Patient population
The medical records of patients with pulmonary metastatic lesions of sarcoma treated with SBRT at two institutions (Seoul National University Hospital and Korea Cancer Center Hospital) between January 2011 and December 2021 were retrospectively reviewed. Cases of pulmonary metastasis of carcinoma with sarcomatoid change or sarcomatoid features, metastasis from a primary site of soft tissue that was not of mesenchymal cell origin, and tumors without follow-up computed tomography (CT) scans were excluded from the study. A total of 71 pulmonary metastatic lesions from 39 patients treated with SBRT were eligible.
Treatment
Patients with pulmonary metastasis of sarcoma were referred by treating surgeons or medical oncologists to the radiation oncology department for local ablation of metastatic tumors. There were three categories of indications for SBRT: (1) Oligometastasis, defined as a limited number (≤ 5) of metastatic lesions at diagnosis or recurrence; (2) Oligoprogression, defined as a limited number (≤ 5) of metastatic lesions that progressed or did not respond during systemic therapy or within 6 months after the completion of systemic therapy; (3) Palliation, defined as metastatic disease that is not under systemic therapy, with numerous active metastatic lesions, and some rapidly progressive tumors that require local treatment. The treating radiation oncologist re-evaluated the feasibility of SBRT for pulmonary lesions and determined the necessity of treating such lung nodules.
For radiation therapy planning, CT-based simulation was performed. The patient was placed in a supine position with both arms abducted, using a wing board and vacuum cushions for immobilization. An abdominal compression plate was used to limit the movement of the diaphragm during breathing. For metastatic nodules located in the lung apex, the patient was placed in a supine position with both arms adducted and immobilized using thermoplastic aquaplast. Four-dimensional CT was performed to generate CT images for each respiratory phase. The internal target volume (ITV) was delineated by the radiation oncologist based on these CT images, taken at different respiratory phases. The planning target volume (PTV) was generated by expanding the ITV by 3–7 mm. The prescribed dose and fractionation were determined by the radiation oncologist, taking into account the indication for SBRT, proximity of the lung nodules to critical mediastinal structures, and the patient’s baseline lung function.
The radiation dose was delivered to patients using various devices. Radiation therapy was delivered mainly using TrueBeam and Clinac iX (Varian Medical Systems Inc., Palo Alto, CA, USA). Volumetric modulated arch therapy was applied for radiation therapy planning and beam delivery using these devices. For patients with large respiratory motion, treatment was delivered using MRIdian (ViewRay Inc., Oakwood Village, OH, USA), a device that utilizes magnetic resonance imaging-based gating. For patients with limited lung function and appropriate for tracking gold fiducial markers, treatment was delivered using CyberKnife (Accuray Inc., Sunnyvale, CA, USA). Volume-based prescriptions were used for radiation dose prescriptions in all four devices. For CyberKnife, the dose was prescribed to the 75% isodose line, and the maximum dose reached around 130% of the prescribed dose. For the other devices, the plan was optimized to cover 95% of the PTV by 100% of prescribed dose, and the maximum dose was limited to around 110% of the prescribed dose. Each fraction was delivered two or three times per week without consecutive daily treatment. Treatment of multiple pulmonary lesions varied based on their proximity to one another. When lung nodules were far apart, each one was treated with an individual plan, which were delivered either on the same day, on alternate days, or consecutively. Lesions close to each other were treated with a single isocenter plan.
Endpoints and statistics
The primary endpoint of this study was local control per tumor (LCpT). An event of LCpT was defined as regrowth of the treated tumor or the formation of new lesions inside the PTV. LCpT was measured from the start of SBRT to the lesion, and calculated using the Kaplan-Meier method for each pulmonary metastatic tumor. The biologically effective dose with an α/β ratio of 10 (BED10) was calculated for each lung tumor using the following equation:
$$}_} = nd\left( }} \right)$$
where n is the number of fractions, d is the dose per fraction in Gy, and α/β is the dose at which the linear and quadratic portions of cell killing are equal in the linear-quadratic model. Prescribed dose was used for the calculation of BED10. Treated lung tumors were categorized into two groups: a low BED10 group, defined by BED10 < 100 Gy, and a high BED10 group, defined as BED10 ≥ 100 Gy. Although there were reports with lower α/β ratios for sarcoma [13,14,15], an α/β ratio of 10 and a BED10 cutoff value of 100 Gy were chosen based on previous literature for SBRT for primary lung tumors and metastatic lung tumors [16, 17]. Comparison of LCpT between the two groups was performed using a log-rank test. The centrality of treated lung nodules was defined in two ways: using conventional Radiation Therapy Oncology Group criteria, which defined a central nodule as a location within 2 cm from the proximal bronchial tree[18], and by abutment to the mediastinal structures such as the heart, great vessels, and trachea. The response of the treated lesion at the last follow-up was evaluated per tumor based on the Response Evaluation Criteria in Solid Tumors.
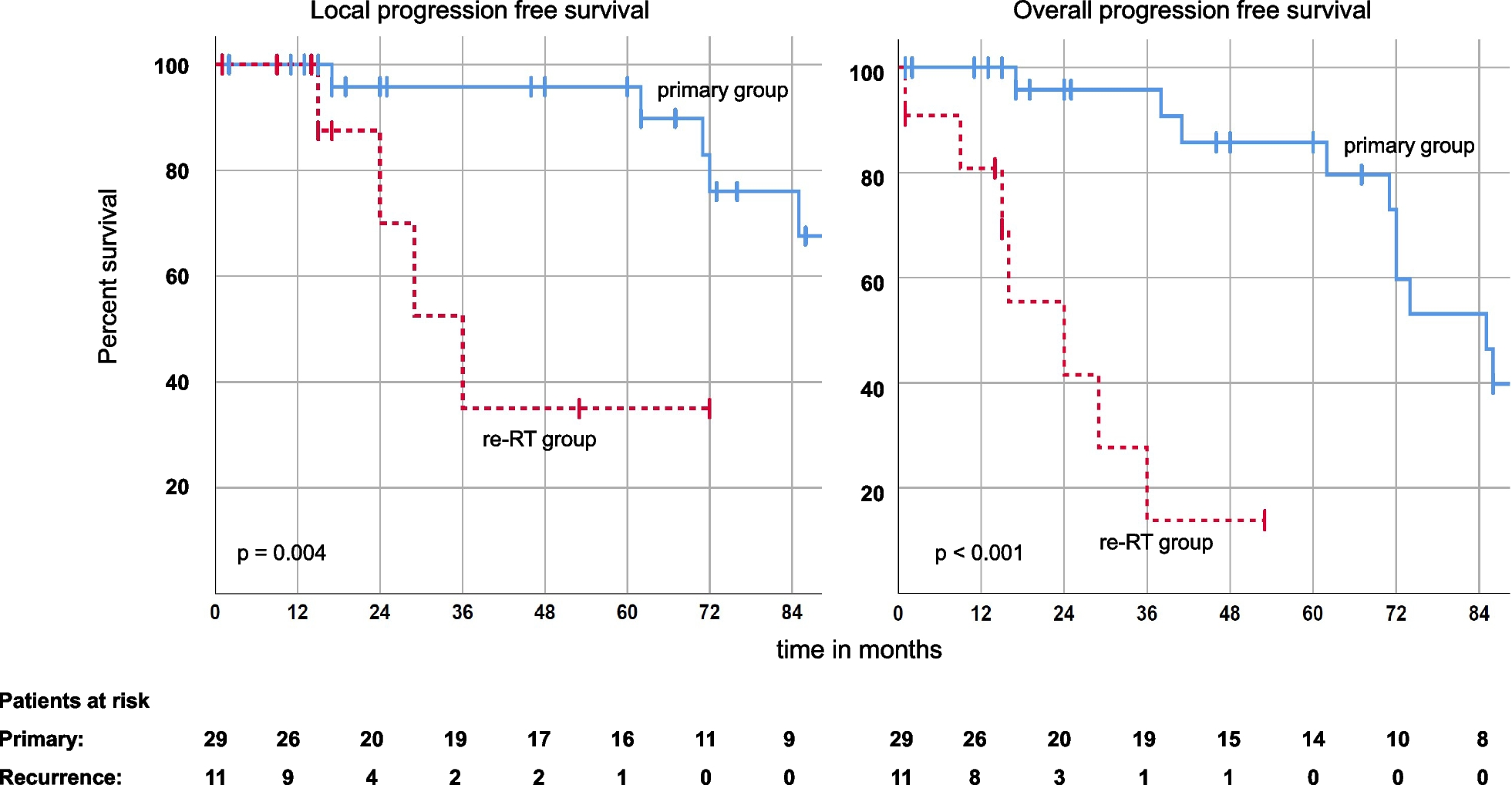
The observed clinical outcomes per patient were local control per patient (LCpP), pulmonary progression-free rate (PPFR), any progression-free rate (APFR), and overall survival (OS). An event for LCpP was defined as any LCpT event for lesions treated with SBRT for the patient. An event for PPFR was defined as the progression of any metastatic lesions in the lung. An event for APFR was defined as the progression of any intra- and extra-thoracic metastatic lesions. An event for OS was defined as the death of the patient from any cause. These clinical outcomes per patient were measured from the start of the first SBRT session and calculated using the Kaplan-Meier method. Comparison of these clinical outcomes between the two groups was not possible as some patients with multiple pulmonary metastatic lesions underwent simultaneous SBRT sessions with different BED10.
Univariate analyses were performed on LCpT, LCpP, PPFR, APFR, and OS to search for variables associated with corresponding endpoints. The Cox proportional hazards model was used for the univariate analysis. When no event occurred with a specific variable, the hazard ratio could not be derived, and the p-value was calculated using the log-rank test instead. Multivariate analysis was not performed due to a low number of cases and events. SBRT-related adverse events were graded using the Common Terminology Criteria for Adverse Events version 5, and severe (grade ≥ 3) adverse events were reported. Student’s t-test was used for the comparison of continuous variables, and chi-square test with or without Yate’s continuity correction was used for the comparison of categorical variables. A p-value less than 0.05 was defined as statistically significant. All statistical analyses were performed using R 4.2.1 (The R Foundation for Statistical Computing, Vienna, Austria).








留言 (0)