requirements for ventilators in treatment with remdesivir caused an increase in QALY compared to the standard of care. The difference in QALY in the investigated groups was estimated to be 0.174. The average cost of an episode for each patient in the remdesivir arm was USD 34,611.1, and in the standard of care arm, it was USD 3538.9. Remdesivir, compared to the standard of care, led to a shorter length of stay and less need for intubation among intensive care unit patients, and in patients with spo2 < 94%, who required oxygen support, it was the dominant option (higher QALY and lower costs) [15].
Table 3 Main cost-effectiveness resultsIn a study in China, the cost-effectiveness of 5-day remdesivir compared with the standard of care was examined among severe COVID-19 patients. The results of this study showed that the cost of treatment with remdesivir was CNY 97.93 million more than the standard of care. The ICER was CNY 14,098 per QALY, which was lower than China’s willingness-to-pay threshold. Daily severe cases of COVID-19 were 19% lower in the remdesivir treatment strategy than in the standard of care. The results of the study were robust to changes in the severity of the epidemic, modelling methods, and most of the model parameters. However, the results were relatively sensitive to changes in efficacy estimates [22]. Another study was conducted to investigate the cost-effectiveness of remdesivir compared to standard treatment with the decision tree technique from the perspective of the hospital. In this study, the ICER of the combination of remdesivir and the standard of care compared to the standard of care was estimated at USD 346,622, and remdesivir was not recognized as a cost-effective drug [29]. In an American study comparing the cost-effectiveness of pharmacological treatments for COVID-19, it was concluded that such drugs as remdesivir, casirivimab, imdevimab, dexamethasone, Baricitinib, and Tocilizumab were cost-effective compared to usual care, while treatments with Hydroxychloroquine, lopinavir-ritonavir, and interferon beta-1a were not cost-effective. Remdesivir was a dominant drug (lower cost and more effective) compared to conventional treatments, and the ICER of other drugs (casirivimab, imdevimab, etc.) was below the willingness-to-pay threshold, and they were cost-effective [11]. A study conducted in South Africa investigated the cost-effectiveness of remdesivir compared to the standard of care in non-ventilated patients and the cost-effectiveness of dexamethasone for non-ventilated and ventilated patients. The results of this study showed that remdesivir in non-ventilated patients and dexamethasone in ventilated patients prevented 408 deaths and saved 15 million dollars in costs. This result was due to the effectiveness of dexamethasone and the reduction of the required time in the ICU for patients treated with remdesivir. Compared to the standard of care, the use of remdesivir for non-ventilated patients and dexamethasone for ventilated patients would probably result in cost savings by reducing the ICU length of stay. Much uncertainty was observed in reducing the effectiveness and length of stay of remdesivir. Drug cost, cost per day of stay in the ICU, and mortality rate in the ICU were the most important influencing factors in the analysis of dexamethasone sensitivity in non-ventilated and ventilated patients [23].
In a study with a time horizon of one year and from the payer perspective in the United States, COVID-19 patients who required intubation and intensive care were classified as patients with severe COVID-19 and those requiring oxygen as patients with moderately severe COVID-19. Treatment strategies considered in this study included remdesivir for all patients, remdesivir for patients with only moderate and only severe infections, dexamethasone for all patients, dexamethasone for severe infections, remdesivir for moderate infections/dexamethasone for severe infections, and best supportive care. The results of this study showed that the use of dexamethasone was the most cost-effective strategy for all patients, with an ICER of USD 980.84 per QALY. However, the remdesivir treatment strategy was more expensive and less effective than other strategies. Dexamethasone was cost-effective for all patients in 98.3% of scenarios. Dexamethasone was the most cost-effective strategy for moderately severe infections. On the basis of the current data, remdesivir was unlikely to be a cost-effective treatment for COVID-19. The results of sensitivity analysis in this study showed that dexamethasone was cost-effective for all patients when the willingness-to-pay threshold was more than USD 1250 per QALY [14]. A study in the USA examined the cost-effectiveness of remdesivir and dexamethasone compared to the standard of care in hospitalized patients with COVID-19 in a time horizon of one year from the perspective of health care. The findings of this study showed that if the costs associated with remdesivir were only related to hospitalization costs, remdesivir was cost-effective (dominant). Dexamethasone was also cost-effective with an ICER of USD 5,208 per QALY, and the simultaneous use of remdesivir and dexamethasone was the most favourable strategy (dominant). If remdesivir had an effect on reducing the mortality rate, its usefulness (the number of lives saved) would be three times higher than base cases (hazard mortality ratio = 0.91). If health care costs were not related to the length of the patient’s hospitalization, remdesivir was not cost-effective with an ICER of USD 384,412.8 per QALY. Dexamethasone was also cost-effective if the cost-effectiveness ratio of life saved was USD 313.79. This study concluded that remdesivir and dexamethasone were cost-effective. The results of the deterministic sensitivity analysis of remdesivir compared to the standard of care also showed that the most important variable affecting the results was the rate ratio for time to recovery. In this study, the most cost-effective strategy as the dominant option compared to standard treatment was remdesivir, which had the greatest cost savings [21].
Cost-effectiveness results of the combination of remdesivir and baricitinib compared with remdesivir aloneThe results of a cost-effectiveness study comparing the combination of baricitinib and remdesivir with remdesivir alone in hospitalized patients with COVID-19 in the United States showed that in the long-term time horizon the combination of these two drugs was cost-effective (cost-effectiveness ratios = 22,334 per QALY and 17,858 per life year gained). In all hospitalized patients, the combination of baricitinib and remdesivir compared to remdesivir reduced the total hospital expenses by USD 1778 per patient and reimbursement by up to USD 1526, and it increased QALY by 0.0018 and survival in hospitalized patients by 2.7% [24]. The results of a cost-effectiveness study into adding baricitinib to the standard of care (systemic corticosteroids and remdesivir) in the United States showed that the addition of baricitinib led to a QALYs gain of 0.6703 and LYs gain of 0.837 compared to the standard of care. The addition of baricitinib increased survival by 5.1% and decreased the use of mechanical ventilation by 1.6%. The results of deterministic sensitivity analysis showed that the most important variables influencing the results of the study were lifetime health care costs among recovered patients, followed by progress towards mechanical ventilation during hospitalization. The results of probabilistic sensitivity analysis showed that on the willingness-to-pay threshold of USD 50,000 per QALY with a probability of 96.5%, adding baricitinib to the standard of care was cost-effective. [25].
留言 (0)