A multi-center institution-based cross-sectional study was carried out among patients with ESRD undergoing hemodialysis in both governmental and private hospitals/dialysis centers in Addis Ababa, Ethiopia. The study demonstrated that patients undergoing hemodialysis rated their HRQOL as poor. Several socio-demographic and clinical characteristics of hemodialysis patients were found to be associated with both generic and kidney disease-related components of HRQOL.
The average age of the patients in our study (45 years) was broadly comparable to that of patients undergoing hemodialysis in other African countries [17, 32] and close to the mean age of patients in south-Asian countries [44, 45]. This could be explained by the fact that, in Sub-Saharan Africa and Asia, ESRD affects younger populations due to the influence of established risk factors, such as diabetes, hypertension and kidney infection [46, 47]. In support of this explanation, our data showed that 67% and 76% of diabetes and hypertensive patients, respectively, were younger than 60 years of age.
Our results showed that patients undergoing hemodialysis in Ethiopia struggle with poor physical and mental health (subscales PCS and MCS, respectively). This is in line with previous reports [30,31,32, 34, 48,49,50]; however, our mean scores (PCS and the MCS) were slightly lower than most other studies when taking the confidence intervals into account. A study from Malawi [32] with a small sample (n = 22) found higher scores of both PCS and MCS, and a single center study carried out in Colombia [30] reported higher ratings of PCS. Additionally, a large study from the US [25] reported better physical and mental health in a large sample of patients with all types of dialysis (in center hemodialysis, peritoneal dialysis, home hemodialysis, and nocturnal dialysis). Differences in sampling strategies, sample size, and response rates limit the possibility to conclude that our results are worse than previously reported. Our results underscore that this group of patients not only have serious limitations regarding physical health, but also mental health issues that merit concern.
Regarding the kidney disease-targeted part of the instrument, the BKD subscale was rated low, indicating that patients on maintenance hemodialysis experienced a huge disease burden. This finding is in line with two previous studies conducted in Ethiopia and Malawi but higher compared to a study performed in Kenya [49]. Our results were lower reflecting more frustration and interference, than those from the US, Europe (France, Germany, Italy, Spain, and the United Kingdom), and Japan [25, 48] or those studies performed in Colombia and Egypt [30, 31]. A possible explanation of this discrepancy might be related to differences in healthcare systems. The healthcare system in Ethiopia requires lengthy procedures and numerous diagnostic tests, which may frustrate the patient. In addition, restrictions on mobility, daily activities, and the risk of losing one’s job due to dialysis therapy can result in a feeling of frustration and cause dialysis patients to perceive themselves to be a burden on their families. “Itchy skin (pruritus)”, “fainting or dizziness” and feeling “washed out or drained” were the most prevalent symptoms recorded in the SPKD subscale. These symptoms have been previously reported in systematic reviews [51, 52]. Additionally, in support of this observation, a US study reported the negative effects of pruritus on the HRQOL of patients on maintenance hemodialysis beyond the discomfort caused by the condition [53].
Patients’ ratings of effects of the disease, as measured with the subscale EKD, reached a similar level as a study performed in Colombia [30]. However, it is lower than the scores reported by other studies conducted in different parts of the world [31, 32, 34, 48, 54]. Hemodialysis patients must visit medical facilities three times a week for a total of three to five hours; this interferes with their ability to carry out their daily lives independently including work which may contribute to low HRQOL.
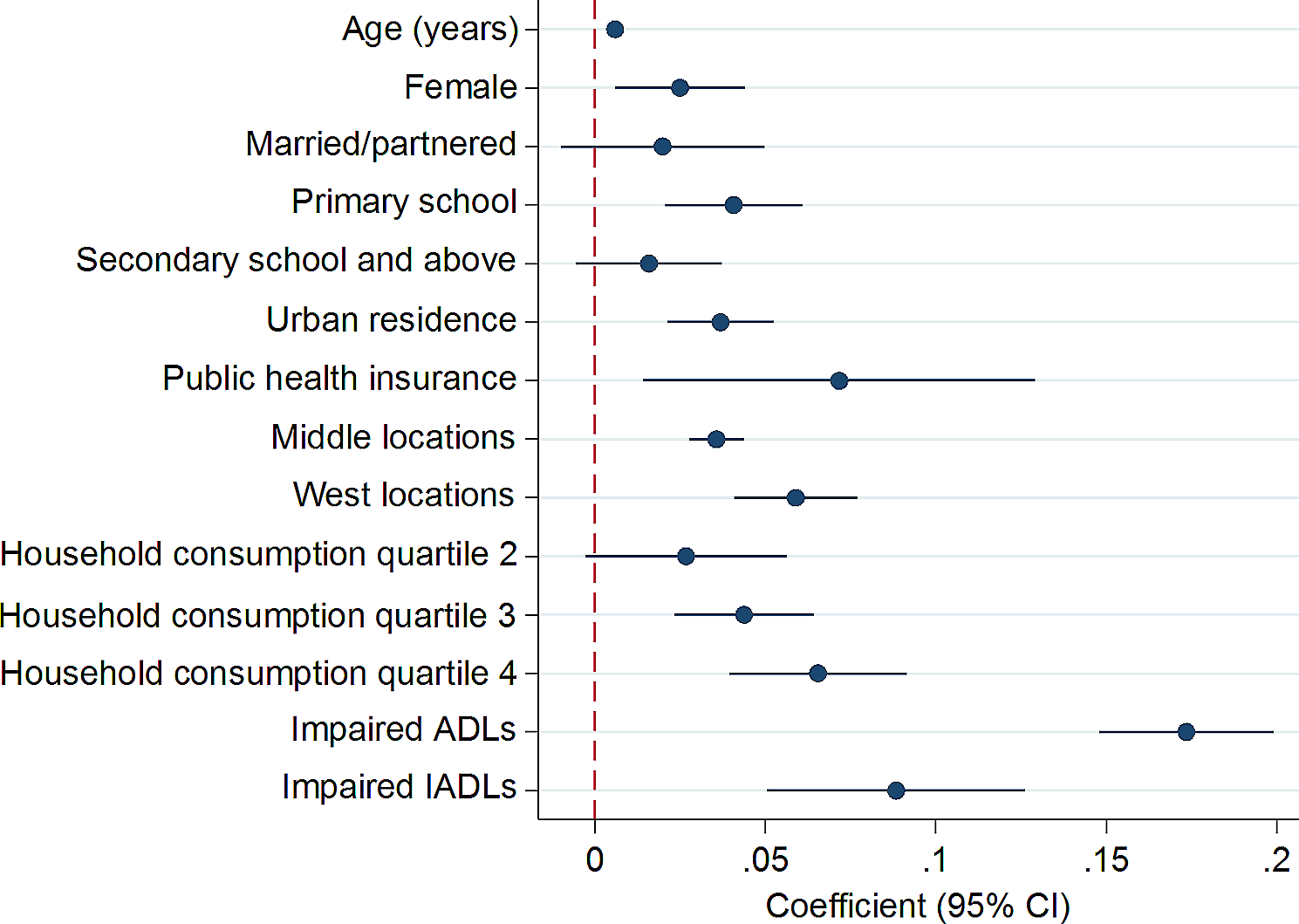
Our findings demonstrated that mean PCS and EKD scores decrease as age increases. This finding is supported by previous studies [27, 28, 31, 55] and may be explained by the reduced physical function, strength, energy and self-care ability of elderly patients that occurs with increased age. Complications including heart disease, anemia, high blood pressure, pulmonary edema, and decreased immune response that leads to infection, are also more likely to occur as age increases, which in turn increases pain and leads to further declines in energy and physical functioning [28]. Conversely, the shorter disease duration among younger patients might explain their higher HRQOL scores.
Female sex was associated with lower ratings of mental health (MCS), in line with previous reports [27, 28, 31]. This could be explained by the various roles women play in society that contribute to physical and mental stress, which have a significantly negative influence on the HRQOL of CKD patients [56]. This finding draws attention to the need to support women, who have more roles and responsibilities at home. Thus, a multidisciplinary team of nephrologists, nurses, social workers, and psychologists must work together to support patients undergoing hemodialysis; particularly women.
Consistent with previous studies [27, 28, 31], our data showed that participants with a higher educational levels scored their physical health (PCS) as better and perceived fewer burdens and effects of their kidney disease. This might be because higher education enhances individuals’ understanding of the value and importance of hemodialysis. In addition, higher educational levels are usually associated with higher income and the ability to afford treatment costs, which improves HRQOL.
Technically, patients’ HRQOL is supposed to improve with more frequent dialysis treatments; however, the opposite was found to be true in this study. This study demonstrated that attending hemodialysis sessions three times a week—which is the standard recommendation—was associated with poorer ratings of physical health (PCS subscale). A similar result was found in a Brazilian study [57], which found that attending hemodialysis sessions was associated with a higher prevalence of symptoms, worsening burdens of kidney disease, and lower PCS scores. Similarly, AlSalmi et al. reported that the HRQOL scores of hemodialysis patients decreased with increasing dialysis frequency [58]. This may be due to the patients’ health condition; severely ill patients may undergo hemodialysis three times a week.
The current study showed a positive relationship between adherence to medication and HRQOL with regard to the EKD subscale, consistent with previous findings [59]. This may indicate that non-adherence to medication prevents ESRD patients from gaining the full benefits of the prescribed medications, which has been associated with increased mortality and hospitalisation, leading to poorer HRQOL [60]. The health care team working in the dialysis unit should emphasise health education and counselling regarding medication adherence to improve patients’ HRQOL.
Social support plays a significant role in improving the HRQOL of hemodialysis patients. In line with other studies, we found that having social support was associated with better HRQOL regarding physical health [61,62,63]. Dialysis treatment should consider the role of family members’, friends’, and neighbors’ participation by welcoming relatives and inviting family members to the dialysis unit. Additionally, due to the gaps they may fill in patients’ support requirements and the shared experiences of the group members, support groups that include patient’s relatives may prove helpful.
In the present study, normal or high BMI were associated with better HRQOL in all domains. About 20% of the respondents had a BMI > 24 kg/m2, which is the recommended BMI for hemodialysis patients [64]. Similarly, Kalantar-Zadeh et al. reported that a higher BMI was protective against cardiovascular disease among hemodialysis patients, in contrast to the general healthy population [65]. This may decrease the risk of having a cardiovascular comorbidity, which in turn contributes to better HRQOL for the patient. Healthcare professionals working in the dialysis unit should be aware of the recommended BMI for ESRD patients undergoing hemodialysis and provide counselling, as needed, to help them maintain it.
The duration of hemodialysis treatment had a significant impact on patients’ HRQOL. According to this study, a duration of one year and above was associated with low SPKD and EKD scores, which is consistent with a previous study [66]. A similar observation was also made by a group in the US, who found that patients who had been on hemodialysis for a longer duration had lower functional status, more hospital readmissions, and worse HRQOL [56]. This is likely explained by the negative feelings brought by the lifelong nature of the treatment, monotonous living, feeling exhausted and fed up, and an inability to deal with the symptoms of dialysis [54]. Thus, as the duration of hemodialysis increases, patients will continue to experience these adverse effects, which may lower their HRQOL.
Strengths and limitations
The present study has several strengths. First, it assessed HRQOL using a standardized measure (KDQOL-36) that has been used extensively around the world and validated in Ethiopian patients with ESRD, allowing for comparisons with data from other settings. Second, to the best of our knowledge, this study had the largest sample size (481 participants) in sub-Saharan Africa, including both private and governmental facilities, where the cost of hemodialysis varies greatly. This study has limitations. As it is a cross-sectional study, causal inferences cannot be made between HRQOL and the independent variables. Data were collected through face-to-face interviews, which might have introduced interviewer and social desirability bias into the results. Another limitation could be the use of an already-changed terminology (“ESRD” changed to “kidney failure”) for the purpose of continuity with our previous work.









留言 (0)