
記住我








Sixty-seven individuals who were diagnosed with lung cancer were enrolled. All of them had multiple 4D and 3D CBCT scans during the treatment. In total, 260 4D CBCT image datasets and 228 3D CBCT image datasets were collected.
Analysis of tumor volume during treatmentThe target area was outlined for 39 4D CBCT series, All tumors were delineated manually by two physicians with more than 5 years of clinical experience and reviewed by physicians on the same team with more than 20 years of clinical experience. The tumor volumes were calculated and compared.
(1)The mean tumor volume in this group was 38.63 mL (0.44 to 285.78 mL). Tumor volume response (TVR) was observed in 16 (41.0%) cases during the treatment.
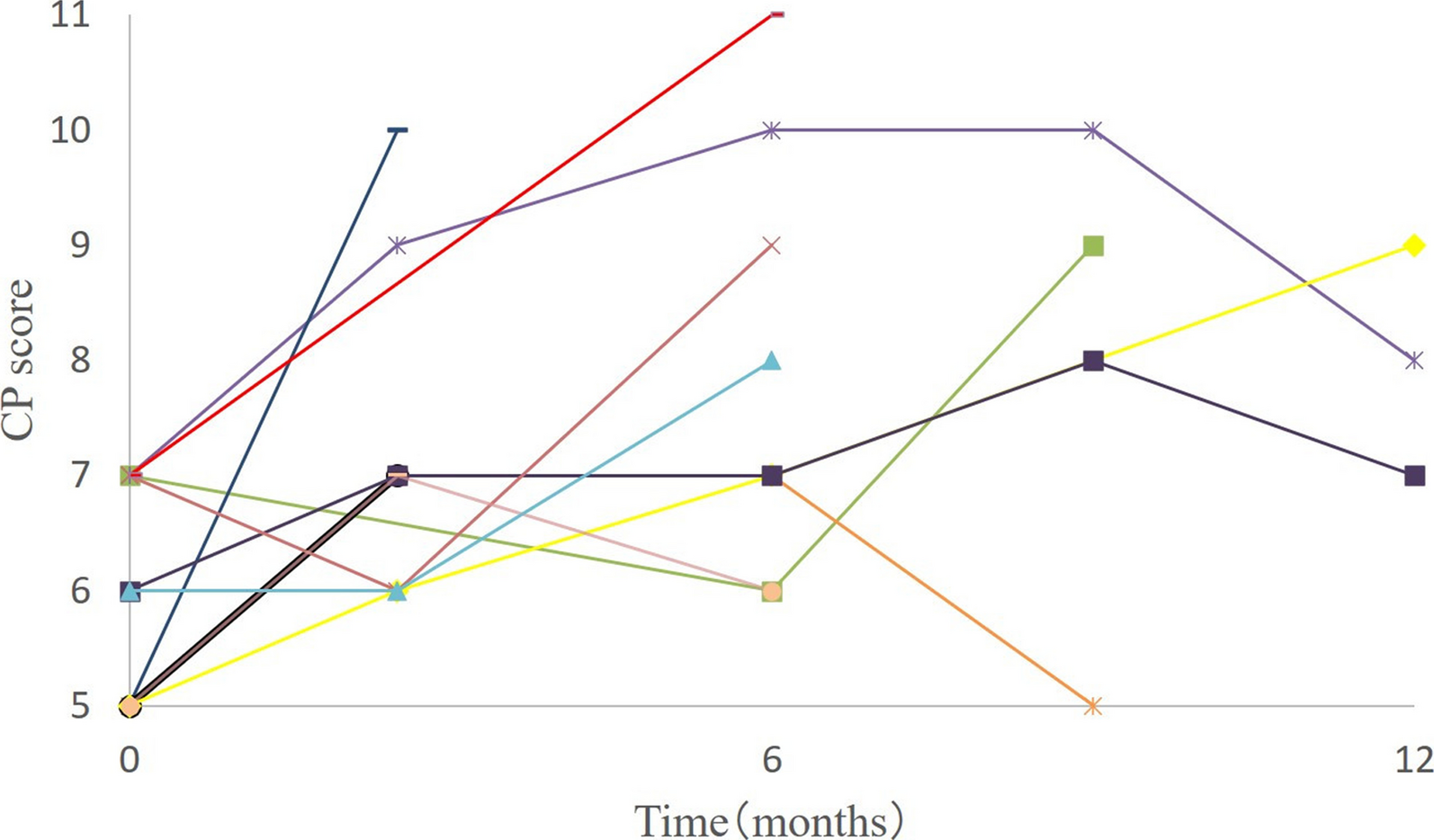
(2)Tumor volume change curves for each 4D CBCT in the patients with TVR are shown in Fig. 2. The mean tumor volume was 57.06 mL (0.56 to 285.78 mL) in this group and the mean volume reduction was 41.70% (17–77%),The average volume reduction was 23.79mL(9.7mL-43.9mL). TVR was usually observed within the first 3 weeks, with a median time to response of 19 days (3 to 40 days).
Fig. 2
Dynamic change of target volume in 16 patients with tumor volume reduction. The median time to observed tumor volume response was 19 days (3 to 40 days)
Analysis of tumor motion during treatment (1)In the initial 4D CBCT validation, tumor motion could be traced along three axes in 64 cases (Table 2), of which 13 (20%) were volume reduced and 3 (5%) were near the diaphragm. The X-axis is left-right,the Y-axis is superior-inferior, the Z-axis is anterior-posterior.
(2)The mean value of the maximum difference in motion (the difference between the maximum and minimum motion) along the Y-axis was 0.24 cm (0.00 to 1.34 cm). In 16 cases (25%), the maximum difference was > 0.20 cm and the mean value of the maximum difference was 0.52 cm (0.22 to 1.34 cm) in these cases.
(3)Tumor motion decreased in 10 cases and increased in 3 cases. The median time to maximum motion was 13 days after the first irradiation (5 to 40 days).
(4)Three of the 6 lesions near the diaphragm demonstrated fluctuating tumor motion (0.28, 0.33, and 0.66 cm) with stable tumor volumes.
Table 2 Tumor motion along three axes (N = 64)Tumor motion was observed in all directions, mostly during the first 3 weeks of treatment; the most movement was measured along the Y-axis, in volume-reduced patients, and in the lesions near the diaphragm, which may show greater motion regardless of volume changes.
Analysis of tumor center coordinatesThe geometric center of the tumor was identified by outlining the target area in 39 4D CBCT images and determining the coordinates of the geometric center. The tumor center was calibrated by using 4D CBCT grayscale + manual registration data.
(1)The average range of motion of geometric centers was 0.25 cm (0.03 to 1.44 cm) on the X-axis, 0.28 cm (0.03 to 2.50 cm) on the Y-axis, and 0.22 cm (0.01 to 0.73 cm) on the Z-axis.
(2)Among 39 lesions, those with a range of motion < 0.5 mm were defined as centrally stable (N = 22) and those with a range of motion ≥ 2.5 mm as unstable (N = 17). The result of a univariate analysis of the mean tumor volume, tumor motion, and patient BMI in these two groups is shown in Table 3.
Table 3 Univariate analysis of factors influencing central stability (N = 39)Tumor volume was found to be an independent factor affecting central stability (P = 0.008), and central stability was worst in patients with large volumes and a range of motion ≥ 2.5 mm. There was no statistical difference in range of tumor motion and body mass index between the two groups (P > 0.05)
Registration with planning 4DCT and data analysis Setup error1: Comparison of 4DCBCT bone-based registration and grayscale + manual registrationPatients (N = 67) were divided into a small error group (N = 39) and a large error group (N = 28); large error was present when the deviation between bone registration and 4D grayscale + manual registration was > 0.5 cm. Grayscale + manual registration was defined according to gray-based automatic registration with 4DCT and adjusted by the radiotherapist based on soft tissue(mainly the primary tumor).Univariate analysis of mean tumor volume, motion, and BMI was performed for both groups (Table 4).
Table 4 Factors influencing the error of four-dimensional cone beam computed tomography bone- based registration and grayscale + manual registration (1)Tumor motion was the most influential factor in the difference between the two registration methods (P < 0.05); tumor motion was > 1 cm in the large error group.
(2)Upon further analysis of the effect of tumor motion on registration errors, the partial volume off-target rate was 41.8% if based on bone registration only, 19.0% when the motion was ≤ 0.5 cm, and 52.2% when the motion was > 0.5 cm.
Setup error2: Comparison of 4DCBCT grayscale + manual registration and average intensity projection(AIP) of 4DCBCT grayscale + manual registrationTwo sets of registration data were obtained: 4D grayscale + manual registration and AIP of 4DCBCT grayscale + manual registration. In 260 sets of 4D CBCT images, the margin of error was < 0.5 cm in three axes. There were only four occasions out of 260 (1.5%) where the registration verification process demonstrated and error of ≥ 0.30 cm (0.30 to 0.34 cm).The frequency of errors in each axis is shown in Table 5. There was no difference between the 4D CBCT grayscale + manual registration and AIP of 4DCBCT grayscale + manual registration.
Table 5 Registration errors in 4DCBCT grayscale + manual registration and AIP of 4DCBCT grayscale + manual registration Setup error3: Comparison of 4DCBCT grayscale + manual registration and 3DCBCT grayscale + manual registrationBecause of the constraints of facility resources, patient treatment time, and radiation exposure, our trial used alternating 4D and 3D CBCT validation, which can reduce machine depreciation, decrease the chance of malfunction, reduce patient treatment time and the potential for movement during prolonged treatment, and limit the risk of excessive X-ray irradiation. However, setup errors, baseline differences, tumor volume, location, and motion changes may influence differences between the two methods of registration. Therefore, the 4D and 3D CBCT validation data were analyzed by excluding cases with significant tumor volume, motion changes, and unstable tumor centers. In the end, 21 cases were eligible for analysis. The bone registration data were subtracted from 4D and 3D CBCT grayscale + manual registration data to eliminate the influence of setup errors. When the two groups of data were compared, no difference was found in the 4D and 3D CBCT registration data of 14 cases on each axis, with 10 cases (71.4%) having tumors adjacent to the chest wall, mediastinum, or vertebral body. In 7 cases, there was a difference between the two kinds of registration (X-axis, 5 cases; Y-axis, 2 cases). Among these, the tumor was adjacent to the chest wall, mediastinum, or vertebral body in 3 cases (42.9%) (P = 0.296). Because of the relatively rigid anatomical reference, there was no difference between 4D CBCT and 3D CBCT registration when the tumor was adjacent to the chest wall, mediastinum, or vertebral body.
留言 (0)